Daycare, Tubeless, Supine Percutaneous Nephrolithotomy under Spinal Anesthesia for Large Stone in a Patient with Multiple Comorbidities
Daycare PCNL was first reported in 1986. However due to the major concern regarding patient safety, it was not widely adopted as a routine procedure. A 63-year-old male with multiple comorbidities underwent right-sided tubeless, supine positioned, daycare percutaneous nephrolithotomy while under spinal anesthesia, due to partially staghorn stone. The patient was discharged in the 9th post-operative hour with no complications. Daycare PCNL is a safe and effective procedure in selected patients and may have a role in patients with a larger stone burdens and ASA III patients.
Introduction
Prone Percutaneous nephrolithotomy (PCNL) was first described by Fernstrom and Johansson in 1976 [1], and supine PCNL was first described by Valdivia in 1987 [2]. Currently, both are an accepted choice of treatment for renal stones with diameter larger than 2 cm [3]. Daycare PCNL was first reported in 1986 [4]. Due to a major concern regarding patient safety, it was not widely practiced as a routine procedure. However, as equipment technology advances, scope sizes decrease and the higher-powered lasers have been used, the daycare PCNLs remerge as an option for selected patients.
In the current report, we present a case of a 63-year-old male with multiple comorbidities, who underwent tubeless, supine, daycare PCNL while under spinal anesthesia. The patient provided informed consent to publish his case details and any accompanying images.
Case Report
A 63-year-old male patient was referred to the urology clinic because of an incidental finding of bilateral staghorn renal stones. He had a history of left pyelolithotomy in 2003.
Furthermore, the patient has a history of insulin- controlled type-2 diabetes mellitus, hypertension, and ischemic heart disease. He underwent Percutaneous Coronary Intervention (PCI) in May 2016, and Coronary Artery Bypass Grafting (CABG) in December 2016.
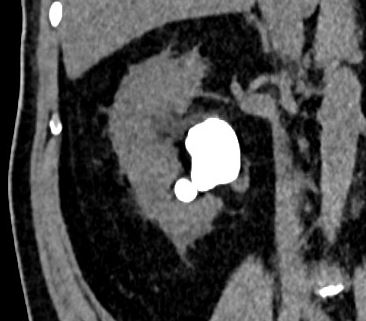
The patients Computed Tomography (CT) scan revealed one large stone (31 mm x 25mm x 14 mm = 16523mm3) in the right renal pelvis and another smaller stone (16 mm x 15 mm x 12 mm = 1497 mm3) with total volume 18021 mm3 and 1350 Hounsfield Unit (HU) (Figure 1). In the left kidney there was a staghorn stone with cumulative volume 47 mm x 28 mm x 37 mm = 25404 mm3 and 1100 HU (Figure 1).
The preoperative laboratory investigations were as follows: hemoglobin 12 g/dL, creatinine 96 umol/L, urine microscopy 71 WBC/HPF, urine culture showed insignificant growth. Aspirin 100 mg was stopped one week before the surgery.
In spite of that the bilateral stones were incidentally diagnosed, the patient had discomfort in the right side, therefore he was counseled for right supine PCNL under spinal anesthesia (Figure 2). Four mL (15 mg) 5% bupivacaine was given intrathecally. Two-gram ceftriaxone was given on anesthesia induction.

The posterior axillary line, the XII rib and the iliac crest were marked before positioning the patient to have the exact marking. The patient was put in Galdakao Valdivia-modified supine position (GVMS) (Figure 3).

The right leg was on extension, the left leg was on flexion. The right gluteal area and right side of the back were elevated to ensure around 25o tilting to the left side. The right flank area, the abdomen and the genitalia were disinfected and draped as one area.
22Fr cystoscope inserted into the bladder, a ureteric catheter was pushed to the renal pelvis of the right kidney over a sensor guidewire.
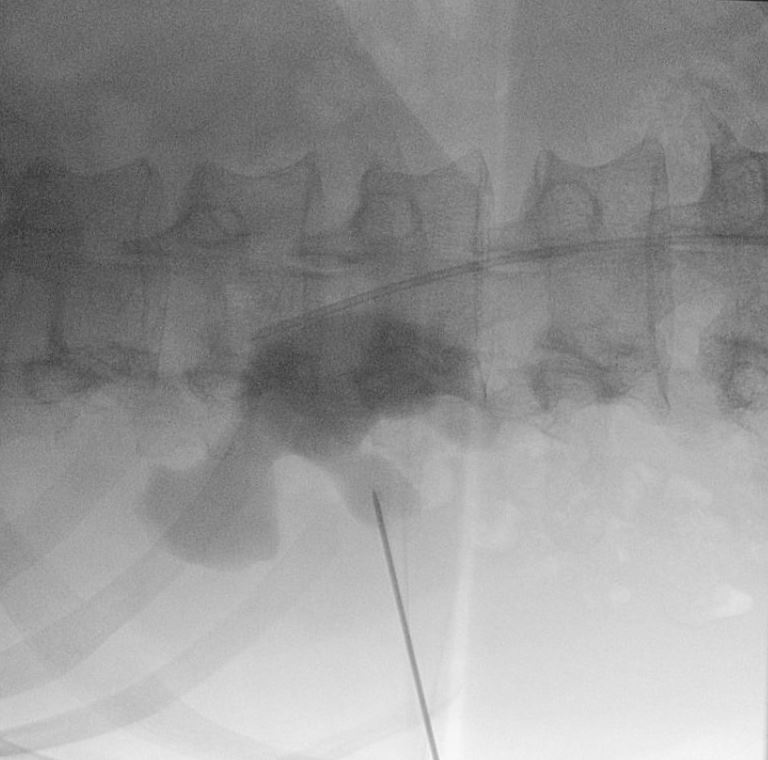
The collecting system was filled with contrast material that was mixed with methylene blue. Monoplanar access was created through the mid-calyx with 18-guage 15 cm length needle (Figure 4).
30 Fr balloon was used for dilation the tract. A 30 Fr Amplatz sheath was pushed over the balloon, then a 26 Fr nephroscope was inserted, the stone was identified, crushed and sucked with combined electro kinetic and ultrasonic energy using 3.9 mm probe (Swiss LithoClast® Trilogy Lithotripter). Endoscopically and on the fluoroscopy, there was no fragment could be seen by the end of the procedure (Figure 5).
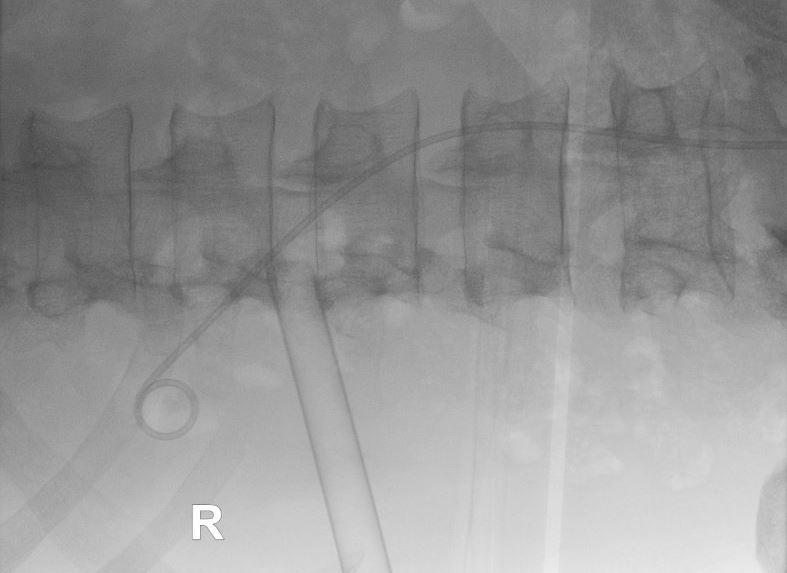
Six Fr 26 cm length JJ stent was fixed retrogradely and 16 Fr Foleys catheter was left in the urinary bladder. As there was no collecting system perforation, no bleeding, and no residual stone, no nephrostomy was inserted. At the end of the surgery 1000 mg tranexamic acid and 10 mg furosemide were given intravenously. The operating time was 90 minutes. Postoperatively the patient was doing well with normal vital signs and soft abdomen. Hemoglobin was
11.8mg/dL compare to 12 mg/dL preoperatively. The urine was clear (Figure 6).

In the 9th postoperative hour, the patient was discharged with the urethral catheter. The patient spent a total of 13 hours 40 minutes in the hospital. On the next day the urethral catheter was removed in the outpatient clinic. The stone analysis showed 90% Ca-Oxalate monohydrate and 10% Ca- Oxalate dihydrate. The JJ stent was removed on the 5th postop day. A follow-up KUB x-ray showed 6-mm residual stone in the upper calyx. Extracorporeal shockwave lithotripsy (ESWL) for the residual stone of the right kidney and PCNL for the left staghorn stone were planned, but due to Covid-19 pandemic, all elective procedures were suspended.
Discussion
Previous studies had shown that daycare PCNL is safe and effective [5]. The first reported outpatient PCNL was in 1986 by Preminger [4]. But despite the early start of this procedure, it was not widely practiced due to concerns about the patient’s safety. Specifically, post-operative infections, bleeding, and pain control that are common risks accompanying the procedure. Therefore, most centers opt to admit the patient overnight to monitor any signs of a complication, interestingly, it is unclear whether this practice improves outcomes [6].
Currently there is accelerated interest in ambulatory surgical procedures to reduce healthcare costs while maintaining the patient safety [7].
Advances in clinical approaches and technology have been made to PCNL, such as mini PCNL, various types of lithotripters and tubeless PCNL- whereby a ureteral stent replaces the traditional nephrostomy tube [8]. This has further encouraged the implementation of daycare PCNL
[9]. However, ambulatory PCNL can only be attempted on carefully selected patients due to the afore-mentioned risks [10].
A recent systemic review summarized the inclusion criteria: normal renal function, ASA I or II, BMI <30, adequate family and social support, age more than 18, single stone, lives nearby and has easy access to the hospital, motivated to be compliant post-operatively, normal contralateral kidney. In addition, certain criteria precluded the procedure for patients, such as an active urinary infection, solitary kidney, transplant kidney, congenital abnormality of the urinary tract, encrusted stents, BMI >30, active cardiac disease, staghorn calculi, multiple comorbidities, previous renal surgery and bleeding [11]. The case in the present report was comprised of certain aspects that have been listed in both the exclusion and inclusion criteria, which included: an ASA score of III, having multiple comorbidities, and the stone being partially staghorn. In addition, the case was conducted under spinal anesthesia in the supine position.
A meta-analysis published in 2020 had shown that there was no significant difference between the daycare PCNL and inpatient PCNL groups in the stone-free rate (P = 0.18), and the mean overall complication rates were 13.6% and 24.4% in the daycare and inpatient PCNL groups, respectively (P < 0.001). The two groups had similar readmission rates (P = 0.26), and the daycare PCNL was associated with a shorter operative time (P= 0.006) and shorter hospital stay (P = 0.01) [5].
The favorable data such as the significantly less complications and shorter operative time in the daycare group is due to strict selection criteria as mentioned above. The studies identified in this review support practice of ambulatory PCNL in carefully selected patients. With experience, its application can be further extended to patients with more complex stone disease and higher BMI [11].
When looking at the cost increment for the patients, Preminger, et al. reported that the cost of outpatient PCNL is 22% less than the inpatient PCNL when having the same inclusion criteria [4]. Moreover, Fareed, et al. reported that out of his 210 PCNL performed by a single experienced urologist, 97% of the cases were ambulatory cases [12]. Further studies also suggested that this approach is a potential algorithmic change in centers with sufficient case volume and with experience, ambulatory bilateral and multipuncture mini-PCNL can be carried out [13, 14].
Based on the more recent evidence, we had expanded our selection criteria and performed the procedure on this patient with success.
Conclusion
Daycare PCNL is a safe and effective procedure in selected patients. However, it should be performed in high volume centers by experienced endourologists. It has less cost, better utilization of the hospital resources and less nosocomial infection. The inclusion criteria can be expanded to have larger stone burden and ASA III patients; however randomized controlled trials are needed.
References
-
Fernstrom B (1976) Johansson, Percutaneous pyelolithotomy. A new extraction technique. Scand J Urol Nephrol 10(3): 257-259.
-
Valdivia Uría JG, Lachares Santamaría E, Villarroya Rodríguez S, Taberner Llop J, Abril Baquero G, et al. (1987) Percutaneous nephrolithectomy: simplified technic (preliminary report). Arch Esp Urol 40(3): 177- 180.
-
Turk C, Petrik A, Sarica K, Seitz C, Skolarikos A, et al. (2016) EAU guidelines on interventional treatment for urolithiasis. Eur Urol 69(3): 475-482.
-
Preminger GM, Clayman RV, Curry T, Redman HC, Peters PC (1986) Outpatient percutaneous nephrostolithotomy. J Urol 136(2): 355-357.
-
Gao M, Zeng F, Zhu Z, Zeng H, Chen Z, et al. (2020) Daycare surgery versus inpatient percutaneous nephrolithotomy: a systematic review and meta-analysis. Int J Surg 81: 132-139.
-
Fahmy A, Rhashad H, Algebaly O, Sameh W (2017) Can percutaneous nephrolithotomy be performed as an outpatient procedure? Arab J Urol 15(1): 1‐6.
-
Abbott JE, Davalos J (2017) Ambulatory Percutaneous Nephrolithotomy: 2-year 150 case experience. WCE Abstract. J Endourol 31(S2): A179.
-
Farach SM, Danielson PD, Walford NE, Harmel RP Jr, Chandler NM (2014) Same‐day discharge after appendectomy results in cost savings and improved efficiency. Am Surg 80(8): 787‐791.
-
Bellman GC, Davidoff R, Candela J, Gerspach J, Kurtz S, et al. (1997) Tubeless percutaneous renal surgery. J Urol 157(5): 1578-1582.
-
Beiko D, Lee L (2010) Outpatient tubeless percutaneous nephrolithotomy: The initial case series. Can Urol Assoc J 4(4): E86-90.
-
Jones P, Bennett G, Dosis A, Pietropaolo A, Geraghty R, et al. (2019) Safety and efficacy of day-case percutaneous nephrolithotomy: a systematic review from European society of uro-technology. Eur Urol Focus 5(6): 1127- 1134.
-
Fareed R, Shamim H (2021) The Pattern of Day Case (Ambulatory) Percutaneous (PCNL): A Descriptive Retrospective Study from a Tertiary Care Hospital. Nephro-Urol Mon 13(1): e103332.
-
Bechis SK, Han DS, Abbott JE, Holst DD, Alagh A, et al. (2018) Outpatient percutaneous nephrolithotomy: the UC san diego health experience. J Endourol 32(5): 394- 401.
-
Aarthy P, Thangarasu M, Sanjay Prakash J, Raghavan D, Jain N, et al. (2021) Safety and efficacy of mini‑percutaneous nephrolithotomy as daycare procedure: a prospective observational study. Afr J Urol 27: 9.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report