Self Amputation of the Penis to a Schizophrenic Patient: A Case Report
Introduction: We present a rare case of complete self-amputation of the penis to a patient followed for schizophrenia under neuroleptic. Case Presentation: A 44 years old patient, schizophrenic under neuroleptic, who presents following an almost total section of his penis 48 hours after his self-mutilation. After having ruled out a life-threatening emergency, hemostasis control with urethral catheterization was carried out in the operating room and then phallic replacement may be indicated to the patient after psychological stabilization. Discussion: The section of the penis is a rare urological emergency that requires a fast surgical catch and can be classified into 3 groups: self-mutilation, criminal amputation or traumatic accident. Schizophrenia and depression represent the two most common causes of psychosis. Iatrogenic amputations of the penis have been described in the literature secondary to circumcisions. Surgical management is based on emergency reimplantation of the penis, section with placement of a urethral catheter or phallic replacement. Conclusion: The section of the penis is a rare urological emergency and the choice of treatment depends on the severity of the lesions and the consultation time.
Introduction
Section of the penis is rare, more common in men between the ages of 20 and 30, and most patients are psychotic at the time of sectioning of the penis [1]. The severity of the injuries can range from lacerations to total amputation of the penis and the instruments used can be blades, knives or scissors. We report the case of an almost total section of the penis in a schizophrenic patient consulting in a stable hemodynamic state after 48 hours of his self-mutilation and aimed to show that the external genital organs represent one of the sites or targets of self-mutilation in a schizophrenic patient and that penis complete section by self-mutilation is possible.
Observation
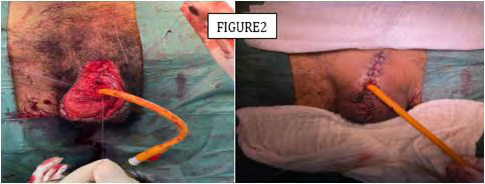
This is a 44-year-old patient, followed for schizophrenia under neuroleptics, admitted for an almost total section of his penis with suicidal thoughts motivating his family to consult our emergency room for additional care after 48 hours of the section. On examination, the patient was conscious, hemodynamically stable, calm and non-cooperative with the interrogation. The examination of the external genitalia organs objectified an almost total section of his penis and without active bleeding through the wound of the section (Figure 1). The patient was brought back urgently to the operating room with satisfactory control of haemostasis of the cavernous bodies and spongious muscle with haemostatic sutures, then dissection and catheterization of the urethra (Figure 2). The postoperative biological assessment based on blood count, haemostasis assessment and renal function did not note any particularity. The patient was then referred to psychiatry service for further treatment. After stabilization on the psychological status and with agreement of the patient, a phallic replacement may be indicated.

Discussion
The section of the penis is a rare urological emergency, and requires a fast surgical catch. It most often occurs in a psychotic state or secondary to drug [1]. The section of the penis can be classified into 3 groups: self-mutilation, criminal amputation or traumatic accident [2]. Genital self- mutilation has been classified into 3 groups according to Blacker and Wong: psychotics, transvestites and men with religious or cultural conflicts. Schizophrenia and depression represent the two most common causes of psychosis. In most cases, the psychosis secondary to schizophrenia was controllable, which allowed these patients to keep their surgical reconstructions [3]. Traumatic penis’ amputations are rare and most often occur after an accident, burn, animals’ attack or sexual abuse. Iatrogenic amputations of the penis have been described in the literature secondary to circumcisions especially the glans’ amputation [4]. Surgical management is based on emergency reimplantation of the penis, which was impossible for our patient given the delay in consultation, section with placement of a urethral catheter or phallic replacement. Reimplantation of the penis is a surgical emergency and requires emergency care and depends on the viability of the amputated penis and the state of the graft bed [2]. In the event of failure of the reimplantation or non-viability of the amputated penis, phalloplasty may be indicated after complete healing and stabilization of the patient’s psychological state. The delay in treatment is mainly linked to the patient’s psychosis. Even if amputations are rarely fatal, it sometimes occur severe bleeding that requires transfusion and emergency care in the intensive care unit [5]. Preservation of the sectioned penis should always be attempted. The penis must be rinsed in a saline solution and placed in a sterile bag then conserved in an ice bath to keep the hypothermia which favors the survival of the tissues [6]. In the literature, cases of reimplantations have been carried out successfully during the first 24 h [7]. The first cases of penis’ reimplantation were done without vascular or nerve anastomosis and the first case was described in 1929 [8]. The main complications of penile reimplantation described in the literature are: necrosis of the skin, loss of sensitivity, stenosis and urethral fistula with no impact on sexual function [9]. The technique of verge’s reimplantation consists in preparing the amputated distal segment and the stump of the penis, a dissection and spatulation of the urethra and identification of the arterial, venous and nervous structures but also the buck’s facia, then an anastomosis of the urethra in two mucosal planes and at the level of the corpus spongiosum and vascular anastomosis using microsurgical techniques [10]. Phallic replacement is reserved for failed penile reimplantation and the first penile reconstruction was performed in 1936 described by Bogoraz [11]. The use of a forearm flap for phallic replacement described by Chang represents the most used method with creation of a neo-urethra [12, 13].
Conclusion
The section of the penis is a rare urological emergency and requires multidisciplinary care involving the urologist, the resuscitator and the psychiatrist. The severity of the lesions and the consultation time represent the important factors for the choice of treatment.
Consent
Patient’s family has given her informed consent for the case to be published.
Conflict of Interest
None.
Acknowledgments
At the end of this work, we would like to sincerely thank all the people who contributed to its writing, To Dr. Zineb from department of anesthesia and resuscitation for the success of the anesthesia despite the patient was not cooperating.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
-
Ghannam Y, Nedjim AS, Abdi EM, Hagguir H, Moataz A, et al. (2021) Genital auto-mutilation, the second attempt was dramatic. Clin Surg Res Commun 5(2): 7-9.
-
Zior JR, Brady JD, Schlossberg SM (2001) Management of penile amputation injuries. World journal of surgery 25(12): 1602-1609.
-
Blacker KH, Wong N (1963) Four cases of autocastration. Arch Gen Psychiatry 8: 169-176.
-
Yilmaz AF, Sarikaya S, Yildiz S, Buyukalpelli R (1993) Rare complication of circumcision: penile amputation and reattachment. Eur Urol 23(3): 423-424.
-
Sanger JR, Matloub HS, Yousif NJ, Begun FP (1992) Penile replantation after self-inflicted amputation. Ann Plast Surg 29(6): 579-584.
-
Hayhurst SW, O’Brien BM, Ishida H (1974) Experimental digital replantation after prolonged cooling. Hand 6(2): 134-141.
-
Wei F, McKee, NH, Huerta FJ, Robinette MA (1983) Microsurgical replantation of a completely amputated penis. Ann Plast Surg 10(4): 317-321.
-
Ehrich WS (1929) Two unusual penile injuries. J Urol 21(2): 239-241.
-
Carroll PR, Lue TF, Schmidt RA, Trengrove-Jones G, McAninch JW, et al. (1985) Penile replantation: current concepts. J Urol 133(2): 281-285.
-
Jordan GH, Gilbert DA (1989) Management of amputation injuries of the male genitalia. Urol Clin North Am 16(2): 359-367.
-
Bogoraz NA (1936) Plastic restoration of the penis. Sov Khir.
-
Chang TS, Hwang WY (1984) Forearm flap in one-stage reconstruction of the penis. Plast Reconstr Surg 74(2): 251-258.
-
Greilsheimer H, Groves JE (1979) Male genital self mutilation. Arch Gen Psychiatry 36(4): 441-446.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report