Malakoplakia of the Urachus
Malakoplakia is a chronic inflammatory pathology that can affect any organ in the body. Urological malakoplakia presents several clinical manifestations, depending on its location. Most often, it is responsible for hematuria, which may be mistaken for a neoplastic pathology. Positive diagnosis is made by anatomopathological study, which shows the presence of pathognomonic Michaelis-Gutmann bodies. Treatment is based on antibiotic therapy, with the possibility of surgery if medical treatment fails. We report the case of a 45-year-old female patient who presented with hypogastric swelling and haematuria, and was first diagnosed with a malignant tumour of the urachus and went for aggressive surgery. Histological examination confirmed the diagnosis of malakoplakia.
Introduction
Malakoplakia is a rare chronic inflammatory disease that was identified in 1901 by Professor von Hansemann and first reported in 1902 by Michaelis and Guttman. Since then, malakoplakia has been reported in a multitude of organ systems, including the gastrointestinal tract, bones, lungs and skin [1]. Urological malacoplakia presents a multitude of clinical presentations, depending on the location of the disease, and can affect any part of the urinary tract, with the bladder most usually involved, followed by the renal parenchyma, ureter and renal pelvis [2].
Malakoplakia is characterized microscopically by a collection of large mononuclear cells with abundant cytoplasm. These cells are called Hanseman’s macrophages and are full of calcium- and iron-loaded lysosomal material known as Michaelis-Gutman bodies [3]. Misdiagnosis is common, with lesions often mistaken for renal abscesses or malignant tumors, particularly in the case of concomitant pulmonary lesions that may simulate metastatic disease [2].
We report the case of a 45-year-old female patient, with no particular pathological history, whose disease history dates back to 4 months before her hospitalization in the urology department, with the appearance of a hypogastric tumefaction associated with mictional burning and a few episodes of hematuria. Due to unsustainable living conditions, low socio-economic status, poverty and ignorance the patient did go to see a doctor until there was a hypogastric mass and pus getting out of the umbilicus. On clinical examination, the patient was in good general condition, with normal vital signs. The abdominal area showed a hypogastric mass adherent to the skin, non-mobile in depth, with discharge of pus-like serosities from the umbilicus on pressure.
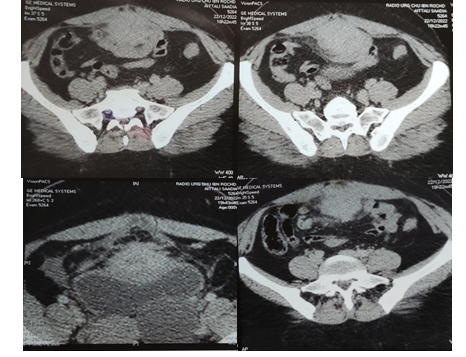
ACT scan revealed a fairly well-limited, well-contoured supravesical tissue mass, enhanced after injection of contrast product, delineating areas of fluid and fine calcifications in places, measuring 46x48x112 mm in diameter. It invades the anterior wall and bladder dome, without visualization of an endoluminal bud, as well as the anterior peritoneal sheet, transversalis fascia, rectus abdominis muscles and surrounding subcutaneous fat. Posteriorly, it came into intimate contact with a few of the bowel loops, with no clear dividing line. No secondary lesions were found. A malignant tumour of the uracula was suggested as the first diagnosis (Figure 1).
Given the strong suspicion of malignancy, the patient was referred to the operating room for surgical excision of her mass. Initial cystoscopy revealed a few nodules in the dome and anterior wall of the bladder, but biopsy revealed no cellular lesions suspicious of malignancy. The surgical approach was a laparotomy with sacrifice of the skin over the suspicious mass and all underlying tissues. The mass was adherent to the bladder dome and a bowel loop, which were also removed (Figure 2).
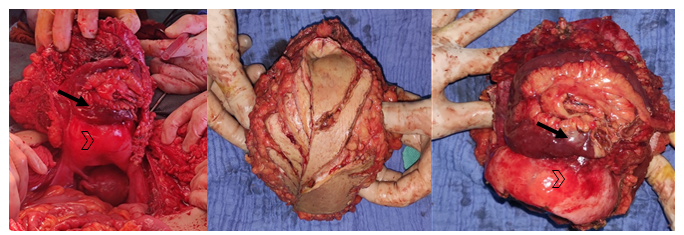
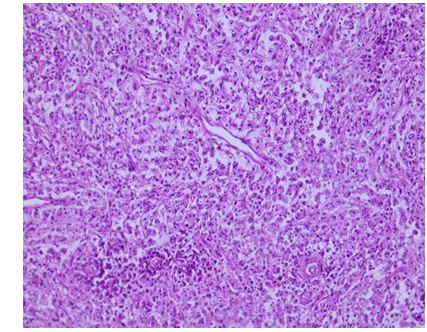
Figure 2 : Intraoperative images of the resected mass and after resection. (Arrowhead : bladder dome ; Arrow : bowel loop) Histological examination revealed oval basophilic intracellular and extracellular inclusions corresponding to Michaelis-Gutmann bodies. The diagnosis of malakoplakia was confirmed (Figure 3).
The patient was put on fluoroquinolones for 6 weeks. Clinical and scannographic controls at 3 and 6 months were good.
Discussion
Malakoplakia is a rare chronic inflammatory disease that most often affects the genitourinary tract, but also other systems including the gastrointestinal tract, lungs, thyroid and skin. Most often, malakoplakia is seen in the urogenital tract, with a predominance in females (female-to-male ratio 4:1). Age at diagnosis ranges from 6 weeks to 85 years, with an average age of presentation of 50 years. Malakoplakia is also more frequent in immunocompromised patients [1].
In fact, underlying dysfunction of the immune system plays an important role in the pathogenesis of malakoplakia. The disease results from an acquired defect in macrophage lysosomal function, leading to poor digestion of bacteria after phagocytosis. The hypothetical etiology of the defective macrophage function is the result of a decrease in the level of intracellular cyclic guanosine monophosphate (cGMP) interfering with microtubular function and lysosomal activity, resulting in incomplete bacterial clearance. Accumulation of partially digested bacteria in macrophages leads to calcium and iron accumulation on residual bacterial glycolipid, resulting in the formation of intracytoplasmic and extracytoplasmic round to oval basophilic structures known as Michaelis-Gutmann bodies, which are considered pathognomonic of malakoplakia. Another important hypothesis is that of a defective immune regulatory system leading to impaired mononuclear phagocytosis and lysosomal hydrolytic functions observed in cases of alcohol abuse, malnutrition, organ transplantation, intake of certain drugs such as steroids or cytotoxic agents, malignant tumors and chronic diseases such as diabetes mellitus, autoimmune diseases and sarcoidosis [3].
Malakoplakia is most often associated with Escherichia coli infection, but other organisms, such as Staphylococcus aureus, Proteus and Klebsiella, can also cause the condition. Most patients diagnosed with malakoplakia have a history of recurrent urinary tract infection [2]. With a variety of clinical manifestations, malakoplakia can easily be confused with a malignant tumor of the corresponding organ depending on the location of the disease, and it can affect any part of the body [4]. Malakoplakia presents clinically with a wide spectrum of outcomes depending on the organs involved. Bladder malakoplakia manifests as irritative symptoms of the lower urinary tract and hematuria, mimicking a malignant tumor. Ureteral malakoplakia may manifest as obstruction and stricture formation. Malakoplakia of the renal parenchyma may cause fever, flank pain and a mass. Testicular malakoplakia may manifest as orchiepididymitis. Prostatic malakoplakia may mimic carcinoma of the prostate, as it may present as a hard induration on rectal examination [5].
A urinary CT scan can be used to assess multiple lesions and evaluate the renal impact of parenchymal and ureteral lesions. Renal lesions are usually segmentally or diffusely hypodense, while ureteral lesions are manifested by gaps, leading to a differential diagnosis with renal parenchymal and urothelial tumours. Final diagnosis is based on histology [6]. Histologically, it is characterized by the presence of patches of histiocytes with granular cytoplasm (von Hansemann cells) mixed with round to oval intracellular and extracellular basophilic inclusions, known as Michaelis-Gutmann bodies, in a context of infiltration by mixed inflammatory cells [3].
At present, there are no clear guidelines for the treatment of malakoplakia. According to the literature, the prognosis of malakoplakia in all organs after treatment is good. The main method of treatment is antibacterial therapy, and the antibiotics used are those that concentrate intracellularly in macrophages, such as quinolones (the mainstay of treatment), trimethoprim and rifampicin. Ascorbic acid has been used to increase levels of cGMP and cyclic AMP in monocytes, which may represent an effective therapeutic strategy, although it is under trial. In addition, as malakoplakia is associated with immunosuppression, stopping immunosuppressive drugs is usually necessary depending on the risk/benefit ratio. When conventional drug therapy is ineffective, surgical treatment may be recommended, along with postoperative anti-infective therapy [2, 3, 4, 6].
References
-
Chaudhry N, Vazzano J, Parwani A (2022) Case study: Malakoplakia of the bladder. Pathology - Research and Practice 237: 153852.
-
Cavallone B, Serao A, Audino P, Di Stasio A, Tiranti D, et al. (2018) Bilateral hydroureteronephrosis with renal failure caused by malacoplakia. Urologia févr 85(1): 36- 37.
-
Vaiphei K, Singh P, Verma GR (2012) Gallbladder malakoplakia in type 2 diabetes mellitus: a rare entity. Case Reports 2012 : bcr2012006601.
-
Gao P, Hu Z, Du D (2021) Malakoplakia of the bladder near the ureteral orifice: a case report. J Int Med Res 49(10): 030006052110507.
-
Hina S, Hasan A, Iqbal N, Shabbir MU, Sheikh AAE (2019) Malakoplakia of the Urinary Bladder and Unilateral Ureter. J Coll Physicians Surg Pak 29(6): 582‑584.
-
Sarkis P, Nawfal G, Mouaccadieh L, Daou I, Zanati M (2012) Malakoplakie rénale, urétérale bilatérale et vésicale : à propos d’un cas et revue de la littérature. Progrès en Urologie 22(15): 970‑973.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report