Multi-Drug Resistance Patterns of Wound Causing Bacterial Infections in a Rural Hospital, Sirajganj, Bangladesh
Wound infection is considered as one of the most common nosocomial infections in the world. The aim of this study is profiling of bacterial pathogenic isolates from wound infected patients who were admitted to the hospital and commonly to measure antimicrobial susceptibility profiling. An entire of 58 samples were collected for the study. The cultural analysis was done by phenotypic examination, and we performed Gram staining and biochemical examination for identification. The pus and wound swabs were collected aseptically and gold standard microbiological cultural analysis was performed in AlHera General Hospital, Sirajganj, Bangladesh between September 2020 and August 2021. 43(74.1%) of the whole samples yielded positive cultures and only 15(25.9%) samples showed negative growth. Gram-Negative bacteria showed more prevalence than Gram-Positive bacteria which were in number 32 and 11 respectively and in at 74.4% and 25.6%. The most predominant isolate was Escherichia coli 18 (41.9%) and second most was Staphylococcus aureus 12(27.9%), and the rest of other bacterial isolates were Pseudomonas aeruginosa was 5(11.6%), Proteus mirabilis 3(7.0%), Serratia marcescens 2(4.7%), Staphylococcus Saprophyticus 2(4.7%) and Klebsiella pneumoniae 1(2.3%). The isolates were resistant to the commonly used oral antibiotics, namely Azithromycin, Amoxicilin, Ceftriaxone, Ceftazidime, Chloramphenicol, Cefixime, Amoxyclav, Colistin, Cefuroxime, Cloxacillin, Ciprofloxacin, Imipenem, Levofloxacilin, Vancomycin, Linezolid, Meropenem, Erythromycin, Gentamycin, Cephradine, Cotrimoxazole, Moxifloxacin which is very alarming. The pathogens showed remarkable sensitivity against Gentamicin and Meropenem, which at least leaves a window to get treated. This study was performed to hunt out appropriate antibiotic/s for wound infections based on pathogens isolated from wounds of hospital admitted patients in Bangladesh and their antibiotic susceptibility profile against available and frequently prescribed antibiotics.
Introduction
Human skin and soft tissue infections (SSTI) are caused by microbial pathogens during or after injury, burn, and surgical procedures end in pus assembly, consisting of white to yellow fluid consisting of dead WBC, cellular debris, and necrotic tissue [1, 2]. Both aerobic and anaerobic bacteria are related to wound infections that typically occur during due to a hospital environment and find you with significant illness, prolonged hospitalization, and enormous economic implications [3]. The emergence of antibiotic resistance and its rapid spread is taken into account as a significant threat to overall public health worldwide. Over the past few decades, the multidrug-resistant Gram Negative Bacterial strains like Escherichia coli, Serratia marcescens, Proteus mirabilis, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Gram-positive methicillin-resistant Staphylococcus aureus, Staphylococcus saprophyticus (MRSA) were found related to pus infection under hospital settings because of widespread misinterpretation of antibiotics and inadequate dosage methods [4, 5]. Due to limited treatment options and the discovery of mild heat within the latest class of antibiotics, the emergence of multidrug-resistant bacteria has become a serious threat to global public health. The goal of the study is to isolate pathogenic bacteria from infected wound samples and to find out their susceptibility against different classes and generations of antibiotics.
Materials and Methods
Study Space
The study was conducted from September 2020 to August 2021. The samples were collected from Al-Hera General Hospital, Sirajganj, Bangladesh. The analysis part was completed in the department of Microbiology, Khwaja Yunus Ali University, Sirajganj, Bangladesh.
Sample Collection and Characterization
A total of 58 pus samples were collected using sterile syringes. (n=15) and by sterile swabs (n=43) from in -patient and outpatient departments of in several wards of Al-Hera General Hospital, Sirajganj, Bangladesh. Over a period of 11 months, the study was carried out by following the standard protocols and ethical guidelines. Pus samples were collected from the skin (furuncles, pustules, and abrasions), nasal lesions, ears, legs, internal organs (lungs, kidneys, and bladder), and catheters. Samples were aseptically inoculated with blood agar (5% sheep blood) and MacConkey agar plates, incubated aerobically at 350C-370C for 24-48 h. The isolation, detection and characterization, Gram staining, microscopic properties, colony properties and biochemical tests were performed using standard microbiological methods.
Antimicrobial Agents
Locally available antibiotic discs were used for antibiotic susceptibility test as per manufacturer’s instructions. namely amoxicillin (20μg), azithromycin (15μg), ceftriaxone (30μg), ceftazidime (30μg), cefuroxime (30μg), cefixime (5μg), ciprofloxacin (5μg), chloramphenicol (30μg), amoxyclav (30μg), colistin (10μg), erythromycin (15μg), cloxacillin (5μg), imipenem (10μg), levofloxacin (5μg), linezolid (30 μg), meropenem (10μg), gentamicin (10μg), cephradine (25μg), cotrimoxazole (25μg), moxifloxacin (5μg), and vancomycin (30μg).
Antibiotics Susceptibility Testing
Antibiotic susceptibility to bacterial isolates was identified with the strategy proposed by the Institute of Clinical and Laboratory Standards. As a summary, the inoculums were prepared for each bacterial isolate by adjusting the turbidity to the 0.5 McFarland standards and spreading it on the Muller-Hinton agar plate. The antibiotic disc (oxide antibiotic disc, UK) was placed on the agar plate and incubated overnight at 37°C for 24 hours. Restricted zones were measured and then the isolates were classified as sensitive, intermediate and resistant according to the CLSI table and guidelines [6].
Statistical Analysis
Statistical Package for Social Sciences (SPSS) Edition-16.0 and Microsoft Excel was used for analysis of the data. The share of frequencies was generated for various categorical variables like rate of isolation, sort of bacteria, pattern of antibiotic sensitivity categorized as resistant, intermediate and sensitive.
Results and Discussion
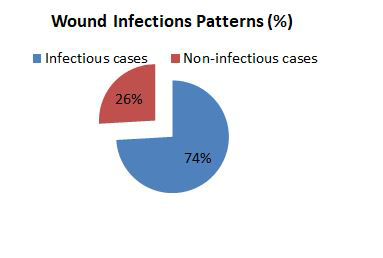
Out of 58 pus samples collected from different wards of the hospital, 43 samples (74.1%) showed bacterial growth within 24-48 hours after incubation at 37°C, whereas 15 samples (25.9%) showed negative growth on the cultured media that were considered as non-infectious (Figure 1).
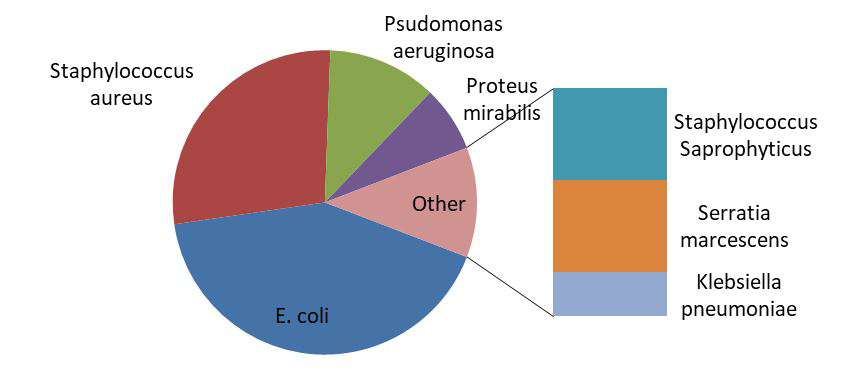
In this study, they cultured positive bacterial growths that were confirmed by Gram staining, and biochemical analysis. The eight bacterial strains of E. coli were the most frequent pathogens revealed as 41.9% of cases, followed by Staphylococcus aureus (27.9%), Klebsiella pneumoniae (2.3%), Serratia marcescens (4.7%), Staphylococcus saprophyticus (4.7%), Pseudomonas aeruginosa (11.6%), and Proteus mirabilis (7.0%) (Figure 2).
The majority of the wounds were infected with a single organism. Bacillus, a Gram negative bacterium, was found in 67.4% cases and 32.6% cases are linked with Gram positive, Cocci. Most of the isolated organisms were E. coli, 18 in number (41.9%) followed by Staphylococcus aureus 12(27.9%), Staphylococcus spp 2(4.7%). Other isolates included Pseudomonas aureginosa 5(11.6%), Proteus mirabilis 3(7.0%), Serratia marcescens 2(4.7%) and Klebsiella spp 1(2.3%) (Table 1).
| Isolation Group | Bacterial isolates | Total No. | Percentage |
|---|---|---|---|
| Gram Negative bacteria n=29(67.4%) | Escherichia coli | 18 | 41.9 |
| Proteus mirabilis | 3 | 7 | |
| Pseudomonas aeruginosa | 5 | 11.6 | |
| Serratia marcescens | 2 | 4.7 | |
| Klebsiella pneumoniae | 1 | 2.3 | |
| Gram Positive bacteria n=14(32.6%) | Staphylococcus aureus | 12 | 27.9 |
| Coagulase Negative Saprophyticus | 2 | 4.7 | |
| Total | 43 | 100 |
Table 1: Distribution pattern of Bacterial Isolates of wound infection (n=43).
High number of samples (15) were collected from patients age group 25-36 years and therefore the least i.e., 03 samples were obtained from the patients at the age group of
0-12 years. Among 43 positive cases, 23 (53.5%) were male and rest of 20 (46.5%) were female (Table 2) [7].
| Age group (Years) | Male | Female | Total | Percentage | ||
|---|---|---|---|---|---|---|
| No. of cases | % | No. of cases | % | No. of cases | (n=43) | |
| 0-12 | 3 | 100 | 0 | 0 | 3 | 7 |
| 13-24 | 6 | 50 | 6 | 50 | 12 | 27.9 |
| 25-36 | 6 | 40 | 9 | 60 | 15 | 34.9 |
| 37-49 | 4 | 66.7 | 2 | 33.3 | 6 | 37.2 |
| >50 | 4 | 57.1 | 3 | 42.9 | 7 | 16.3 |
| Total | 23 | 53.5 | 20 | 46.5 | 43 | 100 |
Table 2: Gender and age-wise distribution of wound infected patient (n=43).
The presence of Gram-negative bacteria (25.9%) was more significant in pus samples than gram-positive bacteria, on which many previous studies do agree. This study is associated with Zhang, et al. [8] where E. coli, S. aureus, K. pneumoniae and, P. aeruginosa were found responsible for infection from patients with severe intra-abdominal problem. In another experiment, S. aureus was identified as dominant bacterial species from wounds followed by P. aeruginosa, P. mirabilis, and E. coli [9] consistent that relate the results of with Dryden [10]. S. aureus and MRSA are the most explanations for soft tissue infections in hospitalized patients. Pseudomonas spp, Staphylococcus spp, Streptococcus spp, Klebsiella spp, and E. coli have also been reported in several other experiments [11, 12].
| Antibiotic | Bacterial Isolations, Number (N) with Percentage (%) | ||||||
|---|---|---|---|---|---|---|---|
| E. coli 18(41.9) | P.mirabilis 3 (7.0) | P.aeruginosa 5 (11.6) | S.arcescens 2(4.7) | S. aureus 12(27.9) | S. Saprophyticus 2(4.7) | K. pneumoniae 1 (2.3) | |
| Azithromycin | 8(44.5) | 3(100.0) | 5(100.0) | 1(50.0) | 4(33.3) | 0 (0.0) | 0 (0.0) |
| Amoxicilin | 3(16.7) | 3(100.0) | 3(60.0) | 0 (0.0) | 5(41.7) | 0 (0.0) | 0 (0.0) |
| Ceftriaxone | 9(50.0) | 1(33.3) | 3(60.0) | 0 (0.0) | 5(41.7) | 0 (0.0) | 1(100.0) |
| Ceftazidime | 14(77.8) | 1(33.3) | 0(0.0) | 0 (0.0) | 9(75.0) | 2(100.0) | 1(100.0) |
| Chloramphenicol | 2(11.1) | 2(66.7) | 4(80.0) | 1(50.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Cefixime | 18(100.0) | 1(33.3) | 0(0.0) | 0 (0.0) | 9(75.0) | 2(100.0) | 0 (0.0) |
| Amoxyclav | 2(11.1) | 0(0.0) | 1(20.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Colistin | 7(38.9) | 0(0.0) | 2(40.0) | 0 (0.0) | 4(3.3) | 2(100.0) | 1(100.0) |
| Cefuroxime | 12(66.7) | 3(100.0) | 2(40.0) | 1(50.0) | 6(50.0) | 0 (0.0) | 0 (0.0) |
| Cloxacillin | 13(72.2) | 2(66.7) | 2(40.0) | 0 (0.0) | 7(58.3) | 1(50.0) | 1(100.0) |
| Ciprofloxacin | 6(33.3) | 1(33.3) | 1(20.0) | 0 (0.0) | 3(25.0) | 0 (0.0) | 0 (0.0) |
| Imipenem | 2(11.1) | 0(0.0) | 0(0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Levofloxacilin | 6(33.3) | 1(33.3) | 1(20.0) | 1(50.0) | 6(50.0) | 0 (0.0) | 0 (0.0) |
| Vancomycin | 16(88.9) | 1(33.3) | 2(40.0) | 0 (0.0) | 3(25.0 | 0 (0.0) | 0 (0.0) |
| Linezolid | 15(83.3) | 1(33.3) | 1(20.0) | 0 (0.0) | 2(16.7) | 0 (0.0) | 0 (0.0) |
| Meropenem | 2(11.1) | 1(33.3) | 0(0.0) | 0 (0.0) | 1(8.3) | 0 (0.0) | 0 (0.0) |
| Erythromycin | 5(27.8) | 3(100.0) | 4(80.0) | 1(50.0) | 4(33.3) | 0 (0.0) | 0 (0.0) |
| Gentamycin | 1(5.6) | 1(33.3) | 1(20.0) | 0 (0.0) | 1(8.3) | 0 (0.0) | 0 (0.0) |
| Cephradine | 14(77.8) | 1(33.3) | 5(100.0) | 1(50.0) | 4(33.3) | 0 (0.0) | 0 (0.0) |
| Cotrimoxazole | 10(55.6) | 1(33.3) | 3(60.0) | 0 (0.0) | 6(50.0) | 0 (0.0) | 0 (0.0) |
| Moxifloxacin | 5(27.8) | 0(0.0) | 1(20.0) | 0 (0.0) | 1(8.3) | 0 (0.0) | 0 (0.0) |
Table 3: Antimicrobial Resistance Profiling of Bacterial Isolates.
Antibiotic susceptibility patterns of the bacterial isolates were shown in Table 3 that were determined by the standard disk diffusion method on Mueller-Hinton culture media. The bacteria E. coli 18(41.9%), was the most predominant isolates were found in our study that exhibited the highest resistance to Cefixime (100%), Vancomycin (88.9%) and Linezolid (83.3), while being least or moderate resistance to Ceftazidime (77.8%), Cefuroxime (66.7%), Cephradine (77.8%) and Cotrimoxazole (55.6%). In this study, E. coli was more sensitive to Cefixime, Vancomycin, Linezolid while being least sensitive to Azithromycin, Amoxicilin, Ceftriaxone, and Ceftazidime. It showed sensitivity to Gentamycin (5.6%), and 88.9% sensitive to 4th generation Meropenem and Imipenem, third-generation cephalosporins of Chloramphenicol; combination of Amoxicillin (Penicillin antibiotic) and Clavulanic acid (Beta-lactamase inhibitor) of Amoxyclav, and only 83.3% of Amoxicilin (Table 3). The second most dominant bacterial frequencies of Staphylococcus aureus 12(27.9) showed the highest resistance to antibiotics, namely Ceftazidime (75.0%) and Cefixime (75.0%), moderate resistance to Cefuroxime (50.0%) and Cloxacillin (58.3%). Chloramphenicol, Amoxyclav and Imipenem were proving to be the choice of antibiotics, reporting a 100% success rate.
Pseudomonas aeruginosa was in third position based on the predominant bacterial species in this study. P. aeruginosa showed complete resistance to Azithromycin (100%), Cephradine (100%) and was 80% resistant to Erythromycin. This species was proven as poorly resistant (20%) to Amoxyclav, Ciprofloxacin, Levofloxacilin, Linezolid, Gentamycin, and Moxifloxacin and 100% sensitive to Ceftazidime, Imipenem, Cefixime and Meropenem. Other species such as Proteus mirabilis 3 (7.0%), Serratia marcescens 2(4.7%), S. saprophyticus 2(4.7%), and Klebsiella pneumoniae 1(2.3%) showed 100% sensitive to Amoxyclav and Imipenem but except Meropenem that is being 66.7% sensitive to Proteus mirabilis. K. pneumoniae showed 100% resistance to Ceftriaxone, Ceftazidime, Colistin and Cloxacillin, and another bacterial strain of S. saprophyticus was 100 % resistant to Ceftazidime, Cefixime, Colistin, but Cloxacillin resistance was only 50%.
Conclusion
To rule out the individual bacterial species, either pathogenic or non-pathogenic, as well as to find out the best treatment option through susceptibility pattern of antibiotics; the study was conducted by collecting wound or pus swab from patients from a rural hospital vulnerable to possible bacterial infection. E.coli isolates showed highest incidence of infection, followed by S. aureus, P. aeruginosa, K. pneumoniae, S. Saprophyticus, Serratia marcescens, P. mirabilis, and Streptococcus app. Bacterial isolates exhibit high to moderate resistance to a spreading number of antibiotics. The sensitivity data of this report can also be considered when implementing empirical treatment strategies for pathogenic infections. At the same time, strict health policies should be applied to limit antibiotic use and to continuously monitor and report antibiotic resistance.
References
-
Cogen AL, Nizet V, Gallo RL (2008) Skin microbiota: a source of disease or defence? Br J Dermatol 158(3): 442- 455.
-
Scalise A, Bianchi A, Tartaglione C, Bolletta E, Pierangeli M, et al. (2015) Microenvironment and microbiology of skin wounds: the role of bacterial biofilms and related factors. Semin Vasc Surg 28(3-4): 151-159.
-
Bowler PG, Duerden BI, Armstrong DG (2001) Wound microbiology and associated approaches to wound management. Clin Microbiol Rev 14(2): 244-269.
-
Rice LB (2006) Antimicrobial resistance in gram-positive bacteria. Am J Med 119(6 suppl 1): S11-S19.
-
Iredell J, Brown J, Tagg K (2016) Antibiotic resistance in Enterobacteriaceae: mechanisms and clinical implications. BMJ 352: 19.
-
CLSI (2010) Performance standards for antimicrobial susceptibility testing. Twentieth informational supplement, Clinical and Laboratory Standards Institute.
-
Ahmed AA, Juyee NA, Hasan SMA, Abedin MZ (2020) Microbiological screening and antimicrobial sensitivity profiling of wound infections in a tertiary care hospital of Bangladesh. Eur J Med Health Sci 2(5): 101-106.
-
Zhang S, Ren L, Li Y, Wang J, Yu W (2014) Bacteriology and drug susceptibility analysis of pus from patients with severe intra-abdominal infection induced by abdominal trauma. Exp Ther Med 7(5): 1427-1431.
-
Bessa LJ, Fazii P, Giulio MDi, Cellini L (2015) Bacterial isolates from infected wounds and their antibiotic susceptibility pattern: some remarks about wound infection. Int Wound J 12(1): 47-52.
-
Dryden MS (2009) Skin and soft tissue infection: microbiology and epidemiology, Int J Antimicrob Agents 34(Suppl 1): S2-S7.
-
Misic AM, Gardner SE, Grice EA (2014) The Wound Microbiome: modern approaches to examining the role of microorganisms in impaired chronic wound healing. Adv Wound Care 3(7): 502-510.
-
Lockhart SR, Abramson MA, Beekmann SE (2007) Antimicrobial resistance among Gram-negative bacilli causing infections in intensive care unit patients in the United States between 1993 and 2004. J Clin Microbiol 45(10): 3352-3359.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines