What about the Intradiverticular Bladder Tumours at Ibn Rochd University Hospital?
Introduction: Bladder diverticula are urothelium herniations that pass through the bladder muscle. The perivesical fat is in direct contact with the urotheliumdiverticularis. As a result, tumours developing from the urotheliumdiverticularis have a distinct evolutionary history from classical bladder tumours and are rarely linked with a bad prognosis. Objective: To assess the management of intraverticular bladder tumours. Material and Methods: This is a retrospective study on intradiverticular bladder tumours from January 2012 to December 2017 (i.e. 6 years) at the urology department of Casablanca’s UH Ibn Rochd. The study included all patients with an intradiverticular bladder tumour and a complete file. Results: The mean age was 63.75 years (with extremes of 44 and 88 years) and the The delay between the onset of symptoms and the consultation was 12.83 months. In all cases, hematuria was the most common symptom for consultation. Smoking (66.66 percent) and recurrent urethritis were identified as two risk factors (16.67 percent). In 50% of the patients, ultrasound revealed a diverticulum with tumour material, and CT scans revealed a tumorous diverticulum in 6 cases. Urothelial carcinoma was the most frequent histological type (83.33 percent), followed by squamous cell carcinoma (16.67 percent). After surgery, the pT3 grade was the most prevalent. In three and nine cases, surgery was conservative and radical, respectively. After three years of follow-up, the majority of patients had a favourable outcome with no recurrence. Conclusion: Intraverticular bladder tumours differed from classical bladder tumours in that they had a higher frequency of T3a tumours and non-urothelial carcinomas, as well as a risk of underestimated extension and tumour multifocality. In the majority of cases, their prognosis is bleak.
Introduction
Bladder diverticula are urothelium herniations through the bladder muscle. The perivesical fat is in direct contact with the urothelium diverticular.
Intradiverticular bladder tumours are rare, with a prevalence of 0.8-13.5 percent and predominance in males over the age of 50 [1, 2, 3, 4, 5].
They appear in the majority of cases as acquired diverticula (due to a subvesical obstruction) and just rarely as congenital diverticula [3, 4].
Early extravesical invasion and poor survival are observed in diverticula due to the absence of a muscular layer [6, 7, 8, 9]. Furthermore, the diverticulum’s thin layer makes transurethral resection more challenging, with a larger risk of bladder perforation. As a result, diverticulectomy or partial cystectomy with or without early postoperative intravesical chemotherapy is usually the recommended treatment.
Material and Methods
This is a descriptive study with retrospective data collecting on intradiverticular bladder tumours (IDBT) at the UH Ibn Rochd of Casablanca from January 2012 to December 2017 (i.e. 6 years). All patients with an intradiverticular bladder tumour and a complete file were included in the study. Patients whose files could not be used were excluded.
classification of 2009 to determine the rate of short- and medium-term post-cystectomy complications to assess the postoperative status. For data analysis, we utilised Epi info.7, and for graphing, we used Excel version 2007. Quantitative variables were reported as means standard deviation, and qualitative variables as number and percentage. For percentage comparisons, the Pearson Chi-square (x2) test was employed, and the p-value of the probability was considered significant if it was less than or equal to 0.05.
Results
Epidemiology and Clinic
We had 12 cases in 6 years or 2 cases each year. All patients were male, with a mean age of 63.7512.84 years and extremes ranging from 44 to 88 years, and the most common symptom for consultation was haematuria (Table 1). The delay between the onset of symptoms and the consultation was 12.83 months (extremes from 6 to 24 months.
| n(%) | ||
|---|---|---|
| Antecedent | Smoking | 8(66,67) |
| Antecedent | Urethritis | 2(16,67) |
| Antecedent | 2(16,67) | |
| Symptom | Hematuria | 9(75) |
| Symptom | Hematuria and lower urinary tract symptoms | 3(25) |
| Clinical Examination | Alteration of the general condition, infiltrated bladder base and prostate enlargement | 2(16,67) |
| Clinical Examination | Normal | 10(83,33) |
Table 1: Patient distribution based on clinical data.
Paracliniques
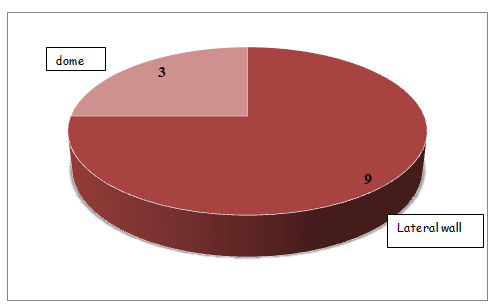
Urinary tract ultrasonography: On ultrasonography of the urinary tract, 11 patients had a diverticular bladder, and 6 patients had a diverticulum with tumour content. In two cases, we found a multidiverticular bladder, and in four cases, we found a single diverticulum positioned latero-vesically. In seven cases, benign prostatic hypertrophy was identified as an obstacle. Computed tomography urogram (CTU): Prior to endoscopic resection, ten patients had a CTU; in all cases, the diverticulum was tumorous and mostly in the lateral wall (7 cases), with 2 cases trigonal and 1 case in the bladder dome.
Endoscopy revealed that eight cases had a peridiverticular bladder tumour, with the diverticulum in three cases being positioned at the level of the dome (Figure 1).
The majorities of intradiverticular tumour resections were biopsy (75 percent of cases) and complete (25 percent of instances).
Endoscopy
Revealed that eight cases had a peridiverticular bladder tumour, with the diverticulum in three cases being positioned at the level of the dome [1].
The majority of intradiverticular tumour resections was biopsy (75 percent of cases) and complete (25 percent of instances).
Histology
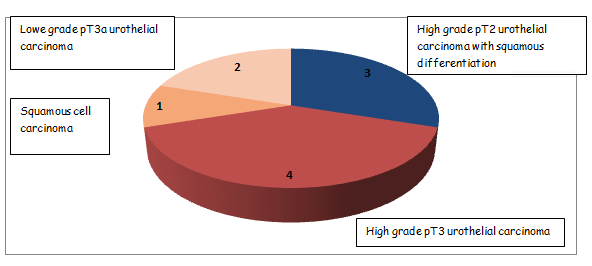
Urothelial carcinoma (10 cases) was the most common histological type, followed by squamous cell carcinoma in two cases (Table 2). The tumors classified as pT2 involved either the neck or the rest of the bladder wall.
| n | % | ||
|---|---|---|---|
| Urothelial Carcinoma pT1 | Low grade | 2 | 16.7 |
| High grade | 3 | 25 | |
| Urothelial carcinoma pT2 | 3 | 25 | |
| Urothelial carcinoma pT3 | 2 | 16.7 | |
| Squamous Cell Carcinoma | 2 | 16.7 | |
| Total | 12 | 100 |
Table 2: Distribution of patients according to histology after endoscopic resection.
Treatment
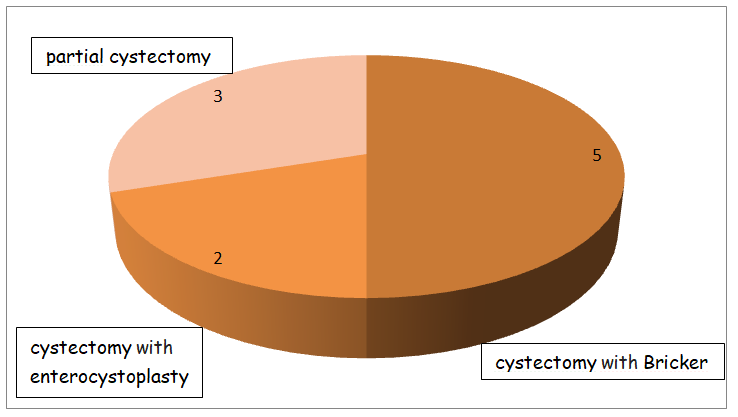
Medical: Two patients had been treated with radio chemotherapy and three with BCG immunotherapy combined with partial cystectomy. Surgical: In three cases, a was performed (Figure 2). There was one case of paralytic ileus, one case of parietal suppuration, and one case of urinary retention after orthotopic neobladder.
Evolution
We had two Lost cases to follow-up (Table 3) (Figure 3).
| n | % | |
|---|---|---|
| Normal cystoscopy at 3 and 6 months and every 3 months for 3 years | 1 | 8,33 |
| Normal cystoscopy at 3 and 6 months and every 3 months for 3 years and normal TAP scan | 2 | 16,67 |
| Lost to follow-up | 2 | 16,67 |
| Normal TAP scan and biological assessment at 3, 6 and 12 months | 2 | 25,00 |
| Normal TAP scan at 3 and 6 months | 2 | 16,67 |
| Normal TAP scan at 3 months | 2 | 16,67 |
| TOTAL | 12 | 100 |
Table 3: Distribution of patients according to follow-up.
Discussion
Bladder diverticula are urothelium herniations through the bladder muscle. The perivesical fat is in direct contact with the urothelium diverticular. As a result, tumours developing from the urothelium diverticularis have been described as having a different evolutionary profile from classic bladder tumors [1].
Bladder diverticula are, by definition, devoid of muscularis. Bladder diverticula are, by definition, devoid of muscularis. They therefore have no contractile function.
Their filling and emptying is passive. The quality of diverticular emptying depends on the diameter of the neck and the gradient of its implantation.
The prevalence of intradiverticular bladder tumours is estimated to be between 1 and 10% in the general population with an average of 4% [2, 3, 4]. In our study, spread over a period of 6 years, we found 12 cases, i.e. 2 cases/year.
Diverticula were mostly secondary to hyperpressure micturition caused by a chronic urethral obstruction, most often prostatic [5, 6, 7]. More rarely, diverticula were of congenital origin. Our study agrees with the results of the literature in finding a prostatic obstacle in 58% of cases.
Eighty percent of diverticula are the location of parietal alterations such as dysplasia, leukoplakia, or squamous metaplasia, while the remaining two to thirteen percent are the bed of malignant tumour processes [8, 9, 10]. In our series, a tumoral diverticulum predominates in the bladder’s lateral wall.
In addition to the classical aetiological factors of bladder tumours, the risk of tumour occurrence in a bladder diverticulum is increased by urinary stasis and chronic inflammation, responsible for chronic irritation of the mucosa, source of dysplasia and malignant transformation.
The diagnostic circumstances are unspecific, with haematuria being the most common symptom in 70-90 percent of patients. The other symptoms are frequently linked to the cervicoprostatic obstruction. Conventional radiological investigations (intravenous urogram and retrograde cystography) are ineffective; the intradiverticular lacuna is seldom seen and can be misinterpreted as lithiasis or a blood clot; the tumour can also obstruct the diverticulum’s neck, rendering it mute [11, 12].
The performance of conventional bladder ultrasonography in the diagnosis of IDBT has been reported as poor [13, 14], although it can detect a tumour in a big diverticulum or a latero-vesical mass. On the other hand, we found a diverticular bladder in 91.6 percent of cases using an ultrasound of the urinary tract, and the diverticulum was tumorous in 6 cases.
Computed tomography and, in particular, magnetic resonance imaging are the best diagnostic techniques [11, 12] because of their multidirectional slices and excellent resolution after contrast medium injection. They help determine the extent of the tumor, looking for extension into the peri-vesical fat in particular. Before endoscopic resection, ten patients in our study underwent a CT scan; in all cases, the diverticulum was tumorous, with a preponderance of the lateral wall of the bladder, with no explanation.
The interior of the diverticula had to be seen during an endoscopic diagnosis of IDBT, which was often challenging due to their angulation in reference to the bladder neck or the narrowness of the diverticular neck. For these reasons, fibroscopy using a flexible endoscope has proven to be more effective than a rigid cystoscope in diagnosing IDBT. Fibroscopy has been demonstrated to correctly identify 60% of IDBT cases [15, 16, 17].
Endoscopic resection of IDBT has the same goals as endoscopic resection of any bladder tumour: full resection of the tumour without perforation of the bladder. The restricted angle of view due to the rigidity of the material and the narrowness of the diverticular neck were the peculiarities of resection in a diverticulum.
The absence of the bladder muscle increased the risk of bladder perforation while respecting IDBTs. Others have advised using cold forceps biopsy to limit the risk of perforation, particularly during removing the IDBT’s base [16, 18]. We found 8 cases with a peridiverticular bladder tumour and 3 cases of dome diverticulum in our study. Resection of the intradiverticular tumour was biopsy in the majority of cases (75%) and complete in 25%.
The diverticular mucosa, by definition, does not rest on the bladder muscle, but rather has a direct contact with the perivesical fat. As a result, IDBT cannot be classed as T2 (muscle invasion tumour), but will instead advance from Ta- T1 to T3 (muscle invasion tumour) (tumour invading the perivesical fat or adjacent organs by contiguity). This IDBT feature is thought to be responsible for the estimated 55- 60% of tumours detected at stage T3 [18, 19]. Many authors have suggested that all IDBTs be treated as invasive tumours from the beginning [1, 19, 20, 21, 22, 23].
The histological diagnosis of IDBT has sometimes been made difficult by two phenomena:
- Peridiverticular fibrosis, characterised by thickening and fibrous densification of the lamina propria, which may give the tumour a margin of progression before reaching the perivesical fat [2].
- The mucosal muscle may be hypertrophic and confused with the bladder muscle [24].
- The predominant histological type was urothelial carcinoma in 83.3% and in two cases we noted squamous cell carcinoma.
- The Cancer Committee of the French Association of Urology recommends the following recommendations [25] based on the results presented in the literature:
- Transurethral resection alone is the usual therapy for Ta- T1 low-grade, unifocal IDBT without concomitant cancer in situ, assuming that it is complete and without bladder perforation.
- BCG therapy may be used to treat T1 tumours.
- Diverticulectomy or partial cystectomy is a therapy option for T1 low-grade, unifocal IDBT without concomitant cancer in situ if good margins are maintained. Extemporaneous examination and node dissection should be undertaken.
- Total cystectomy with pelvic lymph node dissection is the recommended therapy for IDBT > 1 or high grade or multifocal or accompanied with cancer in situ.
Our study revealed ten cystectomy cases, seven complete and three partial, with just one patient receiving radiochemotherapy and a good one-year overall survival.
The prognosis for IDBT is poor, with less than 10% survival at five years due to the delay in diagnosis, the thinness of the diverticular wall, which favors rapid progression of the tumour from a superficial to an infiltrative stage, and a recurrence rate of 62 percent between three and 36 months, according to the literature.
However, despite the fact that survival was satisfactory at one year, we are unable to extrapolate our study results because our sample was small and the survival time was so short at one year on the one hand, and we had patients lost to follow-up on the other, the retrospective nature of the study is the source of many biases.
Conclusion
IDBTs varied from classic bladder tumors in that they had a higher frequency of T3a tumours and non-urothelial carcinomas, as well as a risk of misdiagnosed extension and tumour multifocality. The majority of the cases, their prognosis is poor.
References
-
Bouchot O, Zerbib M (2002) Tumeurs urothéliales intradiverticulaires de vessie. ProgUrol 12: 1109-1111.
-
Golijanin D, Yossepowitch O, Beck SD, Sogani P, Dalbagni G (2003) Carcinoma in a bladder diverticulum: presentation and treatment outcome. J Urol 170(5): 1761-1764.
-
Melekos MD, Asbach HW, Barbalias GA (1987) Vesical diverticula: etiology, diagnosis, tumorigenesis, and treatment. Analysis of 74 cases. Urology 30(5): 453-457.
-
Lowe FC, Goldman SM, Oesterling JE (1989) Computerized tomography in evaluation of transitional cell carcinoma in bladder diverticula. Urology 34(6): 390-395.
-
Kelalis PP, McLean P (1967) The treatment of diverticulum of the bladder. J Urol 98(3): 349-352.
-
Boylan RN, Greene LF, McDonald JR (1951) Epithelial neoplasms arising in diverticula of the urinary bladder. J Urol 65(6): 1041-1049.
-
Montague DK, Boltuch RL (1976) Primary neoplasms in vesical diverticula: report of 10 cases. J Urol 116(1): 41- 42.
-
Peterson LJ, Paulson DF, Glenn JF (1973) The histopathology of vesical diverticula. J Urol 110(1): 62- 64.
-
Micie S, Ilic V (1983) Incidence of neoplasm in vesical diverticula. J Urol 129(4): 734-735.
-
Fellows GJ (1978) The association between vesical carcinoma and diverticulum of the bladder. EurUrol 4(3): 185-186.
-
Dondalski M, Maureen White E, Ghamremani GG, Patel SK (1993) Carcinoma arising in urinary bladder diverticula. AJR 161 (4): 817-820.
-
Sara M, Lawrence H, David M, Paulrusso (1997) MR imaging of carcinoma within urinary bladder diverticulum. Clin Imaging 21(4): 290-292.
-
Fekak H, Rabu R, Joual A, Bennani S, Moufid K, et al. (2002) Les tumeurs de vessie intradiverticulaires À propos de trois cas. Ann Urol (Paris) 36(1): 53-57.
-
Stamatiou K, Moschouris H, Papadaki M, Perlepes G, Skolarikos A (2011) Accuracy of modern ultrasonographic techniques in the follow up of patients with superficial bladder carcinoma. Med Ultrason 13(2): 114-119.
-
Rozet F, Pfister C, Planet M, Sibert L, Grise P (1997) Tumeur de vessie intradiverticulaire À propos de 5 cas. ProgUrol 7(2): 225-228.
-
Aubert J, Dombriz M, Dore B (1982) Tumeurs de vessie intradiverticulaires À propos de 3 cas. J Urol (Paris) 88: 537-540.
-
Montague DK, Boltuch RL (1976) Primary neoplasms in vesical diverticula: report of 10 cases. J Uro 116(1): 41- 42.
-
Tamas EF, Stephenson AJ, Campbell SC, Montague DK, Trusty DC, et al. (2009) Histopathologic features and clinical outcomes in 71 cases of bladder diverticula. Arch Pathol Lab Med 133(5): 791-796.
-
Gattegno B, Chopin D (2001) Diverticule vésical et tumeurs superficielles de la vessie. Prog Urol 11: 1145- 1148.
-
Faysal MH, Freiha FS (1981) Primary neoplasm in vesical diverticula. A report of 12 cases. Br J Urol 53(2): 141- 143.
-
Abeshouse BS, Goldstein AE (1943) Primary carcinoma in a diverticulum of the bladder: a report of four cases and a review of the literature. J Urol 49(3): 534-547.
-
Redman JF, McGinnis TB, Bissada NK (1976) Management of neoplasms in vesical diverticula.Urology 7(5): 492- 494.
-
Rozet F, Pfister C, Planet M, Sibert L, Grise P (1997) Tumeur de vessie intradiverticulaire À propos de 5 cas. ProgUrol 7(2): 225-228.
-
Hansel DE, Paner GP, Nese N, Amin MB (2011) Limited smoothelin expression within the muscularis mucosae: validation in bladder diverticula. Hum Pathol 42(11): 1770-1776.
-
Neuzillet Y, Comperat E, Rouprêt M, Larre S, Roy C, et al. (2012) Tumeurs de vessie intradiverticulaires : revue du Comité de cancérologie de l’Association française d’urologie. Progrès En Urologie 22(9): 495-502.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report