What does a Bosniak Iv Renal Cyst Obscure?
One of the challenges urologists encounter when dealing with renal cysts is distinguishing between benign and malignant cystic tumours. Approximately 5-7 percent of renal malignancies have a cystic appearance, and clear cell renal cell carcinoma is the most common histological type found (half of the cases), followed by papillary carcinoma. Specific management should be performed in accordance with the Bosniak classification stage. Stage IV is a form of complex cystic tumour with a high risk of malignancy. We report the case of a 51 year old patient, followed for gout, in whom a left renal remanent cyst, measuring about 8 cm, was incidentally discovered during a routine check-up on abdominal ultrasound and classified as Bosniak IV on CT urogram. A left Neohrectomy was performed, and a pathologic examination revealed papillary carcinoma, stage pT2a (intermediate risk according to the UISS). The short- and long-term outcomes were both satisfactory, with a normal CT TAP six months after surgery and normal renal function. To summarise, a Bosniak IV renal cyst needs special attention and full surgical excision to reduce the risk of malignancy progression nd survival is unquestionably satisfactory.
Introduction
Distinguishing between benign and malignant cystic tumours is one of the challenges that urologists face when dealing with renal cysts. Approximately 5-7% of kidney cancers have a cystic appearance and the most common histological type is clear cell renal carcinoma in half of cases (56%) followed by papillary carcinoma [1, 2]. A special support must be made according to the Bosniak classification stage. Type IV Bosniak is a form of complex cystic tumour at high risk of malignancy [3], which requires uneven surgical management consisting of a complete surgical excision with acceptable survival at 5 years.
Thus we report a medical observation of a 51-year-old patient, followed for gout admitted for left renal cyst type Bosniak IV.
Observation
Patient M.Z., 51 years old, followed for gout (allopurinol 100mg/d and colcichine 1mg/d), who was admitted for management of a left renal cyst accidentally discovered on abdominal ultrasound. The clinical examination was normal. normal biological exams (hemoglobin at 13 g/dl creatinine at 7 mg/l ) and abdominal CT objectivated a left renal tumour mass, Lower solidokystic polar with peripheral tissue portion slightly enhanced after injection of contrast medium , measuring 76x37x78mm, Bosniak IV type, with absence of deep lymphadenopathy and secondary bone and visceral lesions. The renal pedicle was normal without intraluminal material (Figure 1) and the chest CT was without particularities.
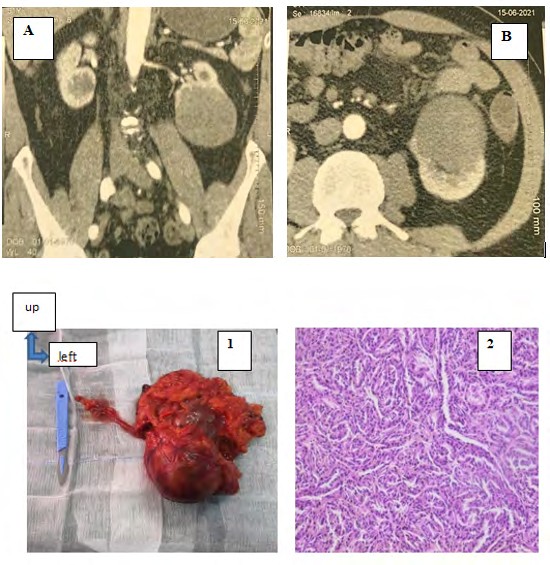
Figures 1: Frontal and transverse sections of CT scan: left renal tumour mass, inferior polar solid-cystic with peripheral tissue portion slightly enhancing after contrast medium injection, measuring 76x37x78mm, type Bosniak IV.
The left lumbotomy revealed a tumour mass of the left kidney, predominantly in the lower two-thirds of the kidney, solid cystic (Figure 2), with no lumbar adenopathy. A left nephrectomy was performed, and the pathologic examination of the surgical specimen revealed a papillary carcinoma type 2 (Figure 2), Furhman’s grade 2 classified as pT2a and intermediate risk according to the UISS (UCLA IntegratedStaging System).
Figures 2: Surgical specimen image of the left enlarged total nephrectomy and histological image noting nucleoli classifying the Furhman grade 2 tumour as papillary carcinoma (magnification 40).
The short and long term evolution was satisfactory , with a normal thoraco-abdominopelvic ct at 6 months and 1 year (no recurrence or lomboaortic adenopathy), as well as renal function and excellent healing.
Discussion
Cystic tumours are renal tumour proliferations with cavities. Histologically, a distinction is made between benign cystic tumours and renal tumours in which the cystitis is the result of an architectural change with malignant potential.
The frequency of cysts increases with age. Indeed, nearly 50% of the population over 50 years of age has a renal cyst [4]. Although most cysts are benign (simple cysts), 5-7% of malignant renal tumours have a cystic appearance [5]. Simple cysts tend to increase in number rather than size and are currently predominantly male [2].
Cysts are usually asymptomatic. As a result, most simple cysts are identified by chance during a radiological assessment required for another cause, as in our patient’s case. Large cysts can induce abdominal or lower back pain, and are sometimes associated with clinical mass syndrome. The cyst may constrict the excretory system and induce renal colic in fewer than 5% of patients. Acute or subacute pain should alert you to the risk of a cyst rupture, bleeding, or infection. Haematuria is a characteristic symptom of cyst rupture in the excretory system. Oedema and proteinuria might result from a cyst compressing the renal vein. Finally, renal cysts can produce arterial hypertension as a result of vascular compression caused by segmental renal ischaemia.
The Morton Bosniak CT classification is used to diagnose cystic masses on imaging [6]. To adequately characterise cystic lesions of the kidney, cross-sectional imaging (CT or MRI) is advised. Contrast ultrasonography may be used in the absence of CT or MRI, or as an addition to better characterise a complicated cystic tumour (Bosniak IIF or III)[7].
Bosniak type IV cysts are distinguished by a vascularised fleshy component, thick and uneven walls, and nodules or vegetations. The fleshy components have a strong contrast.
In our case, standard ultrasound data was insufficient for a firm identification of a cyst mass, thus we used CT to share depth because we lacked contrast ultrasonography. As a result, many authors no longer recommend using standard ultrasonography to characterise cystic tumours, but rather CT, MRI, and even contrast ultrasound [8].
Many authors now speculate on the advantages of contrast ultrasonography over CT [8, 9]. Rare cardiac events associated with the injection of gas microbubbles, however, have been described in the literature, and radiologists should be aware of them in patients with risk factors such as pulmonary hypertension, a history of myocardial infarction, or unstable heart disease. Finally, as with other ultrasound examinations, this approach has limits owing to inter- observer variability, and vision is occasionally obstructed by ribs or intestinal interpositions [10].
The initial risk of malignancy reported by Bosniak for each type was recently re-evaluated in a systematic review of the literature and found to be 86 percent (81-89 percent) for Bosniak IV [11]. Because of the high risk of malignancy, full surgical excision, as performed in our situation, is the preferred therapy.
Percutaneous biopsy in cystic tumours, on the other hand, is being studied and is not yet recommended [12].
Peroperative rupture of a cystic tumour is a frequent occurrence that constantly raises the issue of oncological risk. Some authors demonstrated that this rupture was not linked with a higher risk of recurrence and that the results were similar between robot-assisted laparoscopic surgery and open surgery [13]. Peroperative rupture should be avoided as much as possible, but it appears to have minimal oncological impact.
We proceeded with a complete kidney removal due to the altered and suspicious appearance of practically all of it.
Histology is crucial to understanding the other side of the Bosniak IV cyst. It should be emphasised that in 91 percent of cases, the Bosniak IV cyst indicates a malignant tumour of low stage (86 percent pT1-2), low grade (68 percent ISUP grade 1-2), and favourable prognosis (recurrence 1.1 percent, specific survival 100 percent) [14].
According to Bosniak stage, the following tumour features were observed in one study: clear cell carcinoma in 56% of cases, papillary carcinoma en 23% of cases. However, Bosniak category was not predictive of oncologic outcome with favourable and similar recurrence-free survival rates for Bosniak III and IV of 92% vs. 92% at 5 years and 84% vs. 83% at 10 years (p = 0.60) [2].
According to the UISS, the histological type detected in our patient was papillary carcinoma type 2, Furhman grade 2 classed as pT2a and intermediate risk. This histological type is the second most frequent after clear cell renal cell carcinoma, and type 2 often has a worse prognosis than type 1. However, in our case, we saw a decent survival without recurrence for a period of one year. They have a favorable prognosis ,in general, since they are not aggressive and are of low grade [14].
Conclusion
To summarise, a Bosnian IV renal cyst deserves specific attention and complete surgical treatment to avoid obscuring the risk of advancement of a hidden malignancy, even if survival is frequently satisfactory.
References
-
Nouhaud FX, Bernhard JC, Bigot P, Khene ZE, Audenet F, et al. (2018) Contemporary assessment of the correlation between Bosniak classification and histological characteristics of surgically removed atypical renal cysts (UroCCR-12 study). World J Urol 36(10): 1643-1649.
-
Boissier R, Ouzaid I, Nouhaud FX, Khene Z, Dariane C, et al. (2019) Long-term oncological outcomes of cystic renal cell carcinoma according to the Bosniak classification. IntUrolNephrol 51(6): 951-958.
-
Ljungberg B, Bensalah K, Canfield S, Dabestani S, Hofmann F, et al. (2015) EAU guidelines on renal cell carcinoma: 2014 update. EurUrol 67(5): 913-924.
-
Siegel CL, McFarland EG, Brink JA, Fisher AJ, Humphrey P, et al. (1997) CT of cystic renal masses: analysis of diagnosticperformance and interobserver variation. AJR Am J Roentgenol 169(3): 813-818.
-
Bielsa O, Lloreta J, Gelabert-Mas A (1998) Cystic renal cell car-cinoma: pathological features, survival and implications fortreatment. Br J Urol 82(1): 16-20.
-
Bosniak MA (2012) The Bosniak renal cyst classification: 25 years later. Radiology 262(3): 781-785.
-
Defortescu G, Cornu JN, Béjar S, Giwerc A, Gobet F, et al. (2017) Diagnostic performance of contrast-enhanced ultrasonography and magnetic resonance imaging for the assessment of complex renal cysts: A prospective study. Int J Urol 24(3): 184-189.
-
Park BK, Kim B, Kim SH, Ko K, Lee HM, et al. (2007) Assess-ment of cystic renal masses based on Bosniak classification:comparison of CT and contrast-enhanced US. Eur J Radiol 61(2): 310-314.
-
Quaia E, Bertolotto M, Cioffi V, Rossi A, Baratella E, et al. (2008)Comparison of contrast-enhanced sonographywithunenhancedsonography and contrast- enhanced CT in the diagnosis of malignancy in complex cystic renal masses. AJR Am JRoentgenol 191(4): 1239- 1249.
-
Ellimoottil C, Greco KA, Hart S, Patel T, Sheikh MM, et al. (2014) New modalities for evaluation and surveillance of com-plex renal cysts. J Urol 192(6): 1604-1611.
-
Schoots IG, Zaccai K, Hunink MG, Verhagen PCMS (2017) Bosniak Classification for Complex Renal Cysts Reevaluated: A Systematic Review. J Urol 198(1): 12-21.
-
Marconi L, Dabestani S, Lam TB, Hofmann F, Stewart F, et al. (2016) Systematic Review and Meta-analysis of Diagnostic Accuracy of Percutaneous Renal Tumour Biopsy. EurUrol 69(4): 660-673.
-
Pradere B, Peyronnet B, Delporte G, Manach Q, Khene ZE, et al. (2018) Intraoperative Cyst Rupture during Partial Nephrectomy for Cystic Renal Masses-Does it Increase the Risk of Recurrence. J Urol 200(6): 1200-1206.
-
Reese AC, Johnson PT, Gorin MA, Pierorazio PM, AllafME, et al. (2014) Pathological characteristics andradiographic correlates of complex renal cysts. Urol Oncol 32(7): 1010-1016.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report