The Evolution of Penile Prosthesis in the Treatment of Erectile Dysfunction
The National Institutes of Health consensus on impotence has defined erectile dysfunction in 1993 as the persistent inability of male to achieve and/or maintain an erect penis to allow satisfactory sexual intercourse. This condition affects millions of men of any age, but its prevalence is closely associated with aging, and it is estimated that about fifty percent of men, aged 40-70, experience some degree of erectile dysfunction. Penile prosthesis has been part of the therapeutic alternatives of erectile dysfunction for several decades. However, in the ‘90s, with the arrival of type-5 phosphodiesterase inhibitors, the treatment of erectile dysfunction evolved significantly. This class of drugs, which is currently considered the first line of treatment, is ineffective in about 30% of patients whom continue to require more invasive treatments. Penile prosthesis has high satisfaction and efficacy rates in the management of erectile dysfunction, and they undergone through some evolutions in the past years. This article intent to underline the evolution of the penile prosthesis in the treatment of erectile dysfunction with their virtues and disadvantages.
Introduction
Erectile Dysfunction (ED) represents one of the most universal health problems since the beginning of the human species, with the Ebers Papyrus emerging as the first description of this disease, dating from 1550 B.C [1].
ED is a multifactorial disease that is related to vascular, neurological, psychological and even hormonal causes. Some of the conditions, implicated in the genesis of the disease, have a high prevalence in the population, such as diabetes mellitus (DM), hypertension, dyslipidemia, obesity, smoking, alcohol, drugs (such as marijuana), medication (such as antidepressants), testosterone deficiency, side effects of prostate cancer treatment (surgery, radiation or hormonotherapy) or anxiety and other psychological conditions [2].
Currently, there is a range of treatments available, with type-5 phosphodiesterase inhibitors (PDE5i), discovered in the 90’s, being in the first line of treatment. However, its therapeutic efficacy remains around 60-70% [3].
Although PPs are the last treatment resource, with the constant technological evolution verified in this branch, they have become an excellent therapeutic alternative with low rates of complications and high rates of satisfaction of the patient and most of all of the couple, making it a highly effective treatment [1].
By definition, a PP is a device that is implanted in the corpora cavernosa in order to mimic an erection by the most natural way possible, both in appearance and function. The first PPs used for therapeutic purposes date back to 1950. Since then, there has been an interest for innovation both in the technology used in the prostheses, as well as in the surgical technique, with the great objective of improving the quality of life by reproducing a physiological erection and not harming other functions of the human body, such as the urinary system [4].
The objective of this study is to provide a narrative review, in a systematic way, of the PPs currently used in the treatment of ED, according to the translational studies available.
Methods
A comprehensive literature review was performed using PubMed, ScienceDirect, National Institute of Health (NIH), The Journal of Sexual Medicine (JSM) and International Journal of Impotence Research (IJIR) to identify relevant articles published in the fields of medicine and urology until January 2020.
The search was conducted using a free-text protocol and included the following terms: “Erectile Dysfunction”, “Penile Prosthesis”, “Medical Devices”and “Satisfaction”.
Results
Historical Background
The first attempt, in the modern era, to reconstruct the penis was made in the 30’s with the intention of being just a channel for urination [5].
However, Borgus, a german surgeon, is widely regarded as the first doctor to attempt, in 1936, to implant an artificial penile device to treat ED, in the context of soldiers who suffered traumatic penile injuries [5, 6].
In the transition from the 60’s to the 70’s, there was an advance, both in surgical technique and in the materials used, which contributed positively to the modernization, efficacy and safety of penile implant surgery. Egyptian surgeon Beheri was the first to use intracavernous polyurethane cylinders with reports of an erect, more rigid and less painful penis. However, these PPs still had high rates of complications due to mechanical problems related to the prosthesis, resulting in low levels of satisfaction and acceptance, being subsequently discontinued [5, 6, 7].
The latest major development in technology that led to today’s inflatable PP belongs to the National Aeronautics and Space Administration (NASA), which developed an high quality silicone as part of a space program that later served as the basis for the development of many PP used in humans, including those used to treat ED [5].
The first modern PPs were developed in the early 70’s, when Small and Scott described the implantation of these devices in the corpora cavernosa, in order to provide a physiologically functional erection with good aesthetic results. In its initial description, in 1973, the device consisted of three components: two inflatable silicone cylinders, a fluid reservoir and two control pumps, one in each hemiscrotum. The device caused the desired rigidity of the penis through a mechanism that made the transfer of fluid from the reservoir to the intracavernous cylinders, when a pump was pressed. When not in use, the fluid returned to the reservoir when another pump was tightened. This hydraulic mechanism better mimicked a physiological erection in the flaccid and rigid states than previous devices, however it still suffered from a significant percentage of mechanical failures. Through multiple revisions, Scott and Small designed the inflatable PPs that are currently used. Scott also commercialized the first generation of inflatable PPs, through the American Medical Systems (AMS) [5, 6, 7].
In 1974, doctors Michael Small and Hernan Carrion introduced their competing device, a precursor to semi-rigid prostheses, the Small-Carrion prosthesis. However, this had as a big con, the fact that it didn’t mimic the flaccid state of a penis. This problem was overcome by the doctor Subrini through the use of a softer silicone allowing the device to be folded down when not in use, allowing a better hiding of the device (4.22).
Currently, the market gives priority to inflatable PPs and is dominated by two companies, Boston Scientific (formerly AMS) and Coloplast (formerly Mentor). However, both companies still manufacture semi-rigid PPs (22).
Theoretical Background
Despite the introduction of PDE5 inhibitors, PPs remain a relevant and desired option, as many men become refractory or have contraindications to oral, topical and injectable pharmacological therapies and/or seek a more effective and permanent treatment. Cases of these situations are, for example, ED caused by serious systemic diseases, such as DM, hypertensive arterial syndrome or neurological disorders, due to occlusions of arteriogenic and/or veno- occlusive cause. Pelvic surgery that does not spare nerves, performed on the prostate, bladder and rectum, is another major cause of ED, due to the interruption of neuro-vascular bundles involved in erectile mechanisms [6, 8].
The first step in the implantation of a PP is to obtain informed consent, discussing with the patient and his spouse, in order to understand the expectations and fears in relation to the treatment, and to rule out any unrealistic ideas, such as the fact that this device does not aim to improve libido or ejaculatory function. The patient must know that the placement of the device implies the destruction of the corpora cavernosa and, for this reason, it must be considered an irreversible procedure with regard to a possible spontaneous erection after surgery. The surgeon must present the various devices available on the market, personalized to the patient. An important aspect to be highlighted is the high level of satisfaction expressed by patients who have already undergone this type of treatment. In spite of this, the patient must know that the use of a PP is not immune from complications and they can occur, even with low probability; the main ones are infection, erosion and mechanical malfunction of the device [8, 9].
PPs are currently divided into two large groups depending on the type of treatment: semi-rigid and inflatable (one, two or three components). Both types of PPs have the main objective of obtaining a state of rigidity. However, the differences are related to the aesthetic result and the possibility of obtaining a natural flab [8].
Semi-rigid prostheses have a mechanism to obtain the simplest erection and, therefore, the advantages are related to greater ease of use, greater mechanical reliability and the use of a more simple surgical procedure, compared to inflatable prostheses; however, the main disadvantage is that it does not achieve a state of flaccidity, although the erect penis can be oriented in different positions [8].
Inflatable prostheses, especially those with three components, are considered more sophisticated and complex than the other types because they have the great advantage of mimic the state of erection and flaccidity as well as a better aesthetic result. The disadvantages are related to a greater probability of less technical reliability and the need for a more complex surgical technique [8].
However, with the modernization and globalization of surgical techniques, the length of hospital stay is generally short due to the high success and low complication rates. Although the results are mainly positive, there is always a small rate of possible complications, which can happen in the perioperative, operative and / or postoperative periods [8].
To simplify the surgical procedure, two-component inflatable prostheses were designed due to the removal of the reservoir. Although these devices provide adequate erection in many patients, the limited capacity of the reservoir decreases sagging and may, in some patients, decrease stiffness [10].
Prostheses are relatively contraindicated in cases of recurrent urinary infections and in situations that may increase the risk of local infections, such as spinal cord injury, uncontrolled DM and immunosuppressive therapies. Patients with low motivation or wrong expectations shouldn’t also undergo a PP implant. Above all, the use of these devices requires a patient who is motivated and supported by his partner [8, 9].
Types of Penile Prostheses
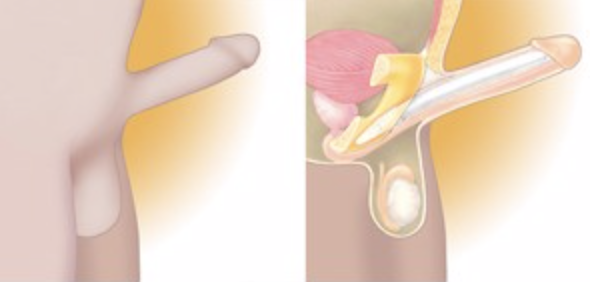
One-component inflatable PPs: One component inflatable prosthesis consists essentially of two cylinders, with the particularity of each containing an incorporated reservoir, which contains the fluid that fill the cylinders to simulate the erection Figure 1 [6].
In the 80’s, two models of this type were introduced: the Flexi-Flate prosthesis from Surgitek and the AMS Hydroflex prosthesis (succeeded by AMS Dynaflex) [6].
However, these devices proved to be inferior to inflatable prostheses with two or three components, in terms of mechanical reliability and patient satisfaction with the aesthetics and stiffness achieved [6].
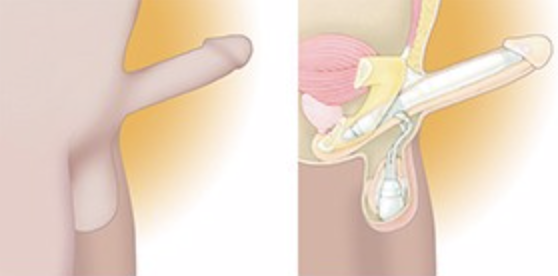
Two-component inflatable PPs: Two-component PPs were designed with the objective of reducing complications and increasing the success rate of surgeries. Generally, they consist of two cylinders connected to a pump. Since the reservoir is absent in this prosthesis, the fluid is provided by a larger scrotal pump. Although these devices provide adequate erection in many patients, the limited capacity of the reservoir decreases flaccidity and may, in some patients, decrease stiffness Figure 2 [10].
For this reason, although less optimized than three-
piece devices, these types of prostheses may be indicated in patients in which the placement of reservoirs is contraindicated or difficulties by anatomical specificities and / or prior pelvic surgeries. Kidney transplant recipients and patients submitted to cystectomy or prostatectomy, can benefit from this type of PP [10, 11].
The main prostheses described were the Mentor GFS models (succeeded by the Mark-II), Sugiteck Uniflate 1000 and the AMS Ambicor, the only one currently available [6].
Three-component inflatable PPs: The inflatable PP of three components are made up of three separate pieces: a pair of cylinders implanted in the corpora cavernosa, a pump implanted in one hemiscrotum and a reservoir implanted in the lower abdomen Figure 3 [6].
The PPs, generally, all work through manual compression of the pump, which transfers the fluid from the reservoir to the penile cylinders, causing them to inflate and become rigid, thus allowing coitus. When an emptying valve, also located at the level of the scrotal pump, is pressed, the cylinders are deflated and the fluid returns to the intra-abdominal reservoir [12].
Currently, the Boston Scientific/AMS 700 and Coloplast Titan series are market leaders on inflatable prostheses of this type [6].
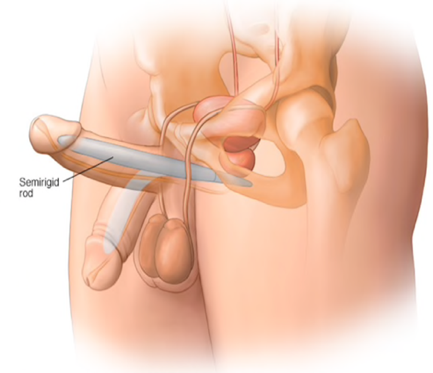
![Figure 3: Three-component inflatable PP. Adapted from bostonscientific.com **Semi-rigid PP:** Semi-rigid PPs consist of two cylinders placed in the corpora cavernosa. These devices have a central core that allows the penis to be curved downwards for concealment and upwards for sexual activity. They are a more economical option, have a high mechanical reliability and are more simple to use and to surgically implant, but they present a greater risk of erosion, don’t allow expansion of circumference and length and the rigidity is constant, which makes it difficult to hide the device, since the penis maintains the same volumetry (Figure 4) [2,13].](/fulltextimages/9228/fig_3.png)
Figure 3: Three-component inflatable PP. Adapted from bostonscientific.com Semi-rigid PP: Semi-rigid PPs consist of two cylinders placed in the corpora cavernosa. These devices have a central core that allows the penis to be curved downwards for concealment and upwards for sexual activity. They are a more economical option, have a high mechanical reliability and are more simple to use and to surgically implant, but they present a greater risk of erosion, don’t allow expansion of circumference and length and the rigidity is constant, which makes it difficult to hide the device, since the penis maintains the same volumetry (Figure 4) [2, 13].
These prostheses are a suitable option for patients with low manual dexterity and who are willing to accept the less aesthetic component of the prosthesis. However, these devices are not ideal for patients who need to perform cystoscopies repeatedly, because the cylinders make the procedure technically difficult [13].
Boston Scientific has the Spectra (ex-Dura II), AMS 600 and AMS 650 prostheses; Coloplast offers the Genesis model, Dacomed offers the Jonas and OmniPhase / DuraPhase models and Zephyr offers the ZSI 475FtM and ZSI 100FtM models [6].
Main Companies
Boston Scientific/AMS: The first version of the inflatable PP created by AMS was characterized for having durability and stiffness rates below what was considered satisfactory, with complication rates of 61% and revision rates between 3 to 11 years after placement [5].
Between 1983-1987 several upgrades were made, compared to the initial model AMS 700, which included the redesign of the cylinders and their ends, with the objective of increasing the resistance and the development of a fluid containment system without requiring suture, which did improve the leak prevention rate. In 1986, there was a great advance with the addition of the so-called kinking- resistant tubing (KRT), allowing less rigorous intraoperative measurements and simplifying the entire procedure of surgical insertion of the prosthesis; a coating made of polytetrafluoroethylene (PTFE) was also added to increase the durability and useful life of the device. In 1987, the PTFE coating was replaced by a three-layer system in the new model, the AMS 700 CX®, which consisted of an internal layer of silicone, a medium layer of Dacron and Lycra and an external layer of silicone, which allowed, not only reduce friction, but also facilitate inflation, thus reducing the resistance to filling which led to mechanical failures and aneurysmatic dilations. All of these changes in the device drastically improved the longevity of the prosthesis, as well as reduced the rates of complications (from 61%, before 1983 to 13% after 1983). The above-mentioned model was again evaluated in 2000, when Carson, et al. Found that in 372 patients, the mechanical reliability of the device was 86.2% after 5 years, with an infection rate of 3.2% of patients. In 2001, AMS debuted a new coating consisting of parylene which, by increasing the lubrication of the silicone, reduced friction even further, better mimicking an organic erection and also reducing the risk of aneurysmal dilation (Figure 5) [5, 7, 13].
![Figure 5: PP Boston Scientific/AMS 700 [12].](/fulltextimages/9228/fig_5.png)
The AMS 700 series manufactured by Boston Scientific currently has three variants (700 CX, CXR and LGX) which, depending on the model, allow controlled expansion in longitudinal and/or transverse dimensions, adapting thus, to several situations that, in the past, were seen as difficult to solve, such as, for example, men with minor erections or anatomical abnormalities, such as fibrosis in the corpora cavernosa [5, 7].
The AMS 700 CX (controlled expansion) model offers only a controlled circumferential expansion, through its unidirectional dacron-lycra material [13].
The AMS 700 CXR (controlled expansion restricted) model, which was an evolution of the AMS 700 CXM (controlled expansion modified), is a similar model, but with smaller components, which also provides a controlled circumference expansion indicated for when there is a large limitation on the insertion of the prosthesis cylinders in the corpora cavernosa, such as, for example, in patients with fibrosis in the corpora cavernosa [6, 13].
The AMS 700 LGX (length girth expansion) model offers controlled expansion in length and circumference, when filled with fluid, through its bidirectional layers of dacron- lycra. This is the only model that allows a 1-4 cm penis enlargement compared to other devices [13].
The AMS 700 series was also subject to improvements at the pump level, with the introduction of the Momentary Squeeze (MS) pump in 2006, with the aim of facilitating deflation, just requiring a simple and quick press of 3-4 seconds of the button, instead of the patient having to press the button during the entire deflation; for inflation, the Tactile pump was introduced, which allowed the transfer of a greater amount of fluid to the cylinders [6].
In the 80’s and 90’s AMS introduced the AMS Hydroflex model in an attempt to reduce the number of components deployed, while maintaining the benefits of an inflatable PP. The AMS Hydroflex prosthesis consisted of two cylinders with a reservoir incorporated at the proximal end and the inflating/deflating pumps at the distal end, which allowed the transfer of the fluid to a non-distensible central core. However, despite its popularity at the time of launch, the AMS Hydroflex was soon substituted by the AMS Dynaflex, a device similar to the previous one, but with multiple tubes that connected the pump to the reservoir, providing better rigidity [6].
In 1994, AMS launched the Ambicor inflatable PP, a two- component device that included two cylinders, implanted in the corpora cavernosa, and a pump placed in the scrotum. Therefore, the procedure for placing these devices was simpler, compared to the three-component inflatable PP, because there was no placement of any reservoir, since the design of the cylinder itself included an inflatable portion and a proximal portion that served as a reservoir for the fluid; patients were able to achieve an erection by compressing the scrotal pump several times, transferring the solution from the reservoir areas located in the proximal part of the cylinders to the inflatable part of the cylinder. Despite this advantage, the level of inflation and stiffness achieved was not as desired, due to the small amount of fluid contained in these devices. This prosthesis, which is still on the market today, is more used for cases in which one wants to avoid approaches through the retropubic space, for example, due to previous surgeries, or when the implantation of the reservoir is technically difficult [7, 9, 13].
The older AMS models (650 and 600) were semi-rigid PPs and had a stainless steel core coated with silicone that allowed the user to flex the penis upwards (for coitus) or downwards (for concealment), depending on the situation [13].
AMS Spectra is currently a reference semi-rigid PP, consisting on two cylinders, externally coated with silicone, which have a foldable portion formed by alternating segments of titanium and polyethylene. This segment is regulated by a central cable mechanism, which, allows, on one hand, adequate rigidity for sexual intercourse, when it is at maximum extension (maximum 90º), but on the other, a concealment mechanism when not in use, due to the flexion angle (maximum 7º) that the prosthesis can reach, thanks to its foldable portion (Figure 6) [6, 14].

In 2000, AMS started offering devices covered by antibiotics, intitulated InhibiZoneTM, which consisted of a formulation composed of minocycline and rifampicin, which was impregnated on the external surface of the PP, with the aim of reducing infections. In 2004, Carson, et al. Made a comparison of the infection rate between the coated and uncoated prostheses of InhibiZone TM, to conclude that, after 60 days, there was an 82.4% reduction in the infection rate in the inflated PP coated with InhibiZone TM and a reduction, after 180 days, of 57.8%. Thus, the introduction of the InhibiZone TM coating significantly reduced infection rates when compared to prostheses that were not coated with InhibiZone TM [5, 7].
In 2010, AMS introduced the concealment reservoir, which had a flat “pancake” configuration, compared to the classic sphere-shaped reservoir, when filled with saline solution, providing better concealment [6].
Coloplast/Mentor: The main difference that the company Mentor, now Coloplast, made in its models of inflatable PPs of three components was the use of different materials in the cylinders, in relation to the models of AMS. Instead of using silicone, the cylinders of the devices were initially made of polyurethane, later designated as Bioflex® material. This new material had numerous advantages over silicone cylinders, the most important of which was perhaps greater tensile strength than AMS cylinders. Bioflex® also provided a more limited expansion capacity, unlike silicone models, which were prone to excessive swelling. Therefore, after the introduction of Bioflex®, Mentor added to the inflatable models a Bioflex® reservoir made up of a new material, KRT silicone, which would later be improved with the addition of nylon. Thus, the Bioflex® models demonstrated a durability superior to that existing in the market, with 88% of the operational devices, after 10 years of use [5].
In 1986, Mentor introduced a three-piece inflatable PP, the Alpha-1, which had undergone improvements in order to increase the durability of the device and reduce the risk of liquid leakage through the connection tubes. As a result, Alpha-1 had higher 5 years longevity rates and lower failure rates, compared to models manufactured before November 1992 (92.6% vs. 75.3% and 1.3% vs. 5.6%, respectively) [5].
In 1988, Mentor launched the Mentor GFS prosthesis (girth, flaccidity, simplicity), a two-piece device, which consisted of a pair of cylinders and a reservoir and pump that were merged into a single piece, the “resipump”, placed in the scrotum. Thus, the cylinders were connected, through tubes, to the reservoir and the pump, causing them to expand to a fixed circumference. However, due to the high complication rates, related to infections and mechanical failures, the model was subject to improvements, replaced and renamed to Mark II, because the tubes that made the connection between the resipump and the cylinders were eliminated. The most recent two-component PP produced by Coloplast (ex-Mentor) was the Excel model, which contains a hydrophilic coating based on an antibiotic [5, 7].
In 2000, Mentor introduced a blocking valve in the reservoir, designed to reduce the likelihood of self-inflation of inflatable PPs, preventing the fluid under pressure in the reservoir, resulting from increased intra-abdominal pressure, from reaching the cylinders. In 2002 Wilson, et al. Compared devices with and without blocking valves and concluded that, although there was no significant increase in the estimated 1-year survival rates, patient satisfaction, infection and mechanical failures, only 2 patients (1.3%) with devices equipped with blocking valves reported self- inflation compared to 11% of patients without this valve. In 2004, Coloplast introduced its semi-rigid device, called Genesis®, a PP that does not have any moving internal components in order to don’t compromise reliability and that has the particularity of being composed of a hydrophilic coating, allowing selecting the antibiotic most suitable for each patient. The PP, to achieve this malleable mechanism, has, at the distal end, a silver core surrounded by a helical wire (Figure 7) [6, 15, 16].
The three-component inflatable PPs manufactured by Coloplast are Titan and Titan Narrow. In these models, the cylinders and the reservoir are covered by Bioflex®, the main highlight of these devices, while the connection tubes and the pump are made of silicone. Similar to other models of the brand, the components are coated with a hydrophilic substance, with antimicrobial function and also have a blocking valve in the reservoir that helps to prevent spontaneous self-inflation. In the same study mentioned above, in 2004, by Wolter, et al. It was observed that, in 2357 users of Titan devices, the 1-year infection rate was 1.06%, compared with 2.07%, observed in 482 patients implanted with Alpha-1 PPs. In both groups, the main infectious agent was the bacterial species Staphylococcus. In 2011 Dhabuwala, et al. Analyzed Titan prostheses coated with vancomycin/ gentamicin or rifampicin/gentamicin and AMS prostheses with InhibizoneTM coating to compare infection rates. The Titan prosthesis with vancomycin/gentamicin had an infection rate of 4.4% and the InhibizoneTM prosthesis had an infection rate of 1.3%. Titan inflatable PPs with rifampicin/ gentamicin had no reported infections. The researchers concluded that rifampicin was the best antibiotic to use [5, 6, 13].
In 2008, Coloplast introduced a new pump mechanism, the One Touch Release (OTR), which allowed the complete deflation of the prosthesis with just one squeeze, causing the fluid to move, only and exclusively, from the cylinders for the reservoir (Figure 7) [17].
![Figure 7: Coloplast/Mentor Titan with OTR pump [17].](/fulltextimages/9228/fig_7.png)
Similar to the AMS 700 CXR, Titan Narrow is ideal for patients with fibrotic bodies in the corpora cavernosa [13].
Surgitek: In the 80’s, Surgitek launched a one component inflatable prosthesis, the Flexi-Flate model, which was composed of two hydraulic cylinders, each containing two chambers, an outer chamber of the reservoir, where the fluid was in the flaccid state and an internal chamber, when the objective was erection [6, 11].
In the late 80’s, the american company introduced a two-component prosthesis called Uniflate 1000 to the market. Its cylinders had two layers, a silicone outer and a dacron inner, with the objective of designing two chambers in each cylinder, for the external chambers to add a greater circumference to the cylinder. Thus, the fluid in the resipump entered the inner chamber and was transferred to the outer chamber when a valve was tightened at the distal end of the cylinder. Despite this, this prosthesis never received approval to enter the market due to mechanical failures related to the fluid transfer mechanism. [11].
In 1997, the Flexi-Rod prosthesis was introduced, a semi-rigid PP that consisted of two silicone cylinders with a firm distal part, the softest middle part to create a hinge effect in the peno-scrotal area, in order to hide it better, and the proximal section composed of segments that could be adjusted, in terms of dimension, according each patient. Subsequently, the silicone core was reinforced with dacron to increase rigidity and a more flexible hinge was created in the middle section, having been renamed to Flexi-Rod II. It was also gradually disappearing from the market [6, 11].
Dacomed: The Jonas prosthesis was the first semi-rigid prosthesis introduced in the American market by the company Dacomed. In 1980, Jonas and Jacobi developed the first German semi-rigid device, the ESKA-Jonas prosthesis, which consisted of a prosthesis made of silicone into which interwoven silver threads were embedded to increase stiffness and allow voluntary flexion of the penis. This German prosthesis received an additional improvement with the teflon coating on the core in order to increase the mechanical durability, since the silver threads were prone to breakage when flexing the PP [6, 11].
The introduction of the semi-rigid prosthesis OmniPhase, in 1986, aimed to provide a prosthesis that was only inserted in the corpora cavernosa, that avoided the use of hydraulic and fluid components and that managed, nevertheless, to alternate between the flaccid and rigid states . The prosthesis used a central cable surrounded by a series of spherical polysulfone segments, in order to achieve a mechanism that changed the length of the central cable, resulting in a flacid or erect state, depending on the tension of the cable. However, this prosthesis was associated with a constant break of the central cable, which caused this prosthesis to be revised and an improved model appeared, the DuraPhase prosthesis, which, despite the weakness of the central cable mechanism has been improved, continued to present an unacceptable rate of problems associated with the central cable. To solve this problem, once again, the cable configuration was reformulated, reducing the size and increasing the number of cables, finally resulting in increased mechanical reliability, having been renamed to Dura II. This PP is currently marketed by AMS as an AMS Spectra prosthesis [6, 11].
Zephyr Surgical Implants: Phalloplasty, that is, the increase in penile size, is a surgery that has undergone, in recent years, major upgrades in order to be able to respond to the main objectives of the people who seek it, most of them, individuals who suffer of gender dysphoria: aesthetic component of the genitals and penile rigidity for sexual intercourse. In this respect, the implantation of a PP after the performance of phalloplasty plays a fundamental role in the component of erection and stiffness. However, its implantation is referred to as a challenge, not only because there is no solid tissue (cavernous tissue) where PP can be anchored, but also because the neophalus is less vascularized, less resistant and does not protect/cover the part distal of PP [18].
Thus, in 2012, the Swiss company started marketing its inflatable prosthesis of three components, the ZSI 475FtM, achieving some European success, namely because it is specific for transgender surgery. The model in question has several particularities that make it very oriented to respond to this type of surgery: a wide base for fixation to the pubic bone, a glans with realistic shape and consistency and a pump with the shape of the testicle in order to be the more aesthetically close to reality. As a relatively recent model, in 2019 Neuville, et al. Published a study with the objective of evaluating the safety, reliability and satisfaction of patients in this PP. For this, they selected 20 patients, with an average age of 37.9 years, who implanted the model in question. All individuals suffered from gender dysphoria and underwent transgender “female-to-male” (or FtM) surgery. An average follow-up time of 8.9 months was performed. To assess patient satisfaction were used various scores: IIEF-5, EDITS and Self Esteem and Relationship (SEAR). Of the 20 initial patients, 14 (70.0%) responded to the questionnaires. The investigators then reported that 12 patients (85.7%) had regular sex during the follow-up period. The mean scores of IIEF-5 were 20.2 out of 25, SEAR was 84.5 out of 100 and EDITS was 82.0 out of 100. Finally, 13 patients (92.8%) reported being, overall, satisfied or very satisfied with the prosthesis. It should be also noted complications rates related to infections, mechanical failures and surgical failures were, respectively, 4.7%, 9.5% and 4.7%. The results allowed the authors to conclude that, when compared with other PPs from other studies, the rate of complications (infections, mechanical failures and surgical complications) was lower and scores referred were higher. Thus, safety and patient satisfaction seem to be assured, making this prosthesis an option to consider in this type of surgery [6, 18].
Also, in terms of transgender surgery, the same company also developed a model of semi-rigid prosthesis, the ZSI 100 FtM. Then, in 2019 Pigot, et al. Released the results of their retrospective study that involved the semi-rigid PP model. The researchers’ main objective was to describe their clinical experience with the model in question. For this, they included a total of 25 individuals with an average age of 36 years, with an average follow-up time of 6.3 months. Researchers then reported that, due to complications, prosthesis implantation was performed in 8 patients (32%) due to infection (n=3), protrusion (n=4), pain in the pubic area (n=1) or due to personal non-adaptation with it (n=3). Of those with the implanted prosthesis, and who used it regularly, 13 of the 14 patients (93%) were able to have sex. Researchers highlighted some advantages of this model, namely that it is a PP that is easy to implant, without resorting to major surgery; is a PP that can be customized in terms of size, it’s easy to use and effective for what is designed. However, there are similarities with other semi-rigid PPs, it is not possible to acquire a state of complete flaccidity and patients may complain of pain in the pubic region (as it is in this region where it is fixed). In conclusion, the results regarding the complication rates are very much in line with those of other studies and, therefore, this model may be an option for certain people within the transgender group [6, 19].
Giant Medical: In the 1990s, the Italian company, Giant Medical, launched the semi-rigid prosthesis Virilis ITM which is composed by a soft silicone, while Virilis IITM holds a firmer distal portion. Because both prostheses are made of silicone, there’s no need for destruction of the cavernous tissue allowing for a more natural erection due to the preservation of the underlying cavernous blood flow [6].
Another semi-rigid prosthesis designed by this company was the ApolloTM model with the objective of, through periodic injections with saline solution, to produce an expansion of the tissue, before the implantation of a definitive prosthesis [8].
Discussion
Surprisingly, in an era where non-invasive treatment is increasingly prevalent, PPs, and generally medical devices, currently used for the treatment of ED, would go out of use and be removed from the list of therapeutic options. However, despite the fact that, currently, they are not first-rate, as in the past, PPs, appear as an important line of treatment for this disease, highly prevalent in the male population and highly conditioning in terms of the quality of life of the couple. Currently, PPs are mostly used in cases where the first line treatment, iPDE-5, fails or is contraindicated. The main reasons that lead to their choice are the high efficiency and satisfaction that couples report when using it, as well as the high safety and low complication rates of both devices. Therefore, PPs not only did not fall out of favor, but were undergoing updates and improvements in several aspects, such as the naturalness of the erection or the aesthetic aspect. However, these devices have not only advantages and their disadvantages, mainly verified in semi-rigid PPs, are always around the artificiality of the erection, the lack of rigidity or the learning difficulty to handle these devices, in order to obtain the expected results. In cases where it is possible, in a certain way, to circumvent these problems, as is the case of three-component PP, the problem of reliability related to the greater complexity of implantation and functioning of the prosthesis arises.
In an unexpected way, taking into account that we are faced with an extremely frequent pathology and that it’s increasing in terms of incidence in the male population, the scientific community still searching for the ideal medical device, that is, one that simulates with the maximum perfection penile erection and flaccidity and doesn’t interfere with other systems.
It was only in the past year that studies about prostheses designed specifically for transgender surgery were published, as was the case with the ZSI 475FtM and ZSI 100FtM prostheses. However, these are only the first studies and need further investigation to better assess the clinical experience, namely effectiveness, satisfaction and complications, of these specific models for a type of population that is increasingly growing.
Another suggestion is related to the fact that banal technologies, such as Bluetooth, for example in PPs are incorporated, with the aim of transmitting the data and sharing it with your doctors and, thus, simplifying the whole process for doctor and patient, similarly to what’s already done with pacemakers in the field of cardiology.
In short, despite the move towards less and less invasive medicine, currently, PPs still occupy a very relevant place in the treatment of ED.
Conclusion
The PP market is vast and diversified, having adapted and improved over time, following the evolution of technology. Currently, they’re used as a 3rd line of treatment, but they are an equally effective and permanent solution, yet irreversible. These devices are also associated with a very high level of couple’s satisfaction. However, like all existing treatments, it isn’t immune from complications mainly associated with infections and erosions.
Semi-rigid PPs are those that have a simpler operating mechanism and, therefore, are, in theory, those that have less surgical complications and greater mechanical reliability.
However, they fail in terms of induce a flaccid penis.
One and two-component PPs, by reducing the number of parts in the device, try to simplify the entire surgical procedure and reduce the number of PP-related complications as much as possible. However, in general, these prostheses have a limitation in terms of cylinder inflation, making it impossible to achieve the desired stiffness for intercourse in many cases.
Thus, three-component PPs currently dominate the vast majority of the prosthesis market, with varied options that try to adapt to the limitations of different people. In this field, the two major models are Boston Scientific/AMS 700 and Coloplast Titan, each with its own specific variations.
After all, the objective of all types of medical devices is common, that is, to obtain an erection as close as possible to functional and aesthetic levels, without interfering with the other systems of the human body, in order to allow the couple to improve their quality of life.
References
-
Sepúlveda L, Meireles A, Moreira P, Dinis H, Marques V, et al. (2016) Próteses penianas no tratamento da disfunção erétil: a casuística de 13 anos. Acta Urológica Port 33(3): 75-80.
-
Rew KT, Heidelbaugh JJ (2018) Erectile Dysfunction 94.
-
Lee M, Sharifi R (2018) Non-invasive Management Options for Erectile Dysfunction When a Phosphodiesterase Type 5 Inhibitor Fails. Drugs Aging 35(3): 175-187.
-
Rodriguez KM, Kohn TP, Davis AB, Hakky TS (2017) Penile implants: a look into the future. Transl Androl Urol 6(5): S860-S866.
-
Rodriguez KM, Pastuszak AW (2018) A history of penile implants. Transl Androl Urol 6(Suppl 5): S851-S857.
-
Chung E (2017) Penile prosthesis implant: scientific advances and technological innovations over the last four decades. Transl Androl Urol 6(1): 37-45.
-
Le B, Burnett AL (2015) Evolution of penile prosthetic devices. Korean Journal of Urology 56(3): 179-86.
-
Bettocchi C, Palumbo F, Spilotros M, Palazzo S, Saracino GA, et al. (2010) Penile prostheses. Ther Adv Urol 2(1): 35-40.
-
Carson CC (2005) Penile Prosthesis Implantation: Surgical Implants in the Era of Oral Medication. Urol Clin North Am 32(4): 503-509.
-
Carson CC (2018) Penile Prosthesis for Erectile Dysfunction. Encycl Reprod 4: 423-426.
-
Mulcahy JJ (2016) The Development of Modern Penile Implants. Sex Med Rev 4(2): 177-189.
-
Gurtner K, Saltzman A, Hebert K, Laborde E (2017) Erectile Dysfunction: A Review of Historical Treatments with a Focus on the Development of the Inflatable Penile Prosthesis. Am J Mens Health 11(3): 479-486.
-
Sadeghi-Nejad H, Fam M (2013) Penile prosthesis surgery in the management of erectile dysfunction. Arab J Urol 11(3): 245-253.
-
Akdemir F, Okulu E, Kayıgil Ö (2017) Long-term outcomes of AMS Spectra® penile prosthesis implantation and satisfaction rates. Int J Impot Res 29(5): 184-188.
-
Casabé AR, Sarotto N, Gutierrez C, Bechara AJ (2016) Satisfaction assessment with malleable prosthetic implant of Spectra (AMS) and Genesis (Coloplast) models. Int J Impot Res 28(6): 228-223.
-
Sadeghi-Nejad H (2007) Penile Prosthesis Surgery: A Review of Prosthetic Devices and Associated Complications. J Sex Med 4(2): 296-309.
-
Ohl DA, Brock G, Ralph D, Bogache W, Jones L, et al. (2012) Prospective Evaluation of Patient Satisfaction, and Surgeon and Patient Trainer Assessment of the Coloplast Titan One Touch Release Three-Piece Inflatable Penile Prosthesis. J Sex Med 9(9): 2467-2474.
-
Neuville P, Morel-Journel N, Cabelguenne D, Ruffion A, Paparel P, et al. (2019) First Outcomes of the ZSI 475 FtM, a Specific Prosthesis Designed for Phalloplasty. J Sex Med 16(2): 316-322.
-
Pigot GLS, Sigurjónsson H, Ronkes B, Al-Tamimi M, van der Sluis WB (2020) Surgical Experience and Outcomes of Implantation of the ZSI 100 FtM Malleable Penile Implant in Transgender Men After Phalloplasty. J Sex Med 17(1): 152-158.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report