Employer Health Plan Exclusions are a Barrier to Access of Penile Implants for Erectile Dysfunction
Introduction: Many commercial insurers and Medicare have published coverage policies detailing the medical necessity and accessibility of erectile dysfunction (ED) treatment, including implantable penile prosthesis (IPP). Approximately 61% of adults aged 18–64 years in the United States (US) receive health benefits via employer-sponsored health plans (ESHP) and 23% of employers reported medical benefit exclusion for sexual dysfunction treatment. Objective: To obtain nationwide US estimates of the proportions of patients denied IPP treatment due to ESHP exclusions (overall and by state, healthcare insurer, and labor sector industry). Methods: De-identified data from an industry IPP insurance benefit verification database from October 1, 2018 to December 31, 2021 were analyzed to evaluate ESHP-related barriers to IPP access. Results: Among 2,638 patients with commercial insurance and employer data, 34.0% were denied IPP treatment due to ESHP benefit exclusions. ESHPs in Washington (60.7%), Louisiana (55.4%), Arizona (46.6%), Nebraska (45.5%), Ohio (43.3%), and Georgia (43.1%) had the highest exclusion rates, whereas Iowa (19.0%), Alabama (18.9%), Maryland (17.3%), Rhode Island (13.0%), and New York (7.1%) had the lowest exclusion rates. Patients with Aetna insurance had the greatest proportion of exclusions (62.4%), followed by Cigna (61.0%), employer-owned health plans (47.2%), other commercial plans (41.8%), Anthem (37.3%), Blue Cross Blue Shield (BCBS) state plans (24.1%), United Healthcare (15.4%), and Humana (0.0%). The exclusion rate was highest for employees of the leisure and hospitality industry (51.9%), followed by religious organizations (50.0%), health care (40.5%), construction, mining, or agriculture (39.1%), education (38.9%), retail and wholesale trade (36.9%), manufacturing (36.7%), utilities (36.2%), professional and business services (35.4%), transportation (32.6%), finance and insurance (29.1%), labor union organizations (26.9%), and finally public, state, and government administration (25.1%). Conclusions: Despite insurance carrier medical policies, 34.0% of men with an ESHP are denied access to IPP ED treatment due to their ESHP benefit exclusions. ESHP exclusion rates varied geographically, by insurer, and by labor sector industry.
Introduction
Erectile dysfunction (ED) is a common and burdensome urologic condition with profound consequences [1, 2, 3]. Most men with ED have at least one major cardiovascular or endocrine disease risk factor such as hypertension, hypercholesterolemia, or diabetes [4]. Many men with ED are prostate cancer survivors as more than 70% of men undergoing radical prostatectomy report some degree of ED one year following surgery [5]. ED poses a considerable psychological burden on men as it interferes with their overall quality of life (QoL), including their well-being, self- esteem, relationships, and self-worth [6]. Additionally, men with ED have significantly higher rates of absenteeism, presenteeism, overall work productivity impairment, and activity impairment compared to men without ED [6].
Treatment for ED is widely considered ‘medically necessary’ by healthcare insurers. In the United States (US), many commercial insurers and Medicare have published coverage policies providing criteria for medically necessary treatment of ED. The health plan coverage policies include many of the same treatment options as professional society guidelines for the treatment of ED [7, 8, 9], ranging from oral medications, external devices, surgically implanted devices, etc. The most commonly used first-line treatments for ED are oral phosphodiesterase-5 (PDE5) inhibitors; however; approximately one-third of patients do not respond to PDE5 inhibitors and some patients are not able to take them due to medical conditions [10]. One-third of patients using PDE5 inhibitors cease use after one prescription and one-half cease use by six months [11]. Implantable penile prostheses (IPPs) are an alternate, definitive treatment for patients with ED [12]. American Urological Association (AUA) guidelines state that “using the shared decision-making process as a cornerstone for care, all patients should be informed of all treatment modalities that are not contraindicated, regardless of invasiveness or irreversibility, as potential first-line treatments” [9].
Despite health insurance medical benefit coverage, published medical coverage policies, and professional society guidelines [7, 8, 9], there are a disparity in medical and reimbursement coverage for ED treatment in the US [13]. A report published in 2011 by the US Government Accountability Office showed that, in employer-sponsored health benefit plans (ESHPs) from 2010 or 2011, 23% of employers reported a medical benefit exclusion for sexual dysfunction treatment [14]. Another study evaluating trends in health plan insurance coverage of inflatable penile prostheses (IPPs) among patients at the University of Miami between 2016-2017 found that a significant proportion of men with commercial health plan coverage seeking IPPs were unable to obtain the device due to exclusion in their ESHP benefit [15]. The objective of the current study was to expand upon this research by analyzing an IPP manufacturer health plan medical benefit verification database to obtain nationwide US estimates of the proportions of patients denied treatment due to ESHP exclusions. The exclusion rates were evaluated overall, and they were analyzed by state, healthcare insurer, and labor sector industry to assess whether there were any trends in ESHP IPP exclusions.
Methods
Data Source and Patient Population
From October 1, 2018 to December 31, 2021, de- identified data from an industry insurance benefit verification database were analyzed to evaluate ESHPs-related barriers to access for IPP ED treatment. In order to be included in the analysis, each verification record was required to have information regarding the health insurance type, the health plan’s name, the presence of information regarding coverage for IPP, and ESHP data regarding benefit exclusion. Cases with commercial insurance coverage and data regarding the patient’s employer were the focus of the analyses in order to evaluate ESHP exclusions.
Outcomes Evaluated
Data extracted from the insurance benefit verification database included the closed date of the benefit verification, the type of insurance (i.e., government, commercial, military, Worker’s Compensation or ‘other’), the coverage status (i.e., access available – verified/approved, no access due to non- covered service, or no access due to ESHP exclusion), the state, the insurance carrier, and the employer.
Data Analyses
Descriptive statistics were performed to describe all variables in the dataset for patients who received IPP benefit verification. Means, medians, and standard deviations were presented for all continuous outcome variables and counts or proportions were presented for categorical variables. Data management and statistical analyses were conducted using Microsoft® Excel® (Redmond, WA, USA). The proportions of patients with ESHP benefit exclusion were presented overall, geographically (by US state), by healthcare insurer, and by labor industry sector. Data regarding the patients’ employers was categorized into labor industry sector using US Bureau of Labor Statistics labor sector categories.
Results
Among the 8,623 IPP benefit verification cases from October 2018 to December 2021, 76.6% had commercial insurance, 19.0% had Medicare, 3.0% had Medicaid, 1.4% had military insurance, and 0.1% had Worker’s Compensation. An overall analysis of IPP coverage showed that, across the four years, 78.6% of patients with commercial insurance, 100% with Medicare, 54.9% with Medicaid, 100% with military insurance, and 100% with Worker’s Compensation had access to IPP treatment (Figure 1). The proportion of patients with commercial insurance with access to IPP declined slightly from 2018 and 2019 (79.9% and
81.1%, respectively) to 2020 and 2021 (78.2% and 76.8%, respectively). The proportion of patients with Medicaid with IPP coverage increased from 2018 and 2019 (47.4% and 38.2%, respectively) to 2020 and 2021 (58.9% and 65.3%, respectively). The proportion of patients with Medicare, military insurance, and Worker’s compensation with IPP coverage remained at 100% over the four years (Figure 1).
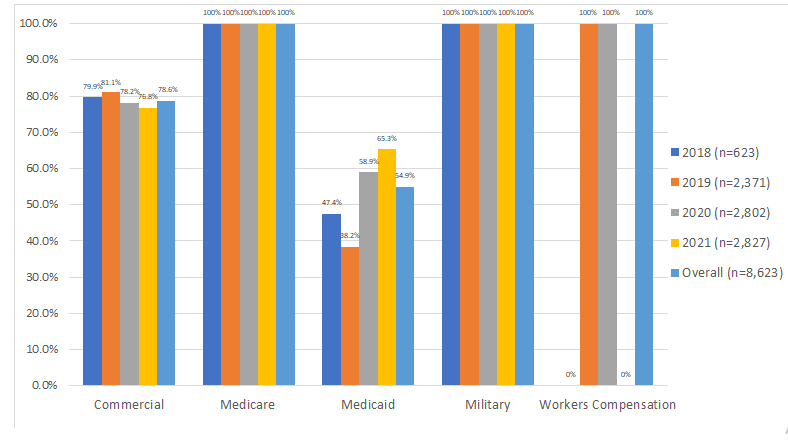
Figure 1: Proportions of patients with access to IPPs by year and by payer. BCBS, Blue Cross Blue Shield; IPP, inflatable penile prosthesis. Of 6,598 cases with commercial insurance, 2,638 had data on the patients’ employers. Overall coverage among patients with employer data was lower compared to all patients with commercial insurance (66.0% vs. 78.6%).
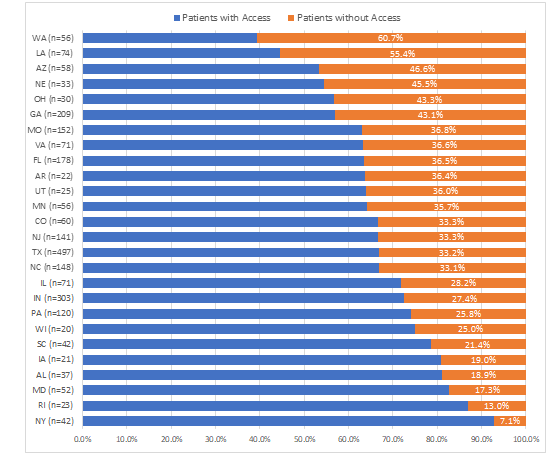
Figure 2: Proportions of patients denied access to IPPs by state. AL, Alabama; AR, Arkansas; AZ, Arizona; CO, Colorado; ESHP, employer-sponsored health plan; FL, Florida; GA, Georgia; IA, Iowa; IL, Illinois; IN, Indiana; IPP, inflatable penile prosthesis; Louisiana; MD, Maryland; MN, Minnesota; MO, Missouri; NC, North Carolina; NE, Nebraska; NJ, New Jersey; NY, New York; OH, Ohio; PA, Pennsylvania; RI, Rhode Island; SC, South Carolina; TX, Texas; UT, Utah; VA, Virginia; WA, Washington; WI, Wisconsin.
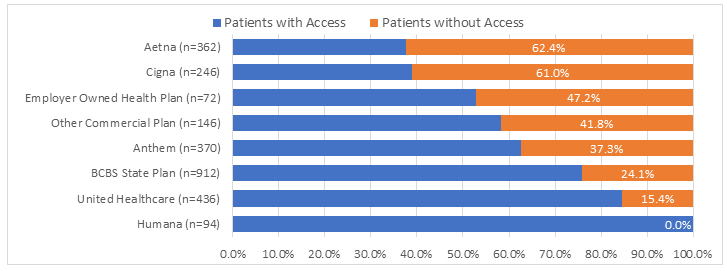
Among commercial cases with employer data, patients with Aetna insurance had the greatest proportion of exclusions (62.4%), followed by Cigna (61.0%), employer- owned health plans (47.2%), other commercial plans (41.8%), Anthem (37.3%), Blue Cross Blue Shield (BCBS) state plans (24.1%), United Healthcare (15.4%), and Humana (0.0%) (Figure 3).
Among the 2,638 cases with employer data, 26 states had data for 20 or more patients seeking IPP coverage. Geographically, ESHPs in Washington (60.7%), Louisiana (55.4%), Arizona (46.6%), Nebraska (45.5%), Ohio (43.3%), and Georgia (43.1%) had the highest exclusion rates, whereas Iowa (19.0%), Alabama (18.9%), Maryland (17.3%), Rhode Island (13.0%), and New York (7.1%) had the lowest exclusion rates (Figure 2).
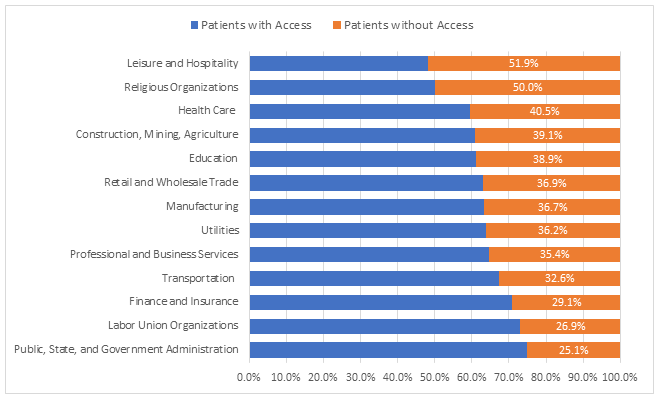
Employees of leisure and hospitality had the highest exclusion rate (51.9%), followed by religious organizations (50.0%), health care (40.5%), construction, mining, or agriculture (39.1%), education (38.9%), retail and wholesale trade (36.9%), manufacturing (36.7%), utilities (36.2%), professional and business services (35.4%), transportation (32.6%), finance and insurance (29.1%), labor union organizations (26.9%), and finally public, state, and government administration (25.1%) (Figure 4).
Discussion
Approximately two-thirds of Americans (67.5%) have commercial or private health insurance coverage, of which 55.7% are insured under an employer-based health plan, accounting for 320,775,014 lives [16]. Despite health insurance medical plan coverage, published medical coverage policies, and professional society guidelines, many ESHPs actually do not include medical coverage benefits for ED treatment. Employers often have specific medical benefit exclusion language written within the employer’s summary of plan benefits for ED treatment options [13].
This study found that 34.0% of patients with ESHPs were denied IPP treatment due to ESHP benefit exclusions. ESHP exclusion rates varied geographically, and were highest for Washington, Louisiana, Arizona, Nebraska, and Ohio. Exclusion rates were highest among patients with Aetna insurance, followed by Cigna, employer-owned health plans, other commercial plans, and Anthem. The labor industries with the highest exclusion rates were leisure and hospitality, religious organizations, healthcare, construction, mining, or agriculture, and education.
There are notable implications of excluded ED treatments by ESHPs. ESHP exclusions create confusion and frustration for clinicians and patients because they usurp the clinicians’ determination of medical necessity and the medical policies developed and published by the health insurance companies that administer their benefits.13 A recent study showed that only 23% of employed men who have been diagnosed with ED actually receive treatment paid for by their ESHP [17]. Although patients may be able to pay for lower cost generic pharmacological ED therapies out-of-pocket, advanced ED treatments such as intracavernosal injections, intraurethral suppositories, vacuum erection devices, and penile prosthesis surgery may not be as accessible to them. Over the past 10 years, ED treatment with PDE5Is remained constant, whereas use of other treatments, including IPP, has declined [17]. Consequently, some patients are more disadvantaged than others based on variations in medical coverage.
In addition to the burden placed on clinicians and patients, these exclusions for ED have implications for the employers. Research on employer benefits and employee engagement showed that 61% of employees reported that health was a bigger concern than wealth or career whereas only 14% of employers cited health and well-being as a talent-management priority [18]. Health and wellness benefits were reported to be more important to employees than job role, colleagues, or organizational culture when it came to loyalty, recruitment, and retention.18 Evidence has also demonstrated that a healthy and engaged workforce correlates with outstanding company financial performance [19, 20, 21]. Worker’s health, productivity, and retention are increasingly important for employers’ competitive advantage in the marketplace [19, 20, 21], particularly since the emergence of COVID-19. Enabling access to medically necessary health benefits such as ED treatment could benefit employers through increased productivity, decreased absenteeism and presentism rates, loyalty, and retention [6, 19, 20, 21]. Employees with ED have been shown to have an incremental 282.7 hours/year of work impairment compared to employees without ED, resulting in annual incremental costs of $7,270 per employee [22].
Conclusions
ED constitutes a large but often hidden burden on society given its high prevalence and impact on QoL and productivity. Despite insurance carrier medical policies, many US men with ESHPs do not have access to ED treatment due to the employers’ benefit design excluding ED or sexual dysfunction benefits. This study found that 34.0% of patients with ESHPs were denied IPP treatment due to ESHP benefit exclusions. ESHP exclusion rates varied geographically, by insurer, and by labor sector industry. Enabling access to medically necessary health benefits such as ED treatment could benefit employers through increased productivity, decreased absenteeism and presentism rates, loyalty, and retention.
References
-
Goldstein I, Goren A, Li VW, Tang WY, Hassan TA (2019) Epidemiology Update of Erectile Dysfunction in Eight Countries with High Burden. Sex Med Rev 8(1): 48-58.
-
Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB (1994) Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 151(1): 54-61.
-
Kessler A, Sollie S, Challacombe B, Briggs K, Van Hemelrijck M (2019) The global prevalence of erectile dysfunction: a review. BJU Int.
-
Hackett G (2009) The burden and extent of comorbid conditions in patients with erectile dysfunction. Int J Clin Pract 63(8): 1205-1213.
-
Haglind E, Carlsson S, Stranne J, Wallerstedt A, Wilderäng U, et al. (2015) Urinary Incontinence and Erectile Dysfunction After Robotic Versus Open Radical Prostatectomy: A Prospective, Controlled, Nonrandomised Trial. Eur Urol 68(2): 216-225.
-
Goldstein I, Goren A, Li VW, Maculaitis MC, Tang WY, et al. (2019) The association of erectile dysfunction with productivity and absenteeism in eight countries globally. Int J Clin Pract 73(11): e13384.
-
Burnett AL, Nehra A, Breau RH, Culkin DJ, Faradayet MM, et al. (2018) Erectile Dysfunction: AUA Guideline. J Urol 200(3): 633-641.
-
SMSNA (2020) Surgical and non-surgical treatments of sexual dysfunction should be standard benefits of all medical insurance programs.
-
AUA Guideline (2018) Erectile Dysfunction. American Urological Association.
-
Goldstein I, Lue TF, Padma-Nathan H, Rosen RC, Steers WD, et al. (1998) Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. N Engl J Med 338(20): 1397-1404.
-
Mazzola CR, Deveci S, Teloken P, Mulhall JP (2013) Exploring the association between erectile rigidity and treatment adherence with sildenafil. J Sex Med 10(7): 1861-1866.
-
Levine LA, Becher EF, Bella AJ, Brant WO, Kohleret TS, et al. (2016) Penile Prosthesis Surgery: Current Recommendations From the International Consultation on Sexual Medicine. J Sex Med 13(4): 489-518.
-
Burnett AL, Edwards NC, Barrett TM, Nitschelm KD, Bhattacharyya SK (2020) Addressing Health-Care System Inequities in the Management of Erectile Dysfunction: A Call to Action. Am J Mens Health 14(5): 1557988320965078.
-
GAO (2020) Employers’ Insurance Coverage Maintained or Enhanced Since Parity Act, but Effect of Coverage on Enrollees Varied, US.
-
Masterson JM, Kava B, Ramasamy R (2019) Commercial Insurance Coverage for Inflatable Penile Prosthesis at a Tertiary Care Center. Urol Pract 6(3): 155-158.
-
Barnett JC, Berchick ER (2016) Health Insurance Coverage in the United States. US Census Bureau.
-
Burnett AL, Rojanasarot S, Amorosi SL (2021) An Analysis of a Commercial Database on the Use of Erectile Dysfunction Treatments for Men With Employer- Sponsored Health Insurance. Urology 149: 140-145.
-
Marsh M (2018) Creating Employee Benefits that Drive Engagement.
-
Goetzel RZ, Fabius R, Fabius D, Roemer EC, Thornton N, et al. (2016) The Stock Performance of C. Everett Koop Award Winners Compared With the Standard & Poor’s 500 Index. J Occup Environ Med 58(1): 9-15.
-
Grossmeier J, Fabius R, Flynn JP, St Noeldner SP, Fabius D, et al. (2016) Linking Workplace Health Promotion Best Practices and Organizational Financial Performance: Tracking Market Performance of Companies With Highest Scores on the HERO Scorecard. J Occup Environ Med 58(1): 16-23.
-
Fabius R, Thayer RD, Konicki DL, Yarborough CM, Peterson KW, et al. (2013) The link between workforce health and safety and the health of the bottom line: tracking market performance of companies that nurture a “culture of health”. J Occup Environ Med 55(9): 993- 1000.
-
Rojanasarot SS, Bhattacharyya SK, Burnett AL (2021) Cost of Lost Productivity Due to Erectile Dysfunction and Impact of Employer Benefit Exclusion of Penile Prosthesis Implantation Treatment. J Occup Environ Med 64(5): 403-408.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report