Antimicrobial Sensitivity Patterns of Uropathogens in India: A Nationwide, Multicentric, Big-Data, Retrospective Study
Introduction: With the increasing antimicrobial resistance, treating community acquired urinary tract infections (UTIs) has become a big challenge for many physicians, and the latest antimicrobial sensitivity patterns play a crucial role in successful outcomes. The current study aims to address the issue of lack of comprehensive regional antimicrobial resistance pattern data for uropathogens in India. Methods: This is an observational, retrospective study conducted on data (urine culture and sensitivity report) retrieved from the diagnostic laboratories across 29 Indian states and Union Territories. All urine samples with positive bacterial culture growth from January-December 2018 were included in the analysis. Sensitivity patterns of major urine isolates against 18 antimicrobials were described across multiple states. Results: There were 44624 positive urine culture samples. The mean age of the patients was 46.9 years, and a female preponderance (69.5%) was seen. Among females, Escherichia coli (66.6%) was the most common isolate followed by Klebsiella pneumoniae (12.8%) and Enterococcus spp. (6%). Urine samples from males had a comparatively higher isolation rate of Pseudomonas (53.8% vs 46.2%) but was lower for E. coli (27.7% vs 72.3%) when compared with females, respectively. Nitrofurantoin, levofloxacin, norfloxacin and fosfomycin were found to be the only antimicrobial agents against which overall urinary isolates have shown sensitivity >80% across at least one State. Conclusion: Common uropathogens showed decreasing sensitivity patterns to most of the conventional antimicrobials, which are particularly useful in the empirical management of UTIs. This study has reiterated the need to understand huge variations in antimicrobial sensitivity patterns across geographical regions in India.
Introduction
Urinary tract infections (UTIs) are common bacterial infections, affecting approximately 150 million people every year across the world and resulting in about $6 billion direct health expenditure [1, 2, 3]. Studies have shown the prevalence of UTIs in India to be consistently high ranging between 10.75-45.69% [4, 5, 6, 7, 8]. The UTIs are more common among women when compared with men [6, 7]. It is estimated that 50% of women get affected with at least one episode of UTI during their lifespan [2, 9]. The recurrence rate is high for UTIs with a study reporting 27% recurrence rate within 6 months in women with a history of UTI [10]. Similarly, 10–15% of women over 60 years of age have frequent recurrences of UTIs with an overall 1-year recurrence rate of 44% among women aged 17 to 82 years [11, 12].
The UTIs are caused by a range of microorganisms, including gram-positive and gram-negative bacteria, and fungi. The most common pathogens involved in uncomplicated UTIs are Escherichia coli, Klebsiella pneumoniae, Staphylococcus saprophyticus, Enterococcus faecalis, Pseudomonas aeruginosa, Staphylococcus aureus and Candida sps [13, 14, 15, 16]. Complicated UTIs are commonly caused by Enterococcus spp., Klebsiella pneumoniae, Candida spp, Staphylococcus aureus, Proteus mirabilis, Pseudomonas aeruginosa and group B streptococcus (GBS) [17, 18, 19, 20].
Antimicrobial resistance (AMR) is a serious threat to public health. According to a multicentre study [21] in India, 26.9% of gram-negative isolates from urine cultures were extended-spectrum β-lactamase (ESBL) producers and showed dismal sensitivity against ciprofloxacin (35.8%), trimethoprim-sulfamethoxazole (30%), amoxicillin (17.7%), amoxicillin-clavulanate (41.6%) and nitrofurantoin (65.7%). A tertiary care centre-based study [22] in Karnataka found 43% of E. coli isolates from urine as multi-drug resistant and showed declining trend of sensitivity with time over a period ranging from 2012-2015. The increased AMR has made the management of community acquired UTIs a challenge for many physicians and hence, the latest antimicrobial sensitivity patterns may facilitate treatment choices which might result in successful outcomes.
Broad spectrum antibiotics form the bedrock of the empirical management of UTIs. The overall antimicrobial use in such conditions should be guided by regional antimicrobial resistance surveillance data regarding these antimicrobial agents. Such regional data is very scarce in developing countries, especially in India. In order to enhance the impact of the antimicrobial stewardship programs and incorporate regional trends of antimicrobial resistance in the overall practice, guidelines have been formulated (Antimicrobial Stewardship Program Guideline – Indian Council of Medical Research (ICMR) – 2018 [23], World Health Organization Guidelines on antimicrobial resistance – 2017 [24], a step-by- step approach for the development and implementation of hospital antibiotic policy and standard treatment guidelines – 2011 [25]) which consider local resistance patterns while selecting an appropriate antimicrobial agent. In India, although there are several studies [21, 22] on AMR patterns of uropathogens conducted in the community or hospital settings, studies comparing the antimicrobial sensitivity patterns amongst the uropathogens at a nationwide level are scarce. The current study was designed to understand the antimicrobial sensitivity patterns of major uropathogens against commonly used antimicrobial agents across regions in India.
Methods
Study Design
This was an observational, retrospective study conducted on database (urine culture and sensitivity report) retrieved from diagnostic labs (following the Clinical & Laboratory Standards Institute (CLSI) and European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines for clinical breakpoints and dosing of antibiotics – for antimicrobial sensitivity pattern testing) located across 29 Indian states and Union Territories (UTs). All urine samples with a positive bacterial culture growth from January- December 2018 were included in the analysis.
Sampling Technique
All urine culture and sensitivity test (CST) with positive bacterial growth were included in the study. In the case of more than one urine sample from a subject, only the first sample was considered for analysis. Samples with multiple isolates and fungal growths were excluded from the analysis. Segregation of data was done into two categories namely outpatient clinic and hospital-based samples. Only outpatient clinic-based sensitivity data were included in the study which is reflective of community-acquired urinary tract infections. The sensitivity of culture isolates was assessed against the following 18 antimicrobial agents.
- Penicillins (amoxicillin, ampicillin, amoxicillin-clavulanic acid)
- Cephalosporins (cefixime, cefuroxime, cefpodoxime)
- Macrolides (erythromycin, clarithromycin, azithromycin)
- Quinolones (ciprofloxacin, levofloxacin, norfloxacin)
- Sulfamethoxazole+trimethoprim (cotrimoxazole)
- Trimethoprim
- Tetracyclines (tetracycline, doxycycline)
- Fosfomycin
- Nitrofurans (nitrofurantoin)
Study Outcomes
The overall sensitivity of urine samples (all isolates together) against the above-mentioned antimicrobial agents was compared across the states and UTs. The sensitivity patterns of major isolates against 18 antimicrobials were also described.
Data Analysis
Data were analyzed using R studio 3.2.3. The culture and sensitivity indices were described in the form of proportions. All samples reported as intermediate or resistant were considered as resistant. Continuous variables were presented as means while categorical variables in the form of proportions. Proportional distribution of major isolates from urine cultures was presented across age and gender.
Ethical Considerations
Confidentiality of the patient identification was maintained and only de-identified and anonymized data was used for analysis.
Results
Study Population
A total of 44624 positive urine culture samples (isolated from an equal number of subjects) were included. The patients had a mean age of 46.9 years and there was a female preponderance (69.5%). The majority of the samples were obtained from adults (52.8%) followed by the elderly population (35.0%); 12.3% belonged to the pediatric population (Table 1 and Figure 1).
| Total Samples (N=44624) | Males (N=13625) | Females (N=30999) | |
|---|---|---|---|
| Age in years, mean (SD) | 46.9 (23.9) | 51.3 (26.3) | 44.9 (22.6) |
| Age categories (years), n (%) | |||
| <18 | 5467 (12.25) | 2229 (40.77) | 3238 (59.23) |
| 19 - 60 | 23537 (52.75) | 4990 (21.20) | 18547 (78.80) |
| >60 | 15620 (35.00) | 6406 (41.01) | 9214 (58.99) |
| Total | 44624 | 13625 (30.53) | 30999 (69.47) |
| Pathogens, n (%) | |||
| Escherichia coli | 29706 (66.57) | 8220 (27.67) | 21486 (72.33) |
| Klebsiella pneumoniae | 5719 (12.82) | 1722 (30.11) | 3997 (69.89) |
| Enterococcus spp. | 2690 (6.03) | 1060 (39.41) | 1630 (60.59) |
| Pseudomonas aeruginosa | 1707 (3.82) | 918 (53.78) | 789 (46.22) |
| Proteus mirabilis | 737 (1.64) | 320 (43.42) | 417 (56.6) |
| Others | 4065 (9.10) | 1385 (34.07) | 2680 (65.92) |
| Total | 44624 | 13625 (30.53) | 30999 (69.47) |
Table 1: Age and gender wise distribution of urine culture isolates The overall number of urine isolates included in the study wa
Table 1: Age and gender wise distribution of urine culture isolates The overall number of urine isolates included in the study was 44624 from diagnostic labs located across 29 states and UTs in India. There were 13 states with a sample size of more than 500. Major contributors to the sample population were Maharashtra (10353), Delhi (5559), Uttar Pradesh (4561), Assam (3077), Punjab (3075), Tamil Nadu (2909), West Bengal (2708), Kerala (2411), Karnataka (2320), Haryana (2033) and Chandigarh (1801) (Figure 2).
The states with a sample size less than 100, were clubbed in a category called others. These states and UTs included Gujarat, Odisha, Andaman and Nicobar Islands, Bihar, Dadra and Nagar Haveli, Tripura, Mizoram, and Manipur.
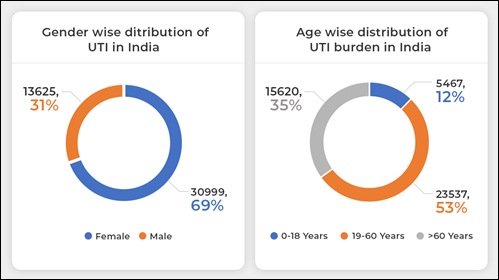
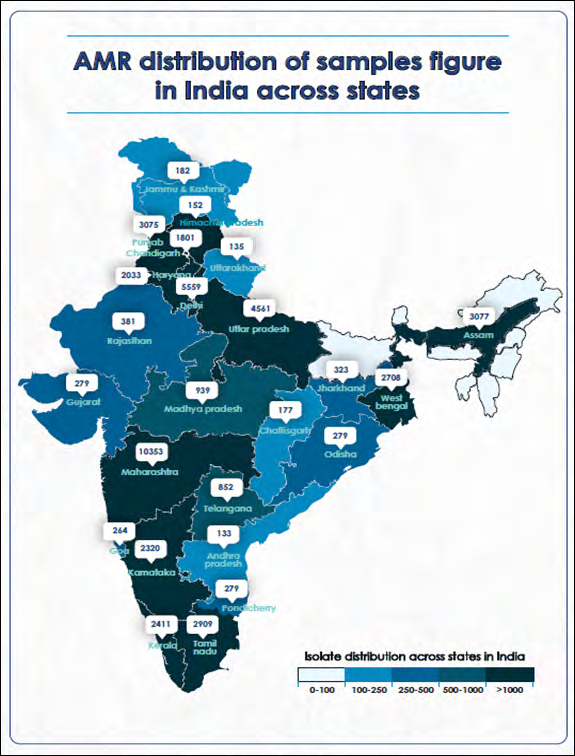
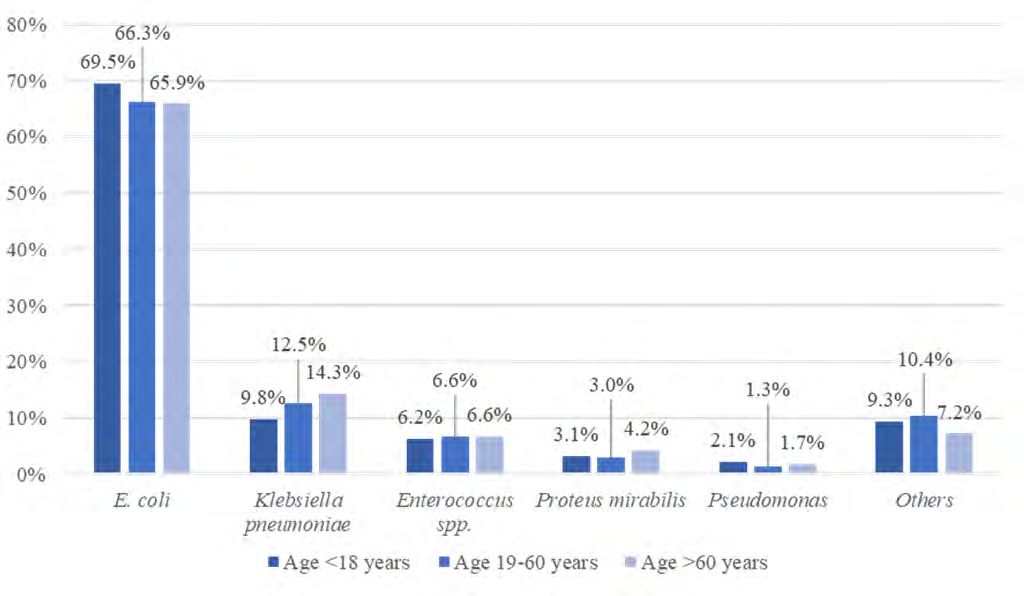
Figure 2: Distribution of culture positive samples across Indian states Among females, E. coli was the most common isolate followed by K. pneumoniae and Enterococcus spp. Urine samples from males had a comparatively higher isolation rate of Pseudomonas (53.8% vs 46.2%) but that of E. coli (27.7% vs 72.3%) was lower when compared with females (Table 1). The isolation rates for all the isolates were found to be comparable across all the age groups (Figure 3).
Majority of the antimicrobials were oral preparations and thus mostly given in clinic/out-patient department (OPD) settings. The overall sensitivity of E. coli was <50% to all antimicrobial agents, except fosfomycin (73.5%) and nitrofurantoin (79.4%). K. pneumoniae also showed poor sensitivity (<50%) to most of the drugs except to fluoroquinolones, cotrimoxazole and fosfomycin. P. mirabilis showed high sensitivity (>80%) to fosfomycin and cefpodoxime. Pseudomonas and other isolates also showed >80% sensitivity to fosfomycin. 83.9% of the Enterococcus isolates and 65.1% of the other isolates showed sensitivity to nitrofurantoin.
Nitrofurantoin, levofloxacin, norfloxacin and fosfomycin were found to be the only antimicrobial agents against which overall urinary isolates had shown sensitivity >80% across at least one state. Only 10 states and UTs had at least one antimicrobial agent against, which urinary isolates showed a sensitivity of >80%. These states and UTs included Andhra Pradesh, Chandigarh, Goa, Karnataka, Maharashtra, Rajasthan, Tamil Nadu, Uttar Pradesh, and West Bengal. Among all states, urinary isolates showed poor sensitivity for penicillins (amoxicillin, ampicillin, amoxicillin-clavulanic acid) except for Himachal Pradesh and Telangana, where sensitivity was >60%. Only in Karnataka and Rajasthan, uropathogens have shown a sensitivity >80% for fluoroquinolones (for levofloxacin in Karnataka and for norfloxacin in Rajasthan). In rest of the states, sensitivity ranged from poor to moderate. In Rajasthan, sensitivity to norfloxacin was exceptionally high (90.3%). Across all states, urine isolates have shown comparatively better sensitivity to nitrofurantoin. Sensitivity for nitrofurantoin was >50% in all states and >80% in Andhra Pradesh, Tamil Nadu, and Telangana.
Sensitivity to macrolides was <50% in all states except in Assam and Madhya Pradesh where sensitivity to azithromycin and erythromycin in the urine isolates was > 50% respectively. For cephalosporins also, sensitivity was <50% in most of the states with a few exceptions such as Maharashtra, Rajasthan, Uttarakhand, where at least for one cephalosporin sensitivity was >50%. Tetracyclines (doxycycline and tetracycline) also performed poor and, culture isolates showed a sensitivity >50% only in a few states. Even for fosfomycin, sensitivity was alarmingly low especially in south Indian states such as Andhra Pradesh (42.9%), Karnataka (37.3%) and Tamil Nadu (33.9%). There were only a few states with sensitivity >50% for trimethoprim and cotrimoxazole.
An assessment of the overall sensitivity patterns (across all states) is presented in Figure 4.
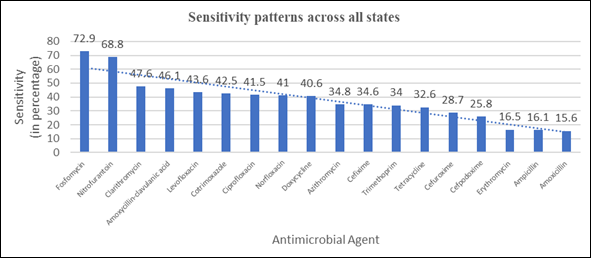
Figure 4: Overall sensitivity patterns of urinary isolates in the study The sensitivity was >50% only for fosfomycin (72.9%) and nitrofurantoin (68.8%). There were antimicrobial agents, with sensitivity <20% such as amoxicillin (15.6%), ampicillin (16.1%) and erythromycin (16.5%). There were six antimicrobials with sensitivity between 20-40% including azithromycin (34.8%), cefixime (34.6%), cefpodoxime (25.8%), cefuroxime (28.7%), tetracycline (32.6%) and trimethoprim (34.0%). Antimicrobial agents with 40-50% sensitivity included doxycycline (40.6%), cotrimoxazole (42.5%), amoxycillin-clavulanic acid (46.1%), ciprofloxacin (41.5%), levofloxacin (43.6%), norfloxacin (41.0%), and clarithromycin (47.6%) (Tables 2, 3a, and 3b).
| Escherichia coli N (% sensitive) | Klebsiella pneumoniae N (% sensitive) | Proteus mirabilis N (% sensitive) | Enterococcus spp. N (% sensitive) | Pseudomonas N (% sensitive) | Others N (% sensitive) | |
|---|---|---|---|---|---|---|
| Amoxicillin | 11930 (16.8) | 2100 (3.2) | 233 (36.1) | 457 (69.8) | 794 (1.8) | 1104 (9.1) |
| Amoxicillin clavulanic acid | 23251 (45.7) | 5296 (48) | 553 (66.4) | 898 (79.3) | 436 (12.4) | 2274 (34.6) |
| Ampicillin | 27381 (16.5) | 5609 (1.6) | 562 (36.7) | 986 (70.7) | 599 (9.2) | 2186 (20.9) |
| Azithromycin | 712 (30.2) | 26 (7.7) | - | 221 (50.2) | 18 (33.3) | 171 (38.6) |
| Cefixime | 14381 (33.6) | 2366 (47.7) | 290 (68.3) | 209 (9.1) | 964 (4.4) | 1055 (41.7) |
| Cefpodoxime | 4727 (23.9) | 743 (34.1) | 97 (81.4) | 134 (1.5) | 96 (2.1) | 214 (41.1) |
| Cefuroxime | 22199 (26) | 4526 (42.9) | 552 (60.3) | 412 (6.3) | 389 (3.6) | 2145 (26.9) |
| Ciprofloxacin | 27224 (35.3) | 5637 (60.3) | 710 (45.1) | 2368 (35.4) | 1712 (57.4) | 3667 (54.5) |
| Clarithromycin | 16 (50) | 5 (20) | - | 19 (57.9) | - | 84 (46.4) |
| Doxycycline | 726 (49.4) | 357 (30.8) | 62 (0%) | 295 (30.2) | 204 (3.4) | 573 (58.3) |
| Erythromycin | 132 (17.4) | 7 (28.6) | 1 (100%) | 1683 (11.6) | 5 (0) | 478 (33.3) |
| Fosfomycin | 6723 (73.5) | 1579 (63.6) | 189 (87.3) | 427 (76.1) | 329 (80.2) | 367 (83.7) |
| Levofloxacin | 12247 (40.3) | 1913 (53.1) | 323 (48.9) | 1728 (36.3) | 1446 (54.9) | 2359 (50.7) |
| Nitrofurantoin | 27067 (79.4) | 5557 (24.6) | 632 (7.3) | 2081 (83.9) | 510 (26.3) | 3242 (65.1) |
| Norfloxacin | 14856 (36.3) | 2455 (64) | 296 (59.5) | 750 (19.2) | 1051 (53.1) | 1405 (50.2) |
| Cotrimoxazole | 16411 (38.8) | 2794 (60.6) | 343 (42.6) | 567 (30) | 282 (13.1) | 1752 (56.6) |
| Tetracycline | 2053 (32.2) | 132 (5.3) | 65 (0) | 1876 (30.4) | 282 (2.1) | 913 (53.3) |
| Trimethoprim | 4811 (33.2) | 924 (33.8) | 176 (28.4) | 5 (40) | 24 (20.8) | 633 (43.1) |
Table 2: Sensitivity patterns of major isolates against various antimicrobial agents
| States | Amoxi cillin | Amoxicillin- clavulanic acid | Ampi cillin | Ciproflo xacin | Levoflo xacin | Norflo xacin | Nitrofu rantoin | Clarithro mycin | Erythro mycin | Azithro mycin | Region |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Andhra Pradesh | 22 (18.2) | 112(35.7) | 100 (32) | 110 (56.4) | 48(50) | 83(60.2) | 104(81.7) | - | 17(23.5) | - | South |
| Karnataka | 1100(14.8) | 1883(42.9) | 1794(20.1) | 2243(57.1) | 190(80.5) | 844(52.5) | 2047(71) | 37 (70.3) | 139 (36) | 86(41.9) | South |
| Kerala | 1935 (0.5) | 200(17.5) | 2197 (1.7) | 1800(45.9) | 40(50) | 1591(37) | 294(56.5) | 2(50) | 126 (8.7) | 118 (7.6) | South |
| Tamil Nadu | 121(11.6) | 2645 (29) | 2587 (23) | 2731 | 179 (48.6) | 2575(45.7) | 2614 (85.7) | 2 (50) | 354 (22.6) | 28 (3.6) | South |
| Telangana | - | 117 (71.8) | 460 (12) | 162 (46.9) | 682 (78) | 756 (42.1) | 828 (80.7) | - | - | 13 (15.4) | South |
| Assam | 79 (25.3) | 1514 (50.7) | 2746 (20.3) | 3014 (46.8) | 1574 (47.1) | 1104 (39.7) | 3017 (72) | 7 (14.3) | 18 (5.6) | 127 (54.3) | North East |
| Chandigarh | 27 (22.2) | 1587 (49.6) | 1567 (14.1) | 1787 (32.4) | 376 (31.9) | 153 (38.6) | 1753 (66.1) | - | 11 (27.3) | 1 (100) | North |
| Delhi | 96(16.7) | 4283 (47.3) | 4263 (14.9) | 4853 (41.4) | 1969 (38.9) | 1652(24.5) | 5185 (65.4) | - | 282(8.9) | 189(16.9) | North |
| Haryana | - | 1811(55.4) | 1740 (14.9) | 2021 (46.3) | 154(44.2) | - | 1933(59.6) | - | 113 (7.1) | - | North |
| Himachal Pradesh | - | 119(61.3 | 115 (20) | 152 (55.9) | 29 (55.2) | - | 142 (68.3) | - | 24 (4.2) | - | North |
| Jammu & Kashmir | - | 147 (47.6) | 142 (8.5) | 182 (31.3) | 31 (22.6) | - | 173 (64.2) | - | 27 (11.1) | - | North |
| Uttar Pradesh | 983 (21) | 1969 (54.4) | 3594 (20.9) | 3975 (40) | 1727 (57) | 1113 (18.8) | 4170 (74.6) | 5 (40) | 467 (12.6) | 384 (39.3) | North |
| Uttarakhand | - | 37 (35.1) | 34 (8.8) | 39 (23.1) | 97 (41.2) | - | 37 (51.4) | - | - | - | North |
| Punjab | 74 (20.3) | 2539 (32.5) | 2487 (11.6) | 3009 (28) | 747 (34.1) | 437 (36.6) | 2850 (58.6) | - | 307 (12.1) | 46 (60.9) | North |
| Chhattisgarh | 10 (10) | 9 (44.4) | 9 (11.1) | 175 (17.7) | 10 (50) | 172 (30.2) | 174 (61.5) | - | - | - | Central |
| Madhya Pradesh | 195 (21.5) | 923 (39.2) | 645 (6) | 908 (31.2) | 787 (31.9) | 849 (26.3) | 888 (74.7) | - | 57 (54.4) | 40 (20) | Central |
| Goa | 260 (12.3) | 231 (43.3) | 241 (13.3) | 261 (38.3) | 263 (40.7) | 210 (45.7) | 227 (67) | - | 2(0) | - | West |
| Maharashtra | 9087(16) | 9398 (50.1) | 9548 (16.8) | 10244 (40.1) | 9070 (40.8) | 7448 (47.5) | 9238 (65.3) | 61 (39.3) | 197 (21.8) | 62 (43.5) | West |
| Rajasthan | 254 (24.4) | 351(51.9) | 341 (21.7) | 380 (41.6) | 266 (49.6) | 134 (90.3) | 344 (65.4) | 2 (50) | 30 (10) | 2 (50) | West |
| West Bengal | 1829 (23.5) | 2261 (47.4) | 2200 (15.9) | 2674 (38.6) | 1315 (40.9) | 1337 (38.3) | 2525 (73.2) | 2 (0) | 79 (15.2) | 48 (66.7) | East |
| Jharkhand | 298 (21.8) | 309 (48.5) | 251 (15.5) | 320 (39.7) | 225 (38.7) | 225 (32.4) | 288 (72.9) | 2 (50) | 35 (20) | 1(100) | East |
| Others | 248 (16.9) | 263 (49.8) | 262 (16.8) | 278 (38.5) | 237 (36.7) | 130 (64.6) | 258 (66.7) | 4 (50) | 21 (14.3) | 3 (66.7) | - |
| Total | 16618 (15.6) | 32708 (46.1) | 37323 (16.1) | 41318 (41.5) | 20016 (43.6) | 20813 (41) | 39089 (68.8) | 124 (47.6) | 2306 (16.5) | 1148 (34.8) | - |
Table 3: Sensitivity patterns of major isolates against various antimicrobial agents
Table 3a: Overall sensitivity patterns of urinary isolates across states
| States | Cefixime | Cefpodoxime | Cefuroxime | Doxycycline | Tetracycline | Fosfomycin | Cotrimoxazole | Trimethoprim | Region |
|---|---|---|---|---|---|---|---|---|---|
| Andhra Pradesh | 78(44.9) | 69 (26.1) | 22 (22.7) | 4 (0) | 19 (26.3) | 70 (42.9) | 77 (54.5) | 11 (0) | South |
| Karnataka | 639 (43.3) | 496 (22.6) | 1488 (42.5) | 59 (74.6) | 136 (41.2) | 582 (37.3) | 850 (51.9) | - | South |
| Kerala | 1095 (6.3) | 1039 (5.1) | 2005 (3.4) | - | 153 (22.2) | 38 (36.8) | 2091 (4.5) | - | South |
| Tamil Nadu | 2345 (44.3) | 2151 (25) | 308 (27.9) | 16 (18.8) | 345 (36.8) | 2385 (33.9) | 2313 (55.3) | 7 (0) | South |
| Telangana | - | 50 (20) | 153 (27.5) | 10 (0) | 658 (34) | - | 624 (42.9) | - | South |
| Assam | 1077 (36.1) | - | 1088(21) | 1314(49.8) | 264(46.2) | - | 1617(46.1) | 36(33.3) | North East |
| Chandigarh | 1693(40) | 4(0) | 1568(30.7) | 12(66.7) | 42(33.3) | 190(81.1) | 1635(40.7) | - | North |
| Delhi | 1259(17) | 135(0) | 4352(33.7) | 1(0) | 810(34.7) | 122(73) | 1563(31.1) | - | North |
| Haryana | - | - | 1818(35.4) | - | 120(25.8) | - | 1(100) | - | North |
| Himachal Pradesh | - | - | 119(42) | - | 24(29.2) | - | - | - | North |
| Jammu & Kashmir | - | - | 147(19) | - | 27(22.2) | - | - | - | North |
| Uttar Pradesh | 317(19.2) | - | 1998(32.9) | 26(65.4) | 804(43.9) | 121(95.9) | 1076(29.3) | 590(32.9) | North |
| Uttarakhand | - | 96(74) | 37(16.2) | - | - | - | - | - | North |
| Punjab | 530(40.4) | 6(0) | 2494 (23.2) | 31(74.2) | 466(27.7) | 3(100) | 196(33.2) | 1(100) | North |
| Chhattisgarh | 170(10) | - | 176(15.9) | 2(50) | 1(0) | - | - | 6(0) | Central |
| Madhya Pradesh | 850 (42) | 520(4) | 632(6.8) | 35(57.1) | 534(20.6) | 43(90.7) | 816(30) | 21(0) | Central |
| Goa | 206(30.1) | 31(67.7) | 230(27.4) | 14(7.1) | 14(14.3) | 142(97.9) | 170(54.1) | 166(34.3) | West |
| Maharashtra | 7103(36.4) | 1287 (54) | 8947(30.2) | 612(19.1) | 676(22.6 ) | 5286(90.9) | 7909(52.3) | 5629(35) | West |
| Rajasthan | 82(72) | - | 348(32.5) | 45(15.6) | 59(27.1) | - | - | 57(0) | West |
| Jharkhand | 220(32.3) | 9(33.3) | 300(33.3) | - | 25(25) | 9(33.3) | 137(51.1) | - | East |
| West Bengal | 1501(32.6) | 117(9.4) | 1727(33) | 3(0) | 116(37.9) | 623(95.3) | 1074(42.6) | 5(20) | East |
| Others | 100(48) | 1(0) | 266(32.3) | 33(12.1) | 41(39) | - | - | 44(2.3) | - |
| Total | 19265(34.6) | 6011(25.8) | 30223(28.7) | 2217(40.6) | 5321(32.6) | 9614(72.9) | 22149(42.5) | 6573(34) | - |
Table 4: Sensitivity patterns of major isolates against various antimicrobial agents
Table 3b: Overall sensitivity patterns of urinary isolates across states
Discussion
The current study aims to address the issue of lack of comprehensive regional antimicrobial resistance pattern data for uropathogens in India and provide an enhanced understanding of such regional variations within India which can be incorporated into local antimicrobial prescription policies or protocols. Various studies in India as well as in other countries have reported that the most common urinary pathogens are E. coli followed by K. pneumonia [26, 27, 28, 29]. The current study showed E. coli as the most common uropathogen followed by K. pneumoniae both among women and men. P. aeruginosa, P. mirabilis and Enterococci were among other important uropathogens.
This study assessed the geographical variation in antimicrobial sensitivity patterns of urinary isolates across Indian states. As AMR is a spatiotemporally dynamic phenomenon, therefore it is essential to understand recent patterns of antimicrobial resistance across regions. According to the ICMR guidelines [30] 2019, empirical treatment for acute cystitis includes nitrofurantoin, cotrimoxazole and ciprofloxacin, while cefixime and cefuroxime can be used as alternatives. In the case of acute prostatitis, doxycycline, ciprofloxacin and cotrimoxazole were empirically recommended, while piperacillin tazobactam, cefoperazone and ertapenem were recommended as an alternative empirical therapy.
The current study showed a wide variation in sensitivity patterns across states and highlighted the importance of local antimicrobial sensitivity data in antimicrobial stewardship. The sensitivity of urinary isolates (collectively) to ciprofloxacin was 41.5%, overall ranging from 17.7% (Chhattisgarh) and 31.2% (Madhya Pradesh) to 57.1% (Karnataka). It is evident that antimicrobial agents relevant in one geographical area might be of less use in other regions. Fosfomycin showed a wide variation in sensitivity ranging from 33.9% in Tamil Nadu to 97.9% in Goa.
The current study showed a high resistance among urinary isolates for multiple antimicrobial classes. A multicentre study conducted in West Bengal showed a high resistance of uropathogens for penicillins (~60%) and an increasing trend of resistance from 2008-2013 [31]. Concurrently, in our study, there was a much higher resistance (>80%) for penicillins (amoxicillin and ampicillin) at the national level as well as in West Bengal. Uropathogens were found to be highly resistant to fluoroquinolones in India. A study [32] conducted in Ahmedabad (Gujarat) reported 85.5% resistance to ciprofloxacin and 53.8% to levofloxacin among uropathogens (2013-2015). Another study [22] from Karnataka reported 65.8% resistance to ciprofloxacin and 53.7% to norfloxacin among E. coli isolated from urine cultures. Our study also reported a high resistance among E. coli to ampicillin (82.5%), cefuroxime (72.4%) but good sensitivity to nitrofurantoin (92.4%). A tertiary care centre in Mumbai also reported a high sensitivity for ESBL E. coli and K. pneumoniae for fosfomycin (ESBL E. coli 99.6% and K. pneumoniae 87.7%) and nitrofurantoin (ESBL E. coli 93.7%). Even ESBL organisms were quite sensitive to fosfomycin and nitrofurantoin with similar results seen in this study as well [33]. A Puducherry [34] based study reported 73% resistance to ciprofloxacin, 80.6% to ampicillin and 26.9% to nitrofurantoin among E. coli isolated from urinary isolates. A tertiary care centre-based study in rural Kerala [35] reported 63% resistance among E. coli and Klebsiella spp. against fluoroquinolones. Similar patterns of antimicrobial sensitivity were shown by studies conducted across India at various centres but a single comprehensive study comparing pan-India trends is still warranted [4, 5, 6, 7, 8].
A Bangalore based study [36] reported urinary isolates from community acquired UTI cases with high resistance to fluoroquinolones (74.1%). Another recent study [37] conducted in Ahmedabad (Gujarat) estimated the sensitivity of E. coli to nitrofurantoin, cotrimoxazole and ciprofloxacin as 72.33%, 18.97% and 27.27%, while for Klebsiella spp. it was 32.0%, 51.77% and 22.13% respectively. A hospital- based study in Tripura [38] also reported high resistance among E. coli and Klebsiella for ciprofloxacin (83.4%, 55.1%), amoxicillin-clavulanic acid (93.0%, 97.8%) and cefuroxime (92.9% and 90.6%), respectively.
Majority of the studies highlighted high resistance among uropathogens against commonly used antimicrobial agents in different states. Our study compared state-wise antimicrobial sensitivity patterns. Further research is required to understand factors responsible for significant differences in sensitivities across various geographical areas. Local prescription practices, availability of antimicrobials, enforcement status of regulation for antibiotic prescription, awareness of the health care providers seem the plausible reasons for these geographical variations, though more research is required in this domain.
Most of the studies across India reported fosfomycin as highly effective in treating urinary tract infections. A prospective study [39] from Aligarh found fosfomycin as highly effective (~100%) against Methicillin-resistant Staphylococcus aureus (MRSA), Vancomycin-resistant Enterococci (VRE), ESBL, High-level aminoglycoside resistance (HLAR) and overall isolates from urine samples. Another prospective study [40] conducted in a tertiary care centre in eastern India found that 95.18% of overall urine isolates and 95.93% of multi-drug resistant Enterobacteriaceae were susceptible to fosfomycin. In our study similar findings of high sensitivity of overall urinary isolates across states such as West Bengal (95.3%), Uttar Pradesh (95.9%), Maharashtra (90.9%), Madhya Pradesh (90.7%), Goa (97.9%) and Chandigarh (81.1%) were reported. However, sensitivity of urinary isolates to fosfomycin was poor across South Indian states, including Andhra Pradesh (42.9%), Karnataka (37.3%), Kerala (36.8%) and Tamil Nadu (33.9%).
This is one of the few studies conducted in India, which has highlighted regional differences in antimicrobial sensitivity of uropathogens with the help of diagnostic data. The extremely large database, along with the ability to differentiate AMR patterns across age, gender, and states, are the major strengths of this study. This study has certain inherent limitations associated with diagnostic laboratory- based data. The non-availability of clinical information regarding signs and symptoms, risk factors such as diabetes, associated comorbidities, catheterization, urological and gynaecological conditions, and surgeries are important limitations.
Conclusion
This study showed that the common uropathogens responsible for UTIs had a decreasing sensitivity patterns to most of the conventional antimicrobials, which are used in the empirical management of UTIs. The current study highlights the need for a renewed emphasis on the education of the physicians related to the threat of antimicrobial resistance and increasing awareness about the local antimicrobial sensitivity patterns. The current study also reiterates the need to understand huge variations in antimicrobial sensitivity patterns across geographical regions in India. This study has provided consolidated evidence for the use of local sensitivity data in antimicrobial stewardship. As high-end antimicrobial agents are also becoming irrelevant and less efficacious, it should be the utmost priority for governments and related agencies to implement regulatory policies strictly.
Acknowledgments
None.
Declaration of Interest
The author declares no conflict of interest.
References
-
Harding GK, Ronald AR (1994) The management of urinary infections: what have we learned in the past decade? Int J Antimicrob Agents 4(2): 83-88.
-
Foxman B (2014) Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am 28(1): 1-13.
-
O’Brien VP, Hannan TJ, Nielsen HV, Hultgren SJ (2016) Drug and vaccine development for the treatment and prevention of urinary tract infections. Microbiol Spectr 4(1): 10.
-
Thass N, Kumar M, Kaur R (2019) Prevalence and antibiogram of bacterial pathogens causing urinary tract infection in a tertiary care hospital. Int J Med Sci Public Health 8(1): 53-57.
-
John S, Sumitha S (2018) Prevalence of UTI in Different Age Groups in a Tertiary Care Hospital and their Antibiogram. Int J Contemp Med Res 5(1): 3-6.
-
Pardeshi P (2015) Prevalence of urinary tract infections and current scenario of antibiotic susceptibility pattern of bacteria causing UTI. Indian J Microbiol Res 5(3): 334- 338.
-
Janifer J, Geetha lakshmi S, Satyavani K, Viswanathan V (2009) Prevalence of lower urinary tract infection in South Indian type 2 diabetic subjects. Indian J Nephrol 19(3): 107-111.
-
Syed M, Ramakrishna P, Shaniya K, Arya B, Shakir VPA (2012) Urinary Tract Infections – An overview on the Prevalence and the Antibiogram of Gram Negative Uropathogens in A Tertiary Care Centre in North Kerala, India. J Clin Diagnostic Res 6(7): 1192-1195.
-
Hooton TM, Scholes D, Hughes JP, Winter C, Roberts PL, et al. (1996) A prospective study of risk factors for symptomatic urinary tract infection in young women. N Engl J Med 335(7): 468-474.
-
Foxman B (1990) Recurring urinary tract infection: incidence and risk factors. Am J Public Health 80(3): 331-333.
-
Ikäheimo R, Siitonen A, Heiskanen T, Kärkkäinen U, Kuosmanen P, et al. (1996) Recurrence of urinary tract infection in a primary care setting: Analysis of a 1-year follow-up of 179 women. Clin Infect Dis 22(1): 91-99.
-
Romano JM, Kaye D (1981) UTI in the elderly: Common yet atypical. Geriatrics 36(6): 113-115.
-
Foxman B (2014) Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am 28(1): 1-13.
-
Nielubowicz GR, Mobley HL (2010) Host–pathogen interactions in urinary tract infection. Nature Rev Urol 7(8): 430-441.
-
Kline KA, Schwartz DJ, Lewis WG, Hultgren SJ, Lewis AL (2011) Immune activation and suppression by group B _Streptococcus_ in a murine model of urinary tract infection. Infect Immun 79(9): 3588-3595.
-
Ronald A (2002) The etiology of urinary tract infection: traditional and emerging pathogens. Am J Med 113(1): 14-19.
-
Levison ME, Kaye D (2013) Treatment of complicated urinary tract infections with an emphasis on drug- resistant Gram-negative uropathogens. Curr Infect Dis Rep 15(1): 109-115.
-
Fisher JF, Kavanagh K, Sobel JD, Kauffman CA, Newman CA(2011) Candida urinary tract infection: pathogenesis. Clin Infect Dis 52 (Suppl 6): S437-S451.
-
Chen YH, Ko WC, Hsueh PR (2013) Emerging resistance problems and future perspectives in pharmacotherapy for complicated urinary tract infections. Expert Opin Pharmacother 14(5): 587-596.
-
Jacobsen SM, Stickler DJ, Mobley HL, Shirtliff ME (2008) Complicated catheter-associated urinary tract infections due to _Escherichia coli_ and Proteus mirabilis_._ Clin Microbiol Rev 21(1): 26-59.
-
Kothari A, Sagar V (2008) Antibiotic resistance in pathogens causing community-acquired urinary tract infections in India: a multicenter study. J Infect Dev Ctries 2(5): 354-358.
-
Kulkarni SR, Peerapur BV, Sailesh KS (2017) Isolation and antibiotic susceptibility pattern of _Escherichia coli_ from urinary tract infections in a tertiary care hospital of North Eastern Karnataka. J Nat Sc Biol Med 8(2): 176-180.
-
ICMR (2018) Antimicrobial Stewardship Program Guidelines, Indian council of medical research, Government of India, pp: 1-62.
-
Tang KL, Caffrey NP, Nóbrega DB, Cork SC, Ronksley PE, et al. (2017) Restricting the use of antibiotics in food- producing animals and its associations with antibiotic resistance in food-producing animals and human beings: a systematic review and meta-analysis. Lancet Planet Health 1(8): 316-327.
-
WHO (2011) Step-by-step approach for development and implementation of hospital antibiotic policy and standard treatment guidelines, World health organisation, pp: 2-43.
-
De Francesco MA, Ravizzola G, Peroni L, Negrini R, Manca N (2007) Urinary tract infections in Brescia, Italy: etiology of uropathogens and antimicrobial resistance of common uropathogens. Med Sci Monit 13(6): BR136- 144.
-
Renuart AJ, Goldfarb DM, Mokomane M, Tawanana EO, Narasimhamurthy M, et al. (2013) Microbiology of urinary tract infections in Gaborone, Botswana. PLoS One 8(3): e57776.
-
den Heijer CD, Beerepoot MA, Prins JM, Geerlings SE, Stobberingh EE (2012) Determinants of antimicrobial resistance in _Escherichia coli_ strains isolated from faeces and urine of women with recurrent urinary tract infections. PLoS One 7(11): e49909.
-
Mukherjee M, Basu S, Mukherjee SK, Majumder M (2013) Multidrug-Resistance and Extended Spectrum Beta- Lactamase Production in Uropathogenic _E. coli_ which were Isolated from Hospitalized Patients in Kolkata, India J Clin Diagn Res 7(3): 449-453.
-
ICMR (2019) Treatment Guidelines for Antimicrobial Use in Common Syndromes Indian Council of Medical Research, pp: 1-201.
-
Saha S, Nayak S, Bhattacharyya I, Saha S, Mandal AK, et al. (2014) Understanding the patterns of antibiotic susceptibility of bacteria causing urinary tract infection in West Bengal, India. Front Microbiol 5: 463.
-
Gupta A, Chauhan B, Pethani J, Shah P (2016) Fluoroquinolones resistance among uropathogens at a tertiary-care hospital, Ahmedabad. Int J Med Sci Public Health 5(8): 1583-1587.
-
Tulara NK (2018) Nitrofurantoin and Fosfomycin for Extended Spectrum Beta-lactamases Producing _Escherichia coli_ and _Klebsiella pneumoniae_. J Global Infect Dis 10(1): 19-21.
-
Mandal J, Acharya NS, Buddhapriya D, Parija SC (2012) Antibiotic resistance pattern among common bacterial uropathogens with a special reference to ciprofloxacin resistant _Escherichia coli_. Indian J Med Res 136(5): 842- 849.
-
Sukumaran TS, Kumar KR (2017) Antimicrobial Resistance among Uropathogenic Bacteria in Rural Kerala, India. Int J Curr Microbiol App Sci 6(9): 2287- 2296.
-
Eshwarappa M, Dosegowda R, Aprameya IV, Khan MW, Kumar PS, et al. (2011) Clinico-microbiological profile of urinary tract infection in south India Indian J Nephrol 21(1): 30-36.
-
Patel HB, Soni ST, Bhagyalaxmi A, Patel NM (2019) Causative agents of urinary tract infections and their antimicrobial susceptibility patterns at a referral center in Western India: An audit to help clinicians prevent antibiotic misuse. J Family Med Prim Care 8(1): 154-159
-
Das UK, Bhattacharjee P, Debnath S, Chakraborty M, Ghosh R, et al. (2018) Antibiotic sensitivity pattern of bacterial isolates from urine samples of admitted patients with urinary tract infection in a tertiary care teaching hospital of Tripura, India: a hospital record based study. Int J Basic Clin Pharmacol 7(4).
-
Sultan A, Rizvi M, Khan F, Sami H, Shukla I, et al. (2015) Increasing antimicrobial resistance among uropathogens: Is fosfomycin the answer? Urol Ann 7(1): 26-30.
-
Banerjee S, Sengupta M, Sarker TK (2017) Fosfomycin susceptibility among multidrug-resistant, extended- spectrum beta-lactamase-producing, carbapenem- resistant uropathogens. Indian J Urol 33(2): 149-154.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report