Laparoscopic Drainage of a Kidney Abscess in a Difficult Location: A Case Report
Introduction: We present a case of a kidney abscess of difficult localization and due to Proteus mirabilis. Presentation of the Case: It is a 29-year-old male patient with no pathological history who presented with left low back pain with intermittent feverish sensation 2 weeks before his admission. The physical examination noted left lumbar tenderness and a fever of 38.50C. The biological assessment noted hyperleukocytosis with polymorphonuclear neutrophils predominance and an elevation of C-reactive protein with infected urine. Initially objectified by ultrasound, an uro-computed tomography was performed and revealed an anterior superior polar abscess of the left kidney measuring 6cm in diameter. Faced with the impossibility of percutaneous radiological drainage, we resorted to laparoscopic drainage and continuation of antibiotic therapy with successful evolution. Discussion: Kidney abscesses are rare and sometimes with difficult location, which compromises the therapeutic approach. Their prevalence varies from 1 to 10 per 10,000 admissions with serious vital or functional complications. The most frequently found germs are Gram-negative bacilli. Ultrasound and especially CT scan make the diagnosis in 90% of cases and guide treatment. Antibiotic therapy alone or associated with percutaneous drainage depending on the abscess size constitutes the basis of treatment; surgical drainage is reserved for failure or impossibility of percutaneous drainage. Laparoscopy drainage constitutes an alternative of drainage in this situation. Conclusion: Kidney abscesses constitute a rare pathology but with consequences that can compromise the vital or functional prognosis of the kidney. Proteus mirabilis is a rare germ but commonly responsible for kidney abscesses. The clinic and methods of diagnosis of this abscess are identical to those due to other germs. Antibiotic therapy associated with imageguided percutaneous drainage was successful in the majority of cases. Drainage by laparoscopy is an alternative for draining abscesses in difficult locations when percutaneous drainage is impossible or fails.
Introduction
Kidney abscess is a pathology that is often the result of bacterial infections by colonization of the urinary tract or rarely from a remote infectious focus that is untreated or poorly treated [1]. Since the advent of means of renal exploration and especially the progress of antibiotic therapy, this condition has become rare with often a good evolution under adequate treatment but it can in certain cases compromise the functional prognosis of the kidney or even the vital prognosis [2]. Although the principle of treatment has not much changed since 1987, kidney abscesses are sometime important in size with difficult location and variable content, which often pose a problem in the therapeutic approach. In some cases, antibiotic therapy alone may be sufficient, but often it must be combined with percutaneous or surgical drainage [1]. We report the case of a 29-year-old patient, with no medical history or comorbidities, admitted to our department for a 6cm left kidney abscess of difficult location and whose urinary tract infection with Proteus mirabilis was identified as the etiology. The aim of this study was to propose the laparoscopic route as an alternative to drainage in the face of a kidney abscess of difficult location.
Case Report
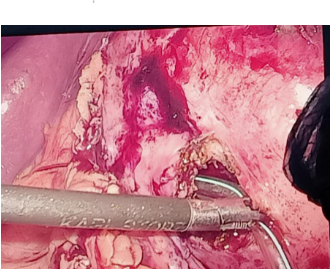
This is a 29-year-old male patient with no pathological history who presented left low back pain with intermittent feverish sensation for 2 weeks before admission. The interrogation did not find any pathological history except for urinary tract infection treated by oral antibiotic therapy a few days before his admission. The physical examination noted left lumbar tenderness and a fever of 38.50C, a stable hemodynamic state and normal consciousness. The complementary biological assessment noted white blood cells at 14,000 elements / mm3, predominantly polynuclear neutrophils, normal hemoglobin at 12g / dl, increased C-reactive protein at 130mg / l, normal renal function with plasma creatinine at 9mg / L and potassium at 4.4 mmol/l. The cytobacteriological examination of the urine was carried out and Protéus mirabilis was the isolated germ. Discovered firstly on ultrasound Figure 1, a confirmation uro-computed tomography (uroCT) showed an anterior superior polar abscess of the left kidney measuring 6cm in diameter (Figure 2). Faced with the impossibility of percutaneous drainage, laparoscopic drainage was resorted after intravenous antibiotic therapy for 48 hours. Under general anesthesia, on the right lateral decubitus position, the laparoscopic approach was performed. Exploration showed a left upper anteropolar abscess which was evacuated with drainage of a residual cavity through a drainage tube (Figure 3). The sample of pus for bacteriological analysis was made in peroperative. The drain was left in place for about a week and then removed after control by uro-CT of the effectiveness of abscess laparoscopic drainage. The postoperative consequences were simple. A bacteriological sample of the collection taken during the operation found the same germ as in the cytobacteriological examination before the procedure and the antibiotic therapy associating cephalosporins, aminoglycoside and antianaerobic was maintained with good clinical, biological and radiological evolution.

Discussion
Kidney abscess is a rare condition but can in some cases compromise the vital prognosis if not the functional prognosis of the kidney. Their prevalence varies from 1 to 10 per 10,000 admissions without sex differentiation with formidable vital or functional complications. Too large a volume of the collection, too thick a content, the existence of partitions or the superior polar location of a renal abscess often pose a problem for the therapeutic approach, which can go as far as surgical drainage of the abscess [1]. The diagnosis is based on radiological explorations given the lack of specificity of the clinical examination and biology. Thus, computed tomography has become the examination of choice in the diagnosis of kidney abscess and in the precise study of the extension towards the perirenal atmosphere to the detriment of ultrasound [3, 4]. In our case, the uro- computed tomography was the means of confirmation used and had objectified a left renal abscess of 6 cm superior anteropolar location (Figure 2). Although our case did not present a history of pathologies found, infections of the local urinary tract or at a distance from the poorly or insufficiently treated urinary tract constitute the main etiologies of this pathology and this by two mechanisms often mentioned: colonization of the urinary tract ascending urinary tract and rarely hematogenous spread from a focus remote from the urinary tract. The germs commonly involved are gram- negative bacilli, which match our case where Protéus mirabilis was identified before drainage but also in the intraoperative sample. However, other germs such as clebsiella, E. Coli, colibacillus and staphylococcus aureus are not spared. Also, diabetes mellitus, immunosuppression and especially lithiasic urological pathology proved to be predisposing factors [1, 5] but no factor was found in our case. In some cases antibiotic treatment alone is sufficient [6]. However, this exclusive antibiotic therapy is disputed in other studies which systematically indicate a gesture of drainage of the abscess whatever its size, thus making it possible to shorten the hospital stay. Often, this involves additional percutaneous drainage performed under ultrasound or CT monitoring depending on the location and size of the lesion. The multi- perforated catheter used will be larger the thicker the pus is. Although percutaneous drainage was successful in 80% of cases, which agrees with the data in the literature, this technique is sometimes compromised and doomed to failure as proven by Hung C, et al. [7] but also by Levin D, et al. [8]. Failures are related to too large a volume of the collection, too thick a content, the existence of partitions or a difficult- to-access location such as the upper polar seat, which leads to surgical drainage [9]. This illustrates our case in which the abscess was superior anteropolar, which motivated the use of laparoscopic drainage as an alternative to open surgery. The laparoscopic approach was successfully used (Figure 3). Although complications resulting from drainage, especially surgical drainage, are not negligible (8 to 10% of cases) such as hemorrhage, fistula, septic shock, pneumothorax [10], no complication was reported in our study case.
Conclusion
Although kidney abscesses are rare, they have consequences that can compromise the vital or functional prognosis of the kidney. Proteus mirabilis is a rare germ but commonly responsible for kidney abscesses. The clinic and diagnostic methods of are identical to those due to other germs. Treatment with antibiotics associated with image- guided percutaneous drainage is successful in the majority of cases. The upper polar or anteropolar seat is a difficult location that compromises the principle of percutaneous drainage. Through our experience, drainage by laparoscopy constitutes an alternative for the drainage of abscesses of difficult location in the face of the impossibility or failure of percutaneous drainage.
Consent
Consent from the patient was obtained.
Conflict of Interest
None.
Acknowledgments
At the end of this work, we would like to sincerely thank all the people who contributed to its writing. Many thanks to the radiology and laboratory staff for your complementary examination. To all our teachers for your teaching and your dedication, we thank you very much.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
-
Dembry LM, Andriole VT (1997) Renal and perirenal abscesses. Infect Dis Clin 11(3): 663-680.
-
An SW, Yoon CJ, Seong NJ, Kang SG, Han HS, et al. (2013) Inaccessible abdominal abscess: percutaneous drainage technique with puncture of a sinus tract. J Vasc Interv Radiol 24(4): 586-591.
-
Best CD, Terris MK, Tacker JR, Reese JH (1999) Clinical and radiological findings in patients with gas forming renal abscess treated conservatively J Urol 162(4): 1273-1276.
-
You K, Bellin MF, Bitker MO, Bousquet JC, Chatelain C, et al. (1988) Lésions infectieuses focales du parenchyme rénal : apport comparé de l’échographie et de la TDM. J Radiol 69: 509-516.
-
Hanno Philip M, Guzzo Thomas J, Bruce Malkowitz S, Wein Alan J (2014) Penn Clinical Manual of Urology. In: Lower Urinary Tract Infections in Women and Pyelonephritis. 2nd (Edn.), Elsevier Saunders, Philadelphia, pp: 130.
-
Dalla palma L, Pozzi-mucelli F, Ene V (1999) Medical treatment of renal and peri renal abscesses: Computerised tomographyevaluation. Clin Radiol 54(12): 792-797.
-
Hung CH, Liou JD, Yan MY, Chang CC (2007) Immediate percutaneous drainage compared with surgical drainage of renal abscess. Int Urol Nephrol 39(1): 51-55.
-
Levin DC, Eschelman D, Parker L, Rao VM (2015) Trends in use of percutaneous versus open surgical drainage of abdominal abscesses. J Am Coll Radiol 12(12): 1247- 1250.
-
Anderson KA, Mcaninch JW (1980) Renal abscesses: Classification and review of 40 cases. Urology 16(4): 333-338.
-
Safir MH, Schaeffer AJ (1997) Urinary tract infection: Simple and complicated. AUA update series 16, lesson 10.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report