Incidental Discovery of Migrated Guidewire from Right Femoral Vein Catheterization: A Case Report
Background: Catheterization of central veins can be life-saving for gravely ill patients and remains the mainstay of vascular access for haemodialysis patients especially in the absence of arterovenous fistula. Femoral vein catheterization often comes in handy especially in emergency situations. This is nevertheless fraught with complications including: hemorrhage, femoral artery puncture, femoral nerve injury, pseudoaneurysm, fistula formation, thrombophlebitis, retroperitoneal hemorrhage, bowel perforation, urinary bladder puncture, and guidewire migration. However, guidewire migration has been considered a rare but serious and preventable complication. Case presentation: We report a case of a 64 year old end stage kidney disease patient who was on maintenance haemodialysis using femoral vein catheters as access. Patient was unaware he had a migrated guidewire in situ following femoral vein cannulation by unqualified health professionals. He remained asymptomatic until the migrated guidewire was incidentally discovered during an attempt at right internal jugular vein cannulation for placement of tunneled catheter for haemodialysis. Guidewire extraction was subsequently done through a right neck open surgery. Conclusion: Migrated guidewire is a rare complication of central vein cannulation. It is potentially preventable but prompt extraction should be done immediately if it occurs.
Abbreviations
AKI: Acute Kidney Injury; AVF: Arterovenous Fistula; CTU: Cardiothoracic Unit; ECG: Electrocardiogram; ESKD: End Stage Kidney Disease; RIJV: Right Internal Jugular Vein; MHD: Maintenance Haemodialysis; UNTH: University of Nigeria Teaching Hospital; WKD: World Kidney Day.
Introduction
Background
Catheterization of central veins can be life-saving for gravely ill patients. It remains the mainstay of vascular access for haemodialysis patients especially in the absence of arterovenous fistula (AVF). Femoral vein catheterization often comes in handy particularly in emergency situations but is fraught with complications including hemorrhage, femoral artery puncture, femoral nerve injury, pseudoaneurysm, fistula formation, thrombophlebitis, retroperitoneal hemorrhage, bowel perforation, urinary bladder puncture, and guidewire migration. Guidewire migration is considered a rare but serious complication.
The procedure for central vein cannulation was reformed by Seldinger in 1953 when he described a simplified “over a guidewire technique”.1This technique has become the popular method for catheterization of central veins. Despite improved outcome with the use of this modified technique, catheterization of central veins is still associated with a number of complications but guidewire migration has been considered a rare but grave complication2. This paper reports a case of incidental discovery and subsequent extraction of migrated guidewire in the right internal jugular vein (RIJV) from right femoral vein catheterization.
Case Report
Mr. OC, a 64year old petty trader, was diagnosed to have hypertension in 2010 but he was neither adherent to his prescribed drugs nor his clinic visits largely due to financial difficulties. In December 2020, a diagnosis of end stage kidney disease (ESKD) was made in a tertiary government hospital. At this point, he had no overt uremic symptoms and his urine output was between 500- 750mls/day. Hypertension remained poorly controlled as out-of-pocket payment for health services limited his ability to afford and adhere to his prescribed medications. Haemodialysis was subsequently prescribed in January, 2021 when he developed uremic symptoms including progressive weakness, anorexia, vomiting and excessive daytime somnolence. His urine output had dropped to 200-350mls/day. Unfortunately, he could only afford once weekly maintenance haemodialysis (MHD) via femoral vein catheters. He also received multiple blood transfusions when required because he could not sustain erythropoietin therapy. In February 2021, he was noted to have positive hepatitis B virus serology at the managing government tertiary hospital. As a result of this, he could only access haemodialysis services in private dialysis centers still using femoral vein catheters.
On hearing about free tunneled RIJV catheterization for haemodialysis being offered as part of a week- long activities to mark the 2021 world kidney day (WKD) celebration under The International Society of Nephrology sister renal centre partnership programme at University of Nigeria Teaching Hospital (UNTH), Ituku/ Ozalla, Enugu State, Nigeria, he presented at UNTH renal unit for enrolment on 4th March, 2021.
He was seen again at the procedure room of UNTH renal unit for free tunneled RIJV catheter placement on 9th March 2021. His physical examination findings were: axillary temperature of 36.7℃, normal volume and regular radial pulse with a rate of 86 beats per minute, blood pressure was 140/70mmHg and respiratory rate was 18 cycles per minute with an oxygen saturation of 97% on room air. Under aseptic conditions, his RIJV was easily cannulated ‘’blindly” but all efforts to subsequently advance the guidewire were futile as constant resistance was met. He was then booked for real- time ultrasound guided RIJV catheterization on 16th March 2021.
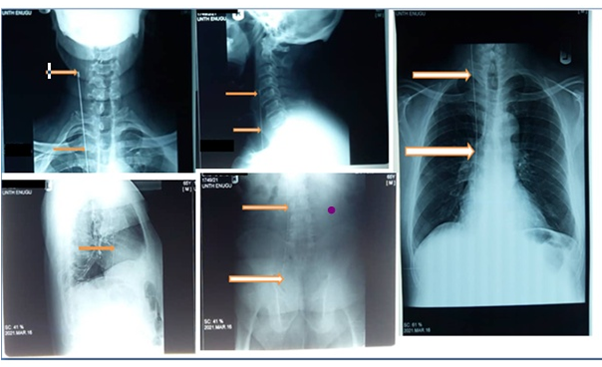
At the UNTH radiology department on the 16th March 2021, ultrasound scan of his neck revealed the presence of an echogenic longitudinal structure with an inverted “J” tip within the RIJV. He was then sent to do x-ray which revealed the presence of a radiopaque longitudinal structure at the right anterior aspect of his neck, extending through the thorax, abdomen and ending with a straight tip in the right true pelvis. This finding raised the suspicion of a migrated guidewire from previous femoral vein catheterization. Following this, patient revealed that his last two femoral vein catheterization done two weeks and a week earlier respectively in a private dialysis centre by a nurse and a dialysis machine technician were difficult, bloody, agonizing and prolonged. He also observed that on each of these two occasions, catheterization of his right femoral vein were unsuccessful. Hence, his left femoral vein was then catheterized to obtain haemodialysis access. An electrocardiogram (ECG) done the same day was essentially normal except for features of left ventricular hyperthrophy. He was then referred to the cardiothoracic unit (CTU) of UNTH. He remained stable, had no palpitation or chest pain and continued to get once weekly haemodialysis via left femoral vein catheters and subsequently presented to UNTH CTU out-patient clinic on 22nd March, 2021. Mr. OC was then worked up for foreign body extraction through the RIJV.
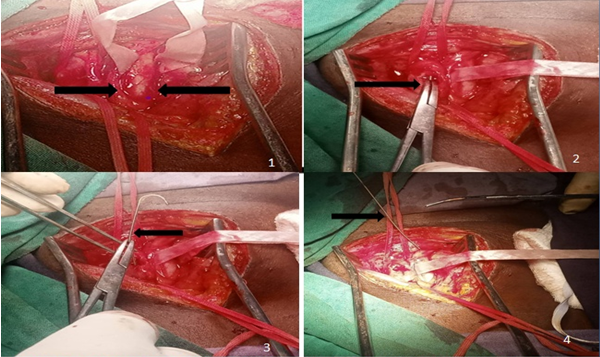
On 24th March, 2021 under general anaesthesia with endotracheal intubation, Mr. OC was placed in supine position with neck extended on a sandbag and tilted to the left. He received prophylactic antibiotics and skin preparation was done from the angle of the mandible to the nipple line. Skin incision was made along the anterior border of sternocleidomastoid muscle. His RIJV when exposed appeared cord-like and was subsequently isolated using a vascular loop. A transverse venotomy was made on the vein at the point where the inverted‘’J’’ tip of the guidewire was localized. The end of the guidewire was then clamped and gently pulled out through the exposed vein. The integrity of the guidewire was assessed to detect any fracture or breakage. The venotomy was closed with prolene 5-0 while the neck wound was closed in layers using Vicryl 2-0. The procedure was well tolerated. Post- operatively, he received intravenous fluid, anticoagulant, antibiotics and paracetamol. He was discharged two days after guidewire extraction on oral amoxicillin/clavulanic acid (500/125mg) 1capsule 8hourly for five days and tablet paracetamol 1g 8hourly for three days. He did not return for his follow-up visits until 19th May, 2021, when he presented at the accident and emergency unit of our hospital with progressive generalized body swelling, dyspnoea at rest, vomiting, drowsiness and anuria. Unfortunately, he could only afford one session of MHD, and he died on 2nd June, 2021.
Discussion
Critically ill patients are often in need of vascular access. At such scenarios, catheterization of central veins becomes a life- saving procedure. Indications for central vein catheterization include: vascular access for drugs, fluid and blood administration, parenteral feeding, central venous pressure monitoring, as well as haemodialysis vascular access for dialysis requiring patients with stage 3 acute kidney injury (AKI) or ESKD. Dialysis is key to the survival of ESKD patients until kidney transplant can be done. It is also life-saving in patients with AKI who meet indications for it.
Among haemodialysis challenges, vascular access creation still stands out. Although permanent access in the form of AVF is the preferred access route for haemodialysis, it is often not available at the time of dialysis initiation especially in resource poor settings like ours where late or emergency presentation is the norm. Even when patients present early and haemodialysis initiation is planned, out- of-pocket payment remains a stumbling block for such patients to pay for and get permanent vascular access. It also precludes dialysis initiation as planned. Hence temporary vascular access most commonly via catheterization of the femoral vein is done for such patients. This was the case in this index patient.
Although femoral vein catheterization is often considered to be a relatively safe procedure [1, 2], the following complications have been observed: haemorrhage, femoral artery puncture, femoral nerve injury, pseudoaneurysm, fistula formation, thrombophlebitis, retroperitoneal hemorrhage, bowel perforation, urinary bladder puncture, infections and migration of guidewire. Despite being a rare complication of central vein cannulation, some cases of guidewire migration or loss have been reported [3, 4, 5, 6, 7, 8].
Guidewire- related complications with or without migration include: arrhythmias and other conduction abnormalities, thrombosis, vessel or myocardial perforation with subsequent haemothorax or cardiac tamponade and circulatory collapse, guidewire kinking, breakage and subsequent embolization. Guidewire migration is associated with mortality in up to 20% of cases [2, 9]. Although the index patient did not experience arrhythmia or any complication as at the time of guidewire extraction, his RIJV was significantly thrombotic. Any of the fatal complications of migrated guidewire would likely have occurred if patient did not enroll in our WKD free RIJV catheter insertion which led to the discovery of the migrated guidewire and the subsequent surgical intervention.
Migrated guidewire may be asymptomatic or may cause difficulty in drawing blood or injecting drugs into the affected blood vessel, reduced venous backflow from distal lumen or may be only seen in x-rays [3, 10, 11]. In this case, although the exact day the guidewire migrated could not be conclusively ascertained, Mr. OC did report a particularly difficult and bloody right femoral vein cannulation and subsequent unsuccessful right femoral vein catheterization. These signs implied obstruction of the femoral vein lumen by the migrated guidewire. Furthermore, although we were able to effortlessly cannulate his RIJV, guidewire advancement was impossible. It is true that he reported no palpitation and the only ECG done demonstrated no arrhythmia, guidewire-related arrhythmias are often momentary and unobserved.9 Hence can easily be missed by a single ECG (Figure 1).
Migrated guidewire from femoral vein cannulation can be retrieved from the groin by interventional percutaneous procedure. In this case report, the x-ray showed the migrated guidewire could not be approached through the groin as its distal tip had migrated deep into the true pelvis while the proximal inverted “J” tip was easily accessible from the RIJV through the right anterior neck angle. The best method for retrieval of migrated guidewire is by interventional means using vascular snares or forceps but when this fails, open surgical approach is done [2, 12]. The index patient underwent open surgical retrieval of the migrated guidewire due to the absence of facility for interventional vascular procedures in our institution.
Causes of guidewire migration include distractions, poor skills, naivety and/or fatigue of the medical personnel doing the procedure as well as lack of trainee supervision [4]. Although many central catheters have been inserted by nurses in the United States, these nurses are well trained and operate under ultrasound guidance [13]. Mr. OC was unfortunately getting haemodialysis in a private dialysis centre where catheterization is done by unqualified health personnel (a non-renal nurse and a dialysis technician). Worse still, they do not operate with ultrasound guidance which is known to reduce the risk of complications [14, 15]. Little wonder that such a complication could go unreported and hence without any intervention. Thus, the need for this life-saving procedure to be carried out by well trained professionals cannot be overemphasized.
Guidewire migration can be prevented through adequate training and supervision of trainees. Central vein cannulation and catheter placement should only be done by qualified and appropriately trained medical personnel. Deep push of the guidewire should be avoided and throughout the duration of the procedure including the time when catheter is being inserted over the guidewire, a good length of the guidewire must always be preferably hand-held or anchored unto a drape. A checklist should be used to assess the contents of the procedure tray after catheter placement. By so doing, a missing guidewire can be detected early with prompt removal averting complications.
Furthermore, post- catheter placement check-x-ray can also help in early detection of catheter insertion-related complications including migrated guidewire.
Signs of migrated guidewire with partial occlusion of vascular lumen including reduced backward blood flow from the vein, difficulty in injection into the vessel as well as difficulty in subsequent cannulation of the vessel as seen in the index case are signs should not be ignored but should prompt investigation. In the case being reported, difficulty in right femoral vein cannulation rather than prompt investigation led to the abandonment of right femoral vein cannulation and preferential cannulation of left femoral vein for subsequent dialysis sessions.
If all precautions are taken and guidewire still accidentally migrates, this should be reported for prompt extraction to be achieved. If migrated guidewire is left, infections, thrombosis, arrhythmias, vascular damage and other complications can occur [16]. Mr. OC in our report was completely asymptomatic in line with the observation of Ruesch, et al. [17] (Figure 2).
Conclusion
Migration of guidewire is a rare complication of central vein catheterization but every precaution should be taken to prevent its occurrence. If it does occur, prompt intervention and extraction should be done.
References
-
Seldinger SI (1953) Catheter replacement of the needle in percutaneous arteriography; a new technique. Acta Radiologica 39(5): 368-376.
-
Okyere I, Takyi CA, Adabie JA, Okyere P, Boateng NA (2019) Accidental guidewire migration following emergency femoral central venous catheterization. The Pan African Medical Journal 33: 259.
-
Guo H, Peng F, Ueda T (2006) Loss of the guide wire: a case report. Circ J 70(11): 1520-1522.
-
Schummer W, Schummer C, Gaser E, Bartunek R (2002) Loss of the guide wire: mishap or blunder? Br J Anaesth 88(1): 144-146.
-
Gordon PC, Linton DM (1992) The missing wire: a complication of central venous catheterization. Anaesth Intensive Care 20(1): 77-79.
-
Batra RK, Guleria S, Mandal S (2002) Unusual complication of internal jugular vein cannulation. Indian J Chest Dis Allied Sci 44(2): 137-139.
-
Auweiler M, Kampe S, Zähringer M, Buzello S, Spiegel TV, et al. (2005) The human error: delayed diagnosis of intravascular loss of guidewires for central venous catheterization. J Clin Anesth 17(7): 562-564.
-
Huang CC, Chan CM, Chen H, Chen WL, Wu YL (2008) Emergency femoral central venous catheterization in an elderly patient complicated by distal guidewire migration. International Journal of Gerontology 2(3): 133-135.
-
Khasawneh FA, Smalligan RD (2011) Guidewire- Related Complications during Central Venous Catheter Placement: A Case Report and Review of the Literature. Case Reports in Critical Care Volume 2011: 287261.
-
Polos PG, Sahn SA (1991) Complications of central venous catheter insertion: fragmentation of a guidewire with pulmonary artery embolism. Crit Care Med 19(3): 438-440.
-
Andrews RT, Bova DA, Venbrux AC (2000) How much guidewire is too much? Direct measurement of the distance from subclavian and internal jugular vein access sites to the superior vena cava-atrial junction during central venous catheter placement. Crit Care Med 28(1): 138-142.
-
Omar H, Fatthy A, Mangar D, Camporesi E (2010) Missing the guidewire: an avoidable complication. Int Arch Med 3: 21.
-
(2013) AIUM practice guideline for the use of ultrasound to guide vascular access procedures. J Ultrasound Med 32(1): 191-215.
-
Grebenik CR, Boyce A, Sinclair ME, Evans RD, Mason DG, et al. (2004) NICE guidelines for central venous catheterization in children. Is the evidence base sufficient? Br J Anaesth 92(6): 827-830.
-
Stokowski G, Steele D, Wilson D (2009) The use of ultrasound to improve practice and reduce complication rates in peripherally inserted central catheter insertions: Final report of investigation. J Infus Nurs 32(3): 145-155.
-
Tong M, Siu Y, Ng Y, Kwan T, Au T (2004) Misplacement of a right internal jugular vein haemodialysis catheter into the mediastinum. Hong Kong Med J 10(2): 135-138.
-
Ruesch S, Walder B, Tramèr MR (2002) Complications of central venous catheters: internal jugular versus subclavian access: a systematic review. Crit Care Med 30(2): 454-460.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report