Unveiling the Secrets of Renal Cancer: From Risk Factors to Promising Therapeutic Strategies
Renal cancer, a global health concern, is on the rise. This mini-review explores the risk factors associated with renal cancer, including smoking, obesity, and genetic conditions. Delving into the molecular intricacies, it unveils the key mechanisms involved, such as mutations in tumor suppressor genes and dysregulation of signalling pathways. The discovery of oncometabolites sheds light on their potential as diagnostic biomarkers and therapeutic targets. Surgical resection remains a primary treatment option, but limited options exist for recurrent metastatic disease. However, innovative therapies aimed at oncometabolites offer hope for enhanced outcomes. Understanding the puzzle of renal cancer will empower us to effectively manage this formidable adversary.
Introduction
Renal cancer, also called kidney cancer or renal cell adenocarcinoma is the formation of malignant tumors originating from the cells that line the renal tubules. Renal cancer affects a significant number of people globally.
According to the International Agency for Research on Cancer (IARC), in 2020, there were approximately 431,000 new cases of kidney cancer worldwide. The advancement of technology and widespread usage of abdominal imaging has increased the detection of renal cancer and more than 50% of RCC are said to be detected incidentally [1]. Epidemiological studies have shown the rising incidence of RCC (Renal Cell Carcinoma) in rapidly developing countries. This rise can be attributed to the use of imagining techniques and established risk factors [2]. Renal cancer predominantly affects men with the average age of diagnosis typically occurring in older adults, around 65 years of age [3].
Some of the established risk factors that increase the chances of renal cancer include cigarette smoking, obesity, hypertension, and high blood pressure [4]. Renal cancer can have hereditary implications, with certain genetic conditions like von Hippel–Lindau disease, hereditary papillary renal cell carcinoma, hereditary leiomyomatosis, and Birt–Hogg–Dube syndrome serving as significant risk factors [5]. Various case studies have investigated the relationship between smoking and renal cancer that says that it is one of the few modifiable and the most significant risk factor for RCC. Carcinogenic compounds including beta-naphthyl-amine and polycyclic aromatic hydrocarbons present in cigarette smoke pass through the nephron and their metabolism can be linked to carcinogenesis [6].
Obesity is a well-established and modifiable risk factor that has been linked to various diseases, including renal cancer. Obesity is associated with diabetes and resistance to insulin. This can lead to increased levels of the hormones- insulin and insulin-like growth factor- 1 (IGF1) in the blood. These hormones control different signal transduction pathways, alteration in which can facilitate cell proliferation, angiogenesis, and ultimately, tumor growth [7, 8]. In a study, Larose and Scelo suggested that 25% of renal cell carcinoma can be attributed to obesity [9].
Hereditary renal cancer has been seen to develop earlier in life, as early as teenage even. In these cases, the tumors are generally multiple and found bilaterally [10]. Renal cancer exhibits various subtypes, with adenocarcinoma being the most common, particularly clear cell renal carcinoma and renal transitional cell carcinoma (RTCC), which originate from the renal parenchyma and renal pelvis respectively, predominantly affecting adults [4, 11]. The clear cell renal carcinoma being the most prevalent subtype, accounting for 70-75% of all RCC cases. Clear-cell renal carcinoma originates from the renal cortex or the proximal convoluted tubular epithelium. These tumor cells, rich in glycogen and lipids, exhibit a distinctive appearance when stained, appearing clear or translucent. The accumulation of glycogen and lipids imparts a yellowish color to the rapidly growing tumors formed by these cells [12]. In children, Wilms tumor or nephroblastoma is the most common type of renal cancer. It affects children of age 3 to 5 years and is caused due to genetic alterations [13]. The papillary or chromophil cell carcinoma is the second most common histological subtype of RCC. They account for 15% of renal cancers. They are seen to have areas of haemorrhage, necrosis, and cystic degeneration. It has 2 histological subtypes. Subtype 1 has a single layer of basophilic cells, whereas subtype 2 cells are covered with papillae having abundant granular eosinophilic cytoplasm. Subtype 2 is more aggressive than type 1 and is seen in the case of hereditary leiomyoma renal cell carcinoma. On the other hand, chromophobe carcinomas have large and pale cells that stain poorly. They have reticulated cytoplasm with perinuclear halos and appear uniformly hyperechoic in ultrasonography. They are closely related to oncocytomas. Collecting duct carcinoma or Bellini duct carcinoma is highly aggressive but is seen in less than 1% of malignant renal tumors. They are characterized by tubular epithelial dysplasia in the adjacent renal parenchyma. The tumors have a tubular or tubule-papillary growth pattern with irregular and infiltrating cells in the collecting duct walls and inflammation [14]. They are prevalent in males. Some other types include renal medullary carcinoma, Mucinous Tubular and Spindle Cell Carcinoma, Neuroblastoma-associated RCC etc (Figure 1).
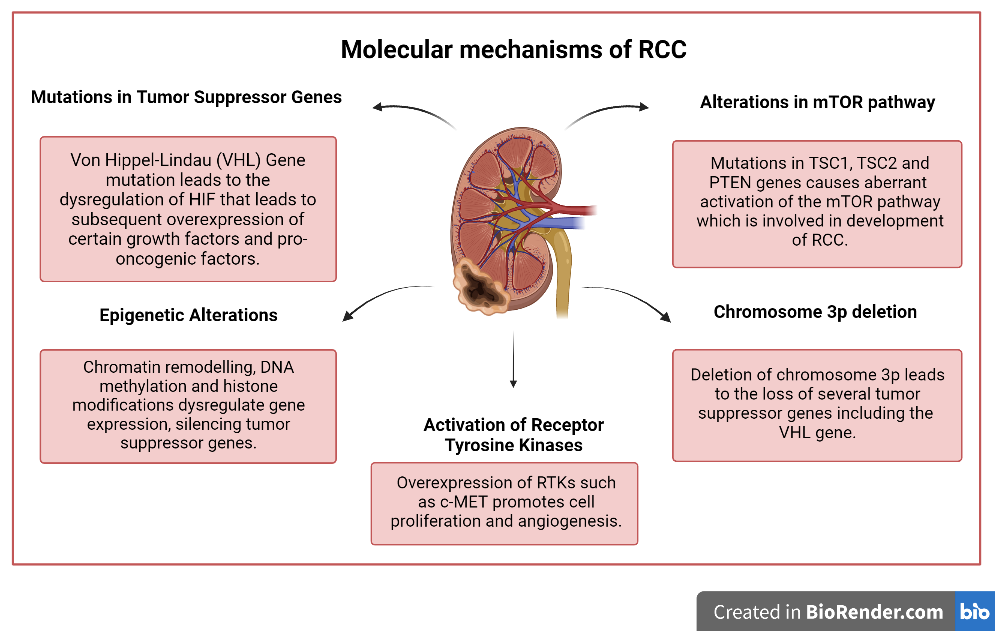
The complex molecular mechanisms underlying renal cancer involve various genetic and epigenetic alterations. Some of the key molecular mechanisms implicated in the development of renal cell carcinoma (RCC) are:
Mutations in Tumor Suppressor Genes such as the Von Hippel-Lindau (VHL) Gene
Mutations in the VHL gene are some of the most common genetic alterations seen in case of renal cell carcinoma [15]. The normal VHL gene produces a protein involved in regulating the stability of the hypoxia-inducible factor (HIF), which plays a crucial role in oxygen sensing and angiogenesis. Mutations in VHL gene lead to the dysregulation of HIF, which results in the subsequent overexpression of vascular endothelial growth factor (VEGF), platelet-derived growth factor receptor-alpha (PDGFRA), epidermal growth factor receptor (EGFR) and other pro-angiogenic factors. Increased production of VEGF and PDGF leads to dysregulation of angiogenesis. The new blood vessels supply nutrients and oxygen to the tumor and promote its growth. Activation of these oncogenes promotes cell proliferation, survival, and angiogenesis.
Activation of Receptor Tyrosine Kinases
Receptor tyrosine kinases (RTKs), such as the c-MET and fibroblast growth factor receptor (FGFR) families, are overexpressed or mutated in renal cancer [16]. Activation of these RTKs can promote cell proliferation, survival, and angiogenesis through various downstream signalling pathways.
Loss of Chromosome 3p
Chromosome 3p deletion is a common genetic alteration observed in RCC. Several tumor suppressor genes are located on chromosome 3p, including the VHL gene [17]. Their loss can lead to alterations in multiple signalling pathways and contribute to the development and progression of renal cancer.
Alterations in the Mammalian Target of Rapamycin (mTOR) Pathway
The mTOR pathway plays a crucial role in regulating cell growth, proliferation, and survival. Dysregulation of this pathway is frequently observed in RCC. Mutations in the tuberous sclerosis complex TSC1, TSC2 genes, and PTEN, which negatively regulate mTOR signalling, contribute to the aberrant activation of the mTOR pathway and development of RCC. Activation of the mTOR pathway promotes cell growth, proliferation and survival in RCC [18].
Epigenetic Alterations
Epigenetic changes, such as chromatin remodeling, DNA methylation and histone modifications, play a role in renal cancer. Mutations or alterations in genes encoding chromatin remodeling proteins, such as PBRM1 or BAP1, have been identified in renal cell carcinoma. Promoter hypermethylation of tumor suppressor genes such as CDKN2A, FHIT, and RASSF1A and global hypomethylation of genomic DNA are commonly observed in RCC. These epigenetic alterations can lead to the dysregulation of gene expression, silencing of tumor suppressor genes and contribute to tumor initiation and progression [19].
Role of Oncometabolites
Studies have shown that alteration in the levels of metabolites are indications of several types of cancers and support tumor formation by different mechanisms such as reduced oxidative phosphorylation, aerobic glycolysis, and elevated generation of biosynthetic intermediates [20]. These metabolites are called oncometabolites and they are nothing but conventional metabolites which when accumulate in abnormal amounts, have pro-oncogenic effects. Some characterized oncometabolites are succinate, fumarate, D-2-hydroxyglutarate (D-2-HG) and L-2-hydroxyglutarate (L-2-HG). These oncometabolites function by inhibiting α-ketoglutarate-dependent dioxygenase (αKGDDs) enzyme superfamily, which leads to pro-oncogenic outcomes in renal cancer. Oncometabolites play a role in epigenetic dysregulation as well [21, 22].
Symptoms and Diagnosis
The symptoms of renal cancer include hematuria, pain in the lower back, abdominal mass, fatigue, loss of appetite, weight loss, and anaemia. A study showed that patients suffering from local RCC usually showed symptoms like visible hematuria, pain, and abdominal mass. Whereas, in case of systemic RCC, weight loss, fatigue, and loss of appetite were more common [23]. Studies show that most cases of renal cancer are detected incidentally. The most common way is detection by abdominal imaging that was done for some other ailment. Lumbar and trans-abdominal ultrasonography performed for non-urological symptoms lead to its discovery [24].
Treatment
In patients where non-metastatic Tumors are detected in early stages, surgical resection is an effective cure. Metastasectomy is the only potentially curative procedure, which is crucial for disease management and cancer-specific survival (CSS) [25]. Radical or partial nephrectomy is a successful treatment option for RCC detected at an early stage. However, in cases of recurrent metastatic disease, treatment options are limited. Less invasive treatment options involve laparoscopy. Radiation therapy is another therapeutic option for RCC; however RCC is intrinsically radio resistant [26]. Certain oncometabolites are involved in cancer diagnosis and they act as therapeutic biomarkers. Novel therapies are targeted towards such oncometabolites as well.
Conclusion
In conclusion, renal cancer, or kidney cancer, is a significant and globally prevalent disease. It is influenced by various risk factors, including smoking, obesity, and genetic conditions. The molecular mechanisms underlying renal cancer involve genetic alterations, epigenetic changes, and dysregulation of signalling pathways. The identification of oncometabolites has shed light on metabolic dysregulation and its impact on tumor development. Early detection through incidental findings and accurate diagnosis is crucial for effective treatment. Surgical resection is the primary approach for non-metastatic tumors, while metastasectomy plays a vital role in managing metastatic disease. However, treatment options for recurrent metastatic renal cancer are limited. Further research and the development of targeted therapies, including those focused on oncometabolites, hold promise for improving patient outcomes in renal cancer management.
Author Contribution Statement
Banerjee A. designed the article theme, drafted the entire manuscript, and arranged the references. Bhowmick A. critically reviewed the manuscript and incorporated the necessary corrections.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
-
Rabjerg M, Mikkelsen MN, Walter S, Marcussen N (2014) Incidental renal neoplasms: is there a need for routine screening? A Danish single-center epidemiological study. APMIS 122(8): 708-714.
-
Rossi SH, Klatte T, Usher-Smith J, Stewart GD (2018) Epidemiology and screening for renal cancer. World Journal of Urology 36(9): 1341-1353.
-
Jani C, Abdallah N, Mouchati C, Jani R, Sharma R, et al. (2022) Trends of kidney cancer burden from 1990 to 2019 in European Union 15 + countries and World Health Organization regions. Sci Rep 12(1): 25485-254858
-
Chow WH, Dong LM, Devesa SS (2010) Epidemiology and risk factors for kidney cancer. Nature Reviews Urology 7(5): 245-257.
-
Cho E, Adami HO, Lindblad P (2011) Epidemiology of Renal Cell Cancer. Hematol Oncol Clin North Am 25(4): 651-665.
-
Padala SA, Padala SA, Barsouk A, Thandra KC, Saginala K, et al. (2020) Epidemiology of Renal Cell Carcinoma. World J Oncol 11(3): 79-87.
-
Pollak M (2012) The insulin and insulin-like growth factor receptor family in neoplasia: an update. Nat Rev Cancer 12: 159-169.
-
Turco F, Tucci M, Stefano RFD, Samuelly A, Bungaro M, et al. (2021) Renal cell carcinoma (RCC): fatter is better? A review on the role of obesity in RCC. Endocr Relat Cancer 28(7): R207-R216.
-
Scelo G, Larose TL (2018) Epidemiology and Risk Factors for Kidney Cancer. Journal of Clinical Oncology 36(36): 3574-3581.
-
Choyke PL, Glenn GM, Walther MM, Zbar B, Linehanet WM (2003) Hereditary renal cancers. Radiology 226(1): 33-46.
-
Chow WH, Devesa SS (2008) Contemporary epidemiology of renal cell cancer. Cancer Journal 14(5): 288-301.
-
Muglia VF, Prando A (2015) Renal cell carcinoma: histological classification and correlation with imaging findings. Radiol Bras 48(3): 166-174.
-
Leslie SW, Sajjad H, Murphy PB (2023) Wilms Tumor. Treasure Island (FL), StatPearls Publishing. Prasad SR, Humphrey PA, Catena JR, Narra VR, Srigley JR, et al. (2006) Common and Uncommon Histologic Subtypes of Renal Cell Carcinoma: Imaging Spectrum with Pathologic Correlation. Radiographics 26(6): 1795-1806.
-
Cowey CL, Rathmell WK (2009) VHL Gene Mutations in Renal Cell Carcinoma: Role as a Biomarker of Disease Outcome and Drug Efficacy. Curr Oncol Rep 11: 94-101.
-
Yamaoka T, Kusumoto S, Ando K, Ohba M, Ohmori T (2018) Receptor Tyrosine Kinase-Targeted Cancer Therapy. Int J Mol Sci 19(11): 3491.
-
Huebner K (2001) Tumor suppressors on 3p: A neoclassic quartet. Proc Natl Acad Sci U S A 98(26): 14763-14765.
-
Hann SC, Heathcote SA, Kim WY (2014) mTOR pathway in renal cell carcinoma. Expert Review of Anticancer Therapy 8(2).
-
Ramakrishnan S, Pili R (2013) Histone Deacetylase Inhibitors and Epigenetic Modifications as a Novel Strategy in Renal Cell Carcinoma. Cancer J 19(4): 333- 340.
-
Yang M, Soga T, Pollard PJ, Adam J (2012) The emerging role of fumarate as an oncometabolite. Front Oncol 2.
-
Khatami F, Aghamir SMK, Tavangar SM (2019) Oncometabolites: A new insight for oncology. Mol Genet Genomic Med 7(8): e873.
-
Yong C, Stewart GD, Frezza C (2019) Oncometabolites in renal cancer. Nature Reviews Nephrology 16: 156-172.
-
Vasudev NS, Wilson M, Stewart GD, Adeyoju A, Cartledge J, et al. (2020) Challenges of early renal cancer detection: symptom patterns and incidental diagnosis rate in a multicentre prospective UK cohort of patients presenting with suspected renal cancer. BMJ Open 10(5): e035938.
-
Vallancien G, Torres LO, Gurfinkel E, Brisset JM (1990) Incidental Detection of Renal Tumours by Abdominal Ultrasonography. Eur Urol 18(2): 94-96.
-
Dabestani S, Marconi L, Bex A (2016) Metastasis therapies for renal cancer. Curr Opin Urol 26(6): 566- 572.
-
Vugrin D (1987) Systemic therapy of metastatic renal cell carcinoma. Semin Nephrol 7: 152-162.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report