Meningoencephalomyelitis of Unknown Etiology: Short-Term Effect of Two Treatment Protocols on Cerebrospinal Fluid
Background: The early disease course of meningoencephalomyelitis of unknown etiology (MUE) is particularly vulnerable. Cerebrospinal fluid is a sensitive indicator of inflammatory disease and can be used for diagnosis and monitoring disease response to treatment. Objective: Compare the effects of glucocorticoids alone versus glucocorticoids and cytarabine on cerebrospinal fluid (CSF) analysis in dogs within 72 hours of diagnosis with MUE. Method: CSF was collected from 10 dogs diagnosed with MUE. Six dogs were administered immunosuppressive glucocorticoids, and four dogs were administered immunosuppressive glucocorticoids and a 300 mg/m² cytarabine CRI over 24 hours. Repeat CSF analyses were performed 69-72 hours after the first administration of Dex SP IV. Results: The median nucleated cell count (NCC) and total protein (TP) levels decreased in both therapy groups. There was no statistical difference in CSF analysis between the two treatment groups after therapy. Conclusion: Seventy-two hours after MUE diagnosis and treatment, the reduction in NCC and TP between initial and repeat CSF analysis was decreased and there was no significant difference in NCC or TP reduction between treatment groups.
Mancini SL¹, Early PJ¹*, Olby NJ¹, Mariani CL¹, Munana KR¹, Bray KY² and Bergman BL²
¹NC State University Veterinary Hospital, William Moore Drive, USA ²Carolina Veterinary Specialists, Winston Salem, USA *Corresponding author: Peter Early J, NC State University Veterinary Hospital, William Moore Drive, Raleigh, NC 27606, USA, Tel: +1 (919) 513-6692; Fax: 1 (919) 513-6784; Email: pjearly@ ncsu.edu Keywords: Dog; Meningoencephalomyelitis; Cytarabine; Dexamethasone SP; Cerebrospinal Fluid
Abbreviations
CNS: Central Nervous System; MUE: Meningoencephalomyelitis of Unknown Etiology; CSF: Cerebrospinal Fluid; GME: Granulomatous Meningoencephalomyelitis; NCC: Nucleated Cell Count; TP: Total Protein; MRI: Magnetic Resonance Imaging.
Introduction
Inflammatory central nervous system (CNS) diseases are a critical concern in clinical veterinary neurology. Meningoencephalomyelitis of unknown etiology (MUE) is a collective term describing CNS inflammation with an undetermined cause, encompassing conditions such as granulomatous meningoencephalomyelitis (GME) and the necrotizing encephalitides (NE), such as necrotizing meningoencephalitis (NME) and necrotizing leukoencephalitis (NLE) [1]. The inability to specifically identify the pathogenesis of MUE and the disease’s inherent heterogeneity complicate the development of an optimal, standardized treatment protocol.
Diagnosis of MUE primarily relies on advanced imaging techniques, particularly magnetic resonance imaging (MRI) and cerebrospinal fluid (CSF) analysis. Typically, dogs with MUE present with focal or multifocal areas of T2 hyperintensity on MRI and a mononuclear pleocytosis along with elevated protein concentration in the CSF [1, 2]. Negative infectious disease testing further supports a diagnosis of MUE.
In addition to its diagnostic value, CSF analysis is essential for monitoring the disease. Studies have shown that changes in CSF can provide insights into multiple sclerosis outcomes when comparing diagnostic and monitoring tools [3]. Furthermore, a study by Lamb R, et al. [4] suggested that CSF is a more sensitive indicator of inflammatory disease than MRI.
Glucocorticoids are a mainstay of therapy for cases of MUE, given evidence suggesting it is an immune-mediated condition [5, 6]. Adjunctive immunosuppressive agents are often added to achieve longer survival times and better outcomes. One commonly used adjunct immunosuppressive agent is cytarabine, a nucleoside analogue that crosses the blood-brain barrier and competitively incorporates into the nucleic acid of mitotically active cells to act as an anti- metabolite [7, 8]. Various therapeutic protocols have been developed to improve survival times. Survival past the first three months has been associated with an increase in overall survival time [3, 9, 10].
There is also a subset of cases that acutely succumb to MUE early in the course of the disease. Some studies have shown mortality rates as high as 25% to 50% within the first two weeks [11, 12]. Although overall survival time is of critical interest, further investigation into the nature of MUE early in the disease course is warranted, as this is a particularly vulnerable period. Studies of this nature are needed to help guide the use of glucocorticoid and cytarabine therapy in treating MUE and further optimize the treatment of dogs with MUE.
This study aimed to compare the effects of glucocorticoids alone versus combination therapy involving glucocorticoids and cytarabine on CSF analysis early in the course of disease in dogs with MUE. We hypothesize that both treatments will decrease the nucleated cell count (NCC) and total protein (TP) of the CSF after 72 hours, with combination therapy yielding a more significant decrease than monotherapy.
Materials and Methods
Ten dogs were enrolled in the study between August 2019 and October 2020. Six dogs were enrolled through the NC State University Veterinary Hospital (NCSU), and the other four were enrolled through Carolina Veterinary Specialists (CVS). All dogs underwent MRI using a GE Signa 1.5T 16X (CVS) or 3.0T Siemens Skyra (NCSU) magnet, followed by cisternal or lumbar CSF analysis. The inclusion criteria specified that CSF must have an NCC greater than 50 cells/ µL, with more than 50% mononuclear cells on cytological evaluation. These cytologic inclusion criteria were based on the guidelines from the review by Granger N, et al. [2]. These criteria have been used in several other MUE studies [3, 9, 12]. Dogs were excluded if they had received glucocorticoids within 36 hours of the MRI and CSF collection. Dogs were excluded if the CSF had a red blood cell (RBC) count >1500 cells/µl or if immature white blood cells were present.
The six dogs in the monotherapy group from NCSU were administered Dexamethasone sodium phosphate (Dex SP) IV at a dose of 0.3 mg/kg immediately after CSF collection. All these dogs also received a second dose of Dex SP IV 0.3mg/kg the following morning. After that, three of the dogs continued to receive daily Dex SP IV at a dose of 0.3mg/kg for the remainder of the study, while the other three dogs received prednisone 2mg/kg/day orally for the next two days before the repeat CSF analysis. In the combination therapy group, all dogs started initially with Dex SP IV at a dose of 0.3 mg/kg. The following morning, all dogs received a second dose of Dex SP IV at a dose of 0.3mg/kg. After that, two dogs continued on Dex SP IV at 0.3 mg/kg during their hospital stay, while the other two dogs switched to oral prednisone 2 mg/kg/day for two days until the repeat CSF analysis. Selection of the corticosteroid formulation was made with careful consideration of the patient’s clinical status and their ability to ingest oral medication.
Repeat CSF samples were collected 69-72 hours after starting glucocorticoids, with repeat samples taken from the same site as the initial collection. In the monotherapy group, 4 dogs had cisternal samples and 2 had lumbar samples. In the combination therapy group, 3 dogs had cisternal samples, and 1 had a lumbar sample. The collection site was based on the localization of clinical signs.
Neurologic exam findings were recorded on the morning of each CSF collection. Clinical progression was also characterized on the morning of the repeat CSF collection as resolved, improved, static, or deteriorated.
Evaluation of NCC and TP value changes within each group was performed with a nonparametric Wilcoxon signed rank test to determine whether there had been statistically significant changes between pre- and post-treatment. Comparison of the changes experienced between the two groups was performed using the nonparametric exact Mann- Whitney U test.
Results
The study population consisted of three Chihuahuas, three Malteses, one Pug, one Poodle, one Shih Tzu, and one Golden Retriever, ranging in age from 14 months to 102 months. Six were male castrated, 2 were female spayed, and 2 were female intact.
The monotherapy group showed a median NCC and TP of 201 cells/μL and 45.95 mg/dL, respectively, in the initial CSF analyses (Table 1). The median percentage of the mononuclear component of the initial CSF analyses was 93% (16.5% large mononuclear cells and 76.5% small mononuclear cells) (Table 1).
When a repeat spinal fluid sample was collected in the monotherapy group, the results showed that the median NCC and TP of the repeat CSF analyses were 49.5 cells/uL and 33.95 mg/dL, respectively (Table 1). The median percentage of the mononuclear component of the repeat CSF analyses in the monotherapy group was 97.5% (10% large mononuclear cells and 87.5% small mononuclear cells) (Table 1).
| Variable | Monotherapy median value (min, max) | Combination Therapy median value (min, max) |
|---|---|---|
| Total nucleated cell count – corrected (cells/uL) | ||
| Pre-treatment | 201 (79,1334) | 548.5 (312,1166) |
| Post-treatment | 49.5 (10,648) | 179.5 (50,388) |
| Large mononuclear cells (%) | ||
| Pre-treatment | 16.5 (2,77) | 16.5 (4,35) |
| Post-treatment | 10 (0,52) | 11.5 (3,27) |
| Small mononuclear cells (%) | ||
| Pre-treatment | 76.5 (15,97) | 68 (62,78) |
| Post-treatment | 87.5 (13,99) | 81.5 (63,93) |
| Total Protein (mg/dL) | ||
| Pre-treatment | 45.95 (19.2,346) | 193.1 (111.1, 382) |
| Post-treatment | 33.95 (18.6,51.3) | 132.7 (48.4,283) |
Table 1: Summary Statistics for Total Nucleated Cell Count, Percent Mononuclear Cell Types, and Total Protein, All Observations.
In the combination therapy group, the median NCC and TP of the initial CSF analyses was 548.8 cells/uL and 193.1 mg/dL, respectively (Table 1). The median percentage of the mononuclear component of the initial CSF analyses was 84.5% (16.5% large mononuclear cells and 68% small mononuclear cells) for dogs treated with combination therapy (Table 2). When a repeat spinal fluid sample was collected in the combination therapy group, the median NCC and TP of the repeat CSF analyses were 179.5 cells/uL and 132.7 mg/dL, respectively (Table 1). The median percentage of the mononuclear component of the repeat CSF analyses in the combination therapy group was 93% (11.5% large mononuclear cells and 81.5% small mononuclear cells) (Table 2).
| Variable | Treatment Group | Z-value | P-value |
|---|---|---|---|
| Total Nucleated cell count – corrected, change in | Monotherapy group | -1.36 | 0.173 |
| Combination Therapy group | -1.83 | 0.068 | |
| Total Protein, change in | Monotherapy group | -1.36 | 0.173 |
| Combination Therapy group | -1.46 | 0.144 |
Table 2: Results of Mann-Whitney U Tests for Changes in Cerebrospinal Fluids Analysis, Total Nucleated Cell Count, and Total Prot
The median NCC was four times lower for the repeat CSF analysis than for the initial CSF analysis in the monotherapy group and three times lower for the repeat CSF analysis than for the initial CSF analysis in the combination therapy group (Figure 1).
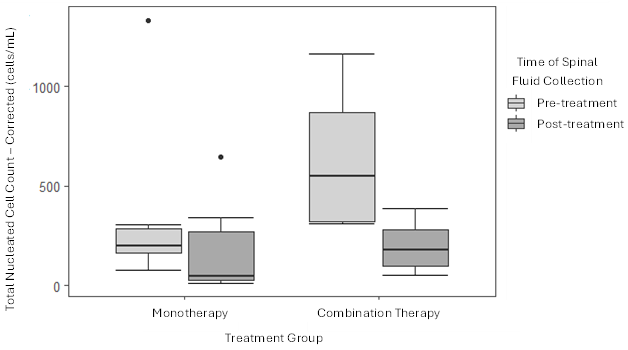
Although both groups saw decreases in median nucleated cell count (NCC) and total protein (TP) within 72 hours of treatment, these changes weren’t statistically significant when comparing the two therapy groups (Table 2). There was one outlier in the monotherapy group. The outlier demonstrated an NCC increase of 334% and a 135% increase in TP on repeat analysis. This patient was euthanized approximately 4.5 months after being diagnosed with diabetic ketoacidosis and pancreatitis. Necropsy definitively diagnosed mild multifocal lymphoplasmacytic meningoencephalomyelitis.
Discussion
The purpose of this study was to evaluate and compare the effects of administering glucocorticoids alone versus glucocorticoids in combination with cytarabine on CSF analysis in dogs with MUE within the first 72 hours of diagnosis and treatment. The overall goal was to provide data to guide the future use of these treatments and optimize care for MUE patients.
Ideally, MRI and CSF analysis are used together for a comprehensive evaluation of inflammatory diseases; however, CSF analysis alone is a relatively simple, reliable, and inexpensive assessment that provides substantial value [3, 4]. Also, when investigating MRI in dogs with and without inflammatory CSF, Lamb R, et al. [4] found MRI abnormalities in only 76% of cases with inflammatory CSF, which suggests CSF may be a more sensitive test for intracranial inflammatory disease than MRI.
Although histopathology is the definitive diagnostic tool, this study’s inclusion criteria prioritized utilizing CSF analysis as a reliable test in MUE cases.
In an earlier study, Mercier and Heller repeated CSF analysis approximately 30 days after diagnosis and initiation of glucocorticoid monotherapy in sixteen dogs diagnosed with MUE. All dogs in the study were treated with intravenous methylprednisolone at a dose of 30 mg/kg IV, followed by 15 mg/kg IV three hours after the initial dose and 10 mg/kg IV three hours after the second dose. The administration of immunosuppressive doses of prednisone or prednisolone followed this treatment. All 16 dogs had a repeat CSF analysis one month after diagnosis [13]. Dogs were classified as responders or non-responders based on the normalization of their CSF analysis, or the lack thereof, respectively. Seven of 16 dogs, or 43.8%, responded to glucocorticoid monotherapy [13].
Additionally, only one of the seven responders had a clinical relapse when follow-up information was obtained within the first 48 months. Three of the non-responders were started on cytarabine, and two of the non-responders were euthanized for progressive signs. Given that only one of the responders showed signs of a relapse, normalization of CSF after one month of treatment might be associated with a lower chance of relapse [13].
Lowrie M, et al. [3] also described the predictive values of repeat CSF analysis regarding the outcomes of MUE. Lowrie M, et al. [3] diagnosed 39 dogs with MUE and investigated prognostic factors and outcomes. CSF analysis was repeated in 17 dogs three months after diagnosis and initiation of treatment, which consisted of immunosuppressive prednisone or prednisolone, accompanied by subcutaneous (SC) cytarabine administered as an initial 50 mg/m² dose every 12 hours for 48 hours, and repeated every 3 weeks. All dogs had partial or complete resolution of clinical signs. However, 7/17 dogs had an inflammatory CSF at three months, and upon long-term follow-up, 11/17 dogs had a relapse [3]. While an unremarkable CSF analysis at the three- month re-examination was not associated with the outcome, an abnormal repeat CSF analysis after three months was predictive of relapse [3].
Utilizing some of the same cases as the 2013 study, Lowrie et al. also compared the survival rate of 39 dogs treated with immunosuppressive prednisone and an initial dose of 50 mg/m2 SC cytarabine every 12 hours for 48 hours with the survival rate of 41 dogs treated with immunosuppressive prednisone and an initial dose of 100 mg/m2 cytarabine constant rate infusion administered over 24 hours [10]. Every three weeks, all dogs received subsequent doses of subcutaneous cytarabine as previously described. Seventeen of 39 dogs that received SC cytarabine and 37 of 41 dogs that received a cytarabine CRI survived three months and had a repeat CSF analysis [10]. Seven of the 17 surviving dogs that received SC cytarabine had an abnormal second CSF analysis compared with only one of the 37 surviving dogs that received their initial cytarabine treatment by CRI [10]. There was a statistically significant increase in the rate of CSF normalization for dogs treated with a CRI compared to dogs treated with SC injections, with rates of 97.3% and 58.8%, respectively [10]. Additionally, the long-term (>12 months) survival rates for dogs treated with a CRI were significantly higher than those treated with SC injections, also suggesting an association between the results of repeat CSF analysis and outcome.
The findings in these studies provided important background for our research but did not focus on the same timeframe of the disease course. Granger N, et al. [2] only repeated the analysis one month after treatment, which does not capture many vulnerable cases that succumb to the disease sooner. Cornelis I, et al. [12] indicated that over 25% of MUE cases died within one week of diagnosis (2016). Furthermore, regarding the dogs in the 2013 and 2016 Lowrie et al studies treated with SC cytarabine, 13/39 (33%) died within three days, and the median survival time was 26 days. Also, 56% and 10% of the dogs treated with SC cytarabine and a cytarabine CRI, respectively, died within the first three months before a repeat CSF analysis [3]. While these studies provided information on serial CSF analysis and demonstrated that CSF findings carry predictive value for cases of MUE, it is still unclear why some cases did not survive the early course of MUE. Additionally, when Lowrie M, et al. [10] demonstrated an increased survival rate in cases treated with a cytarabine continuous infusion (CRI) over cases treated with subcutaneous (SC) cytarabine, the only difference between the groups was the treatment administered immediately after initial diagnostics (2016). The initial treatment with cytarabine CRI suggests that survival depends on short-term disease progression. Therefore, understanding the early stages of disease progression and the response to therapy is vital.
Our study investigated the effects of treatment on CSF analysis findings 69-72 hours after diagnosis, providing insight into the early stages of the disease. Our results indicated improvement in CSF NCC and TP within the first 72 hours of treatment in five of the six cases administered monotherapy and in all four cases administered combination therapy. There was no statistically significant difference in the amount by which the values decreased or the values between treatment groups. The monotherapy group had a four-fold decrease in NCC, and the combination therapy group had a three-fold decrease in NCC. However, it’s worth noting that the combination therapy group initially started with substantially higher NCC and TP levels, which may have contributed to the apparent difference in the magnitude of decrease compared to the monotherapy group.
The repeat CSF analysis results for one patient in our study were particularly unexpected and discordant with the clinical response. This patient demonstrated an NCC increase of 434% and a TP increase of 236% between CSF analysis, but the patient’s clinical signs of spinal pain were ultimately resolved after 72 hours of treatment. The reason for the discordance between the clinical improvement and the increase in NCC in the repeat CSF analysis of the patient is uncertain. Possible explanations were hypothesized. The clinical improvement in this case may have been indicative of resolving edema, rather than a change in the NCC level of the CSF. The initial phase of inflammation is characterized by edema, which results from increased blood flow and vascular permeability. This is followed by cellular recruitment. The cellular component of both inflammation and its resolution occurs later than the appearance and resolution of edema [14]. Therefore, the individual inflammatory response of this dog may have created a timeline in that the edema was resolving at the time of the repeat CSF analysis, but cellular recruitment was still increasing or had not yet decreased to the level previously indicated by the initial study.
Therefore, this dog may have improved clinically in response to the resolving edema while the NCC in the CSF increased. Another possible explanation may exist in the effect that glucocorticoids have on white blood cells. Once white blood cells infiltrate a tissue of recruitment, they differentiate into a proinflammatory state [15]. The glucocorticoids target these differentiated proinflammatory cells and cause them to revert to a tolerogenic cell that produces anti-inflammatory cytokines [15]. This alters the environment and the overall inflammatory response [15]. However, it does not entirely negate the initial recruitment of inflammatory cells. Therefore, it may be possible that the repeated CSF analysis in this patient was collected when the NCC was still increasing. Still, the effects of the glucocorticoids may have reduced the overall inflammatory nature within the CSF, resulting in an improved clinical status. A combination of these theories or a novel explanation is also possible. Following cases like this further into the future may provide additional insight into long-term outcomes.
One of this study’s primary limitations was its small sample size. The lack of statistically significant results may be due to the small sample size, and a more extensive study may reveal differences in these outcomes between initial and repeat CSF analyses, as well as between treatment groups. Another limitation of the study was the absence of a control group, as withholding treatment may be considered unethical. The monotherapy group served as a comparison group, but a crossover study design was not feasible due to the nature of the disease. Additionally, treatment group segregation by location may have introduced confounding variables due to differences in laboratory and hospital protocols. Future studies with larger sample sizes and repeated CSF analysis could help evaluate treatment efficacy and associations between CSF changes and survival rates, optimizing treatment and improving outcomes for canine MUE cases.
Conclusion
In our study, we investigated the effects of glucocorticoids alone and in combination with cytarabine on CSF analysis in dogs with MUE. Both treatment groups exhibited considerable decreases in median nucleated cell count (NCC) and total protein (TP) within 72 hours; however, the differences between the groups were not statistically significant.
Acknowledgement
The CREATE Fund and the Department of Clinical Sciences at NC State University College of Veterinary Medicine provided financial support.
Conflict of Interest
The authors declare that there is no conflict of interest related to this study.
References
-
Coates J, Jeffrey N (2014) Perspectives on meningoencephalomyelitis of unknown origin. Vet Clin North Am Small Anim Pract 44(6): 1157-85.
-
Granger N, Smith PM, Jeffery ND (2010) Clinical findings and treatment of non-infectious meningoencephalomyelitis in dogs: a systematic review of 457 published cases from 1962 to 2008. Vet J 184(3): 290-297.
-
Lowrie M, Smith PM, Garosi L (2013) Meningoencephalitis of unknown origin: investigation of prognostic factors and outcome using a standard treatment protocol. Vet Rec 172(20): 527.
-
Lamb R, Croson P, Cappello G, Cherubini B (2005) Magnetic resonance imaging findings in 25 dogs with inflammatory cerebrospinal fluid. Vet Radiol Ultrasound 46(1): 17-22.
-
Kipar A, Baumgärtner W, Vogl C, Gaedke K, Wellman M (1998) Immunohistochemical characterization of inflammatory cells in brains of dogs with granulomatous meningoencephalitis. Vet Pathol 35(1): 43-52.
-
Matsuki N, Fujiwara K, Tamahara S, Uchida K, Matsunaga H, et al. (2004) Prevalence of Autoantibody in Cerebrospinal Fluids from Dogs with Various CNS Diseases. J Vet Med Sci 66(3): 295-297.
-
Chabner BA, Myers CE, Coleman CN, Johns DG (1975) The Clinical Pharmacology of Antineoplastic Agents. N Engl J Med 292: 1107-1113.
-
Moncrieff JC, Chan TC, Samuels ML, Cook JR, Coppoc GL, et al. (1991) Plasma and cerebrospinal fluid pharmacokinetics of cytosine arabinoside in dogs. Cancer Chemother Pharmacol 29(1): 13-18.
-
Smith PM, Stalin CE, Shaw D, Granger N, Jeffery ND (2009) Comparison of two regimens for the treatment of meningoencephalomyelitis of unknown etiology. J Vet Intern Med 23: 520-526.
-
Lowrie M, Thomson S, Smith P, Garosi L (2016) Effect of a constant rate infusion of cytosine arabinoside on mortality in dogs with meningoencephalitis of unknown etiology. Vet J 213: 1-5.
-
Muñana KR, Luttgen PJ (1998) Prognostic factors for dogs with granulomatous meningoencephalomyelitis: 42 cases (1982-1996). J Am Vet Med Assoc 212(12): 1902-1906.
-
Cornelis I, Volk HA, Van Ham L, De Decker S (2016) Prognostic factors for 1-week survival in dogs diagnosed with meningoencephalitis of unknown aetiology. Vet J 214: 91-95.
-
Mercier M, Heller HL (2015) Efficacy of glucocorticoid monotherapy for treatment of canine meningoencephalomyelitis of unknown etiology: a prospective study in 16 dogs. Vet Med Sci 1(1): 16-22.
-
Sansbury BE, Spite M (2016) Resolution of Acute Inflammation and the Role of Resolvins in Immunity, Thrombosis, and Vascular Biology. Circ Res 119(1): 113- 30.
-
Dubois-Camacho K, Ottum PA, Franco-Muñoz D, De la Fuente M, Torres-Riquelme A, et al. (2017) Glucocorticosteroid therapy in inflammatory bowel diseases: From clinical practice to molecular biology. World J Gastroenterol 23(36): 6628-6638.
- The Digital Stethoscope: Harnessing AI in Veterinary Medicine Without Losing Our Healing Touch
- Safety and Efficacy of the HomeoPet Cough in Domestic Pets –A Clinical and Correction Analysis Based Upon User Response Survey
- Non Human Animals Responses to Social Loss
- Owner Reported Clinical Outcomes of a Homeopathic Proprietary Preparation for the Treatment of Upper Respiratory and Nasal Disorders in Companion Animals
- Effects and Diagnostic Approach of Ultrasound in Veterinary Practice: A Systematic Review
- Everything about Nutritional Value of the Meat Ingredients and How we can Reduce its Microbial Hazards