What Exactly is the TUR Syndrome and How Should it be Treated?
The introduction of this article reports a mini review of the subject. The TUR syndrome is precisely defined. The pathoaetiology, clinical picture and effective therapy are reported. The TUR syndrome is defined as severe cardiovascular reaction shock induced by massive gain of the sodium-free irrigating fluid such as 1.5% Glycine into the cardiovascular system and is characterized by severe hyponatremia. The main presentation is severe cardiovascular shock and post-operative coma and convulsions, but other manifestations of the multiple organ dysfunction syndrome occur. The correct lifesaving therapy for the TUR syndrome, hyponatremia and ARDS is hypertonic sodium of 5%NaCl and 8.4% NaCo
Introduction
The transurethral resection of the prostate (TURP) procedure has long been recognised as the safest method of prostatectomy [1] and is currently the operation of choice for prostatic enlargement. However, like any other operation, it has its complications both general and specific. Specific complications may be immediate such as severe bleeding and the TUR syndrome or delayed such as urethral stricture formation.
The TUR syndrome is one of its acute complications with an average postoperative mortality of 1.59% [2]. Other authors have calculated that it accounts for a morbidity of 17-24% and a mortality of 1-2% [3, 4]. Based on a prospective study an incidence of 7% with a mortality of 1% was reported [5]. Since 10% of males above the age of 40 years will, sooner or later, become candidate for prostatectomy [6], the total number of patients at risk from this complication is considerable [4].
Creevy first described the TUR syndrome as acute water intoxication that led to intravascular haemolysis, jaundice and acute tubular necrosis and death from renal failure at the time when water was used as the irrigating solution during the TURP procedure [7, 8, 9, 10, 11]. Creevy credited both Foley and Mclaughlin for similar and independent observations. Foley observed red urine, due to intravascular haemolysis, spurting from the ureteric orifices during the TURP procedure [7].
Non-haemolytic irrigating solutions were then introduced. Creevy used glucose and Nespit experimented with glycine. Nesbit outlined the criteria for a suitable irrigant as non-haemolytic, non-toxic, transparent, and cheap [12]. Saline was excluded because it disseminates electric current. Glycine was preferred to glucose because of the hyperglycaemia that may complicate the use of glucose solutions [12]. Urea, Mannitol and Cytal (mainly composed of sorbitol and mannitol) and other irrigating fluids were introduced later [13].
The introduction of non-haemolytic and non-electrolytes solutions was considered the most important advance of transurethral surgery [14]. Such solutions are non- haemolytic to red blood cells but may be either hypo- or iso- osmotic to the plasma. Plasma osmolality measures 280-300 mosm/l while that of 1.5% glycine is reported to be 220 but measures 195 mosm/l by freezing point depression.
Non-haemolytic solutions have reduced the morbidity and mortality of the TUR syndrome, as compared to water intoxication, by half from 50% and 4% respectively [9, 11]. Red cell haemolysis and its consequences such as hemoglobinemia, tubular necrosis, renal failure and jaundice have become no longer features of the TUR syndrome [15], but a complex clinical syndrome has continued to occur [16].
Although the cause of the TURP syndrome remains controversial and even its existence may be doubted [17], it has become clear that it is associated with the systemic absorption of a large volume of the sodium-free irrigating fluid [18]. Fluid absorption may occur through the peri- prostatic venous plexus of veins directly injected by the resectoscope flow into the circulation after breaching the prostatic capsule [19, 20], or through the peritoneal membrane in cases of intra-peritoneal perforations [21, 13].
In 1956 Harrison III et al recognized the concept of hyponatraemic shock as the patho-aetiology of the TUR syndrome and introduced 5% NaCl as its successful treatment. This successful treatment was overlooked because it was considered by the medical authorities on hyponatraemia that hypertonic sodium therapy (HST) was contraindicated. In 1990 (Ghanem and Ward) introduced the concept of Volumetric overload shocks as the patho-aetiology of the TUR syndrome and rejuvenated HST in its successful treatment. It has been demonstrated that HST restores serum sodium and osmolality with a matching immediate improvement in clinical picture (Figure 1).
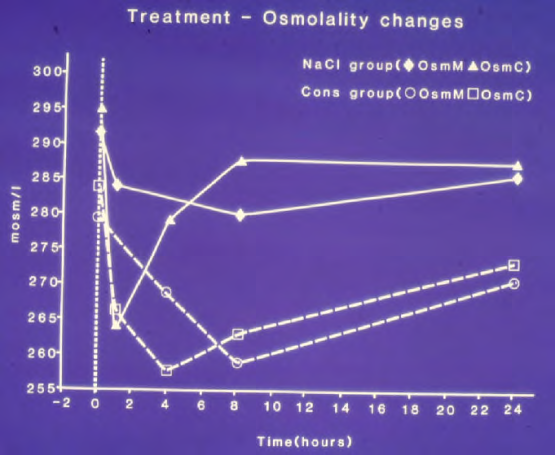
Figure 1: Shows mean changes in measured serum osmolality (OsmM) and calculated osmolality (OsmC)a and serum sodium concentration in patients with the TURP syndrome comparing those infused with 5% hypertonic sodium (solid lines) and those treated conservatively (slashed lines). OsmC was calculated from the formula 2xNa+urea+glucose in mmol/l of serum concentration48 thus reflecting changes in serum sodium concentration. The vertical dotted line represents the start of operation (Time B) followed by C, C1, C2 (end of treatment) and D, respectively.
The latest shift to using normal saline as the irrigating solution may eradicate the TUR syndrome with its characteristic hyponatraemia from urological practice but it will be reincarnated into ARDS as predicted by Ghanem [22, 23, 24, 25] based on the concept of VO induced by saline based fluids [22].
Definition
The TUR syndrome is defined as severe cardiovascular reaction shock induced by massive gain of the sodium-free irrigating fluid such as 1.5% Glycine into the cardiovascular system and is characterized by severe hyponatraemia of <120 mmol/l.
Patho-Aetiology
The toxic hypothesis of glycine and hypernatremia. These have traditionally been used as the patho-etiological explanation for the TUR syndrome with little impact on its correct management and understanding of the condition [26, 27]. Hahn, et al. Remains a firm believer of the toxic hypothesis [28, 29]. However, neither hyponatraemia nor the high serum Glycine reached statistical significance in multiple regression analysis Table 1 but volumetric overload was the most highly significant factor (p=0.0007) in a prospective study on the TUR syndrome [22].
| P | T Value | Std. Value | Std. Err | Value | Parameter | |
|---|---|---|---|---|---|---|
| 0.773 | Intercept | |||||
| 0.0007 | 3.721 | 1.044 | 0.228 | 0.847 | Fluid Gain (l) | |
| 0.0212 | 2.42 | -0.375 | 0.014 | 0.033 | Osmolality | |
| 0.0597 | 1.95 | 0.616 | 0.049 | 0.095 | Na+ (C_B) | |
| 0.4809 | 0.713 | 0.239 | 0.087 | 0.062 | Alb (C_B) | |
| 0.2587 | 1.149 | -0.368 | 0.246 | -0.282 | Hb (C_B) | |
| 0.4112 | 0.832 | -0.242 | 5.98E-05 | -4.97E-05 | Glycine (C_B) |
Table 1: Shows the multiple regression analysis of total per-operative fluid gain, drop in measured serum osmolality (OsmM), sodi
Volumetric Overload Shocks (VOS)
This concept is relatively new and has proved most successful in saving the lives of the TUR syndrome cases [22, 23, 24]. Most of the volumetric overload (VO) in the TUR syndrome is type one induced by sodium-free fluids such as Glycine, Mannitol, Glucose and Sorbitol. Also any fluid that is intravenously infused during the procedure contributes to the pathogenesis. Table 1 demonstrates that VO is the most highly significant factor in causing the TUR syndrome. The magnitude of the VO is demonstrated in Figures 2 &
3. The concept also allows recognizing VO shocks (VOS) that is of two types: Type 1 induced by sodium-free fluids and type 2 induced by sodium-based fluids which clearly indicate that VOS should not be treated with further volume expansion which is lethal. The correct treatment is HST of 5%NaCl and 8.4%Na Co3. Though this good therapy remains contraindicated in the management of Hyponatraemia [26, 27, 30]. These authorities on hyponatraemia changes their views and approved HST as a good successful treatment.
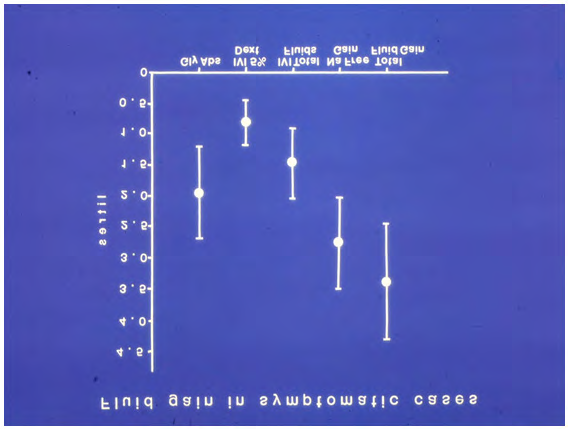
Figure 2: shows the means and standard deviations of volumetric overload in 10 symptomatic patients presenting with shock and hyponatraemia among 100 consecutive patients during a prospective study on transurethral resection of the prostate. The fluids were of Glycine absorbed (Gly abs), intravenously infused 5% Dextrose (IVI Dext) Total IVI fluids, Total Sodium-free fluid gained (Na Free Gain) and total fluid gain in liters.
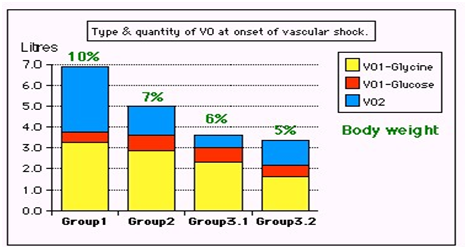
Figure 3: shows volumetric overload (VO) quantity (in liters and as percent of body weight) and types of fluids. Group 1 was the 3 patients who died in the case series as they were misdiagnosed as one of the previously known shocks and treated with further volume expansion. Group 2 were 10 patients from the series who were correctly diagnosed as volumetric overload shock and treated with hypertonic sodium therapy (HST). Group 3 were 10 patients who were seen in the prospective study and subdivided into 2 groups; Group 3.1 of 5 patients treated with HST and Group 3.2 of 5 patients who were treated with guarded volume.
Clinical Picture
The clinical picture of the TUR syndrome is predominated by the cerebral symptoms of coma, convulsions, and bizarre paralysis [31, 32]. However, the cardiovascular shock of VOS precedes this presentation. Other manifestations of the multiple organ dysfunction syndrome (MODS) appear later in the surviving cases that present with features of the acute respiratory distress syndrome (ARDS) (Table 2). Table 3 shows the mean summary of data on biochemical abnormalities, postoperative serum solute changes, therapy and outcome comparing the 3 groups of 23 case series patients whose VO is shown in Figure 2.
| Cardiovascular | Respiratory | Renal | Hepatic & GIT | |
|---|---|---|---|---|
| Numbness | Hypotension | Cyanosis. | Oliguria | Dysfunction: |
| Tingling | Bradycardia | FAM | Annuria | Bilirubin ↑ |
| SBB | Dysrhythmia | APO) | Renal failure or | SGOT ↑ |
| COC | CV Shock* | RA | AKI9 | Alkaline Phosph. |
| Convulsions | Cardiac Arrest | Arrest | Urea ↑ | GIT symptoms. |
| Coma | Sudden Death | CPA | Creatinine ↑ | DGR |
| PMBCI | Shock lung | Paralytic ileus | ||
| ARDS | Nausea & Vomiting. |
Table 2: Shows the manifestations of VOS 1 of the TURP syndrome for comparison with ARDS manifestations induced by VOS2. The mani
| 1 | Gr1 | Gr2 | Gr3 | Gr3.1 | Gr3.2 | Normal Units | ||
|---|---|---|---|---|---|---|---|---|
| 2 | Number of patients 3 | 10 | 10 | 5 | 5 | mean | ||
| 3 | Age 71 | 70 | 75 | 72 | 78 | 72 Years | ||
| 4 | Body weight (BW) 69 | 70 | 68 | 71 | 65 | 69 Kg | ||
| 5 | Postoperative serum solute concentration | Preoperative | ||||||
| 6 | Osmolality | 271 | 234 | 276 | 282 | 271 | 292 | Mosm/1 |
| 7 | Na+ | 110 | 108 | 120 | 119 | 121 | 139 | Mmol/1 |
| 8 | Ca++ | 1.69 | 1.79 | 1.85 | 1.84 | 1.86 | 2.22 | ‘’ |
| 9 | K+ (P<.05) | 5.6 | 4.8 | 5 | 4.9 | 5 | 4.46 | ‘’ |
| 10 | Co (P=.002) 2 | 23 | 23 | 25.5 | 24 | 26.4 | 27.3 | ‘’ |
| 11 | Glucose | 13.2 | 17.3 | 16.4 | 15.9 | 16.9 | 6.2 | ‘’ |
| 12 | Urea (P=.0726) | 26.5 | 9 | 6.6 | 6.8 | 6.4 | 6.7 | ‘’ |
| 13 | Bilirubin (P<.05) | 19 | 16 | 8 | 6 | 9 | 7 | ‘’ |
| 14 | AST | 124 | 32 | 20 | 18 | 21 | 20 | ‘’ |
| 15 | Protein | 43 | 52 | 48 | 44 | 52 | 62 | g/l |
| 16 | Albumin | 23 | 30 | 30 | 28 | 32 | 39 | ‘’ |
| 17 | Hb (P=.0018) | 119.3 | 127.9 | 114.5 | 105.2 | 123.8 | 123.8 | ‘’ |
| 18 | WCC (P<.005) | 18.9 | 16.2 | 7.5 | 7.8 | 7.2 | 8 | per HPF |
| 19 | Glycine | 10499 | 293 | µmol/1 | ||||
| 20 | Therapy | CT | HST | Randomized: | HST | CT© | ||
| 21 | Outcome | Death | Full Recovery | Full Recovery | Morbidity |
Table 3: Shows the mean summary of data on biochemical abnormalities, therapy and outcome comparing the 3 groups of 23 case serie
Table 3: Shows the mean summary of data on biochemical abnormalities, therapy and outcome comparing the 3 groups of 23 case series patients whose VO is shown in (Figure 3). Groip-1 was the 3 patients who died and had post-mortem examination, Group-2 were a series of severe TURP syndrome cases successfully treated with hypertonic sodium therapy (HST), and Group-3 were 10 patients encountered in the prospective study who were randomized between HST (3.1) and conservative treatment (CT) (3.2). The significant changes of serum solute contents are shown in bald font with the corresponding p- value. Most of the patients showed manifestation of ARDS of which the cerebral manifestation predominated, being on initial presentation (Regional Anaesthesia) and representation of VOS 1 (General Anaesthesia). However, most patients were given large volume of saline that elevated serum sodium to near normal while clinical picture became worse. They suffered VOS2 that caused ARDS.
Therapy of VOS causing the TUR syndrome, hyponatraemia, and ARDS
Prevention: Being iatrogenic complications of fluid therapy, both VOS causing the TUR syndrome and ARDS are preventable. To prevent VOS and ARDS a limit to the maximum amount of fluid used during shock resuscitation or major surgery must be agreed upon (New guidelines are required). Surgical care providers must exercise judicious use of crystalloid fluid administration in the trauma bay, ICU, and floor.
Replace the loss in haemorrhagic hypovolaemic shock but do not overdo it. If hypotension develops despite volume replacement later during ICU stay, inotropic drugs, hydrocortisone 200 mg and hypertonic sodium therapy (HST) should be used-see later. The latter restores the pre-capillary sphincter tone (peripheral resistance) so that the capillary works as normal G tube again, but NO isotonic crystalloids or colloids over-infusions is required. This corrects shock and arrythmia and elevates blood pressure.
To learn the new correct science, one must unlearn the old incorrect habits.
The following practices should be abandoned:
Bolus Fluid Therapy in Surgical Patients
Abandon the aggressive current liberal regimen of Early Goal-Directed Therapy (EGDT) in treating shocked and septic patients. Multiple huge multicentre trials have proved it to be the wrong practice. Please refrain from persisting to elevate CVP to levels above 12 and up to 18-22 cm using isotonic saline-based fluids in shock management. This is a major cause for inducing VOS and ARDS during shock resuscitation, particularly septic shock.
Therapeutic
Hypertonic sodium therapy (HST) of 5%NaCl and/ or 8.4%NaCo3 has truly proved lifesaving therapy for the TUR syndrome and acute dilution HN as well as Secondary VOS 2 that complicates fluid therapy of VOS 1 causing ARDS [32, 22, 23]. It works by inducing massive diuresis being a potent suppressor of antidiuretic hormone. It may also work on the capillary pre-sphincter restoring its tone [33].
My experience in using it for treating established ARDS with sepsis and primary VOS 2 that causes ARDS is limited.
However, evidence on HST suggests it will prove successful if given early, promptly, and adequately to ARDS patients while refraining from any further isotonic crystalloid or colloid fluid infusions using saline, HES and/or plasma therapy- just give the normal daily fluid requirement and no more. After giving HST over one hour using the CVP catheter already inserted, the patient recovers from AKI and produces through a urinary catheter massive amount of urine of 4-5 litres as you watch. This urine output should not be replaced. Just observe the patient recovering from his AKI, coma and ARDS and asks for a drink. This is done in addition to the cardiovascular, respiratory, and renal support on ICU. Patients with AKI on dialysis, the treating nephrologist should aim at and set the machine for inducing negative fluid balance.
The HST of 5%NaCl and/or 8.4%NaCo3 is given in 200 ml doses over 10 minutes and repeated. I did not have to use more than 1000 ml during the successful treatment of 16 ARDS patients. Any other hypertonic sodium concentration is not recommended. A dose of intravenous diuretic may be given but it does not work in a double or triple the normal dose. A dose of 200 mg of hydrocortisone is most useful. Antibiotic prophylactic therapy is given in appropriate and adequate doses to prevent sepsis and septic shock. No further fluid infusions of any kind crystalloids, colloids and blood are given. The urinary loss should not be replaced as this defeat the objective of treatment.
Conflict of Interest
None
Funds Received
None
References
-
Mitchell JP (1970) Transurethral resection. Br Med Jour 3(5717): 241-246.
-
Whitfield HN, Mills VA (1985) Percutaneous nephrolithotomy A report of 150 cases. Br J Urol 57(6): 603-604.
-
Chilton CP, Morgan RJ, England HR, Paris AM, Blandy JP, et al. (1978) A critical evaluation of the results of transurethral resection of the prostate. Br J Urol 50(7): 542-546.
-
Rhymer JC, Bell TJ, Perry KC, Ward JP (1985) Hyponatraemia following transurethral resection of the prostate. Br J Urol 57(4): 450-452.
-
Editorial (1980) Second best prostatectomy. Br Med Jour 280(6214): 590.
-
Sellevold O, Breivik H, Tveter K (1983) Changes in oncotic pressure, osmolality and electrolytes following transurethral resection of the prostate using glycine as irrigant. Scand J Urol Nephrol 17(1): 31-36.
-
Creevy CD (1947) Haemolytic reactions during transurethral prostatic resection. J Urol 58(2): 125-131.
-
Creevy CD, Webb EA (1947) A fatal haemolytic reaction during transurethral prostatic resection. Surgery 21(1): 56-66.
-
Creevy CD (1951) The mortality of transurethral resection of the prostate. J Urol 65(5): 876-882.
-
Mclaughlin WL, Holyoke JB, Bowler JP (1947) Oliguria during transurethral resection of the prostate. J Urol 58(1): 47-60.
-
Goodwin WE, Cason JF, Scott WW (1951) Haemoglobinaemia and lower nephron nephrosis following transurethral prostatic surgery. J Urol 65(6): 1075-1092.
-
Nesbit RM, Glickman SI (1948) The use of glycine as an irrigating medium during transurethral resection. J Urol 59(6): 1212-1216.
-
Marmar JL, Allen SD (1970) The transurethral reaction secondary to intraperitoneal extravasation of the irrigating solution. J Urol 104(3): 457-458.
-
Emmett JL, Gilbaugh JH, McLean P (1969) Fluid absorption during transurethral resection: Comparison of mortality and morbidity after irrigation with water and non-haemolytic solutions. J Urol 101(6): 884-889.
-
Hagstrom RS (1955) Studies on fluid absorption during transurethral prostatic resection. J Urol 73(5): 852-859.
-
Berg G, Fedor EJ, Fisher B (1962) Physiologic observations related to the transurethral resection reaction. J Urol 87: 596-600.
-
Goel CM, Badenoch DF, Fowler CG, Blandy JP, Tiptaft RC, et al. (1992) Transurethral syndrome. A prospective study. Eur Urol 21(1): 15-17.
-
Rao PN (1987) Fluid absorption during urological surgery. Br J Urol 60(2): 93-99.
-
Griffin M, Dobson L, Weaver JC (1955) Volume of irrigating fluid transfer during transurethral prostatectomy, studies with radioisotopes. J Urol 74(5): 646-651.
-
Maluf NS, Boren JS, Brandes GE (1956) Absorption of irrigating solution and associated changes upon transurethral resection of the prostate. J Urol 75(5): 824-836.
-
Thomas D, Hales P (1984) Overhydration during transurethral resection of the prostate using glycine as an irrigating solution. Anaesth Intensive Care 12(4): 366-369.
-
Ghanem AN, Ward JP (1990) Osmotic and metabolic sequelae of volumetric overload in relation to the TURP syndrome. Br J Urol 66(1): 71-78.
-
Ghanem AN, Ghanem SA (2016) Volumetric Overload Shocks: Why Is Starling’s Law for Capillary Interstitial Fluid Transfer Wrong? The Hydrodynamics of a Porous Orifice Tube as Alternative. Surgical Science 7(6): 245- 249.
-
Ghanem SA, Ghanem KA, Ghanem AN (2017) Volumetric Overload Shocks in the Patho-Etiology of the Transurethral Resection of the Prostate (TURP) Syndrome and Acute Dilution Hyponatraemia: The Clinical Evidence Based on Prospective Clinical Study of 100 Consecutive TURP Patients. Surg Med Open Access J 1(1).
-
Ghanem ANM (2021) The TUR Syndrome May Vanish from Urology but will be Re-Incarnating as ARDS after Saline Use as Irrigating Fluid in Endoscopic Surgery. J Urol Nephrol 6(2): 000195.
-
Arieff AI (1986) Hyponatraemia, convulsion, respiratory arrest and permanent brain damage after elective surgery in healthy women. N Engl J Med 314(24): 1529- 1535.
-
Arieff AI (1993) Management of hyponatraemia. Br Med Jour 307(6899): 305-308.
-
Hahn RG, Sandfeldt L, Nyman CR (1998) Double blind randomized study of symptoms associated with absorption of glycine 1.5% or mannitol 3% during transurethral resection of the prostate. J Urol 160(2): 397-401.
-
Hahn RG (1997) Irrigating fluids in endoscopic surgery. Br J Urol 79(5): 669-680.
-
Ayus JC, Krothapalli RK, Arieff AI (1987) Treatment of symptomatic hyponatraemia and its relation to brain damage. N Engl J Med 317(19): 1190-1195.
-
Henderson DJ, Middleton RG (1980) Coma from hyponatraemia of the transurethral resection of prostate. Urology 15(3): 267-271.
-
Harrison RH, Boren JS, Robison JR (1956) Dilutional hyponatraemic shock: another concept of the transurethral prostatic reaction. J Urol 75(1): 95-110.
-
Danowski TS, Winkler AW, Elkinton JR (1946) The treatment of shock due to salt depression; comparison of isotonic, of hypertonic saline and of isotonic glucose solutions. J Clin Invest 25: 130-138.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report