Knowledge and Perceptions towards Act Use in the First Trimester of Pregnancy among Pregnant Women Attending ANC Clinic in Siaya County
Aim: We aim to assess and evaluate the knowledge and perception of pregnant women towards ACT use in the first trimester of pregnancy. Methods: The Study was conducted in Siaya County, Western Kenya from January 2019 to Dec 2019. Pregnant women who had attended ANC clinic in the two hospitals were recruited and semi-structured questionnaires were administered to them to obtain socio-demographic information and knowledge of ACT use in the first trimester of pregnancy. Results: Most participants 90%, knew at least one type of ACT (Artemether Lumefantrine), the most common malaria drug in the region, and could name at least two common malaria symptoms fever 92.3% and shivering 82.8%. Majority of the participants who stated that they had been exposed to malaria stated to have been prescribed AL for treatment and reported nausea 22.78% and dizziness 19.41% as the most common side effects experienced after consuming the drugs. There was low awareness of adverse pregnancy outcomes due to exposure to ACTs in the first trimester of pregnancy Conclusion: The most common ACT used for malaria treatment was AL. Most pregnant women had little knowledge about the effects of using an Artemisinin-based combination for malaria treatment in the first trimester of pregnancy. There is a need for more training for pregnant women, community health volunteers, and healthcare professionals on the proper use of ACT during pregnancy.
Background
Malaria remains one of the biggest public health challenges in sub-Saharan Africa. It has been a common disease and is still one of the most widely spread health hazards. According to World Health Organization (WHO)
estimates in 2019, there were about 228 million malaria cases in 87 regions malaria-endemic areas, which was a slight decline from 237 million in the previous year and estimated deaths of 409,000 [1]. It is also estimated that there was 12 million malaria infections during pregnancy in the high transmission regions of Africa. Children under 5 years account for more than 78% of all deaths [2]. Plasmodium falciparum is the deadliest species of plasmodium that causes malaria in humans. In pregnancy, it is associated with intrauterine growth restriction (IUGR), maternal anemia and low birth weight (LBW), stillbirth and preterm birth [3, 4, 5]. Low birth weight is caused by short gestation period, intrauterine growth restrictions or a combination of the two processes and leads to high infant mortality and morbidity globally [6].
Studying the risks and benefits of using the artemisinin- based combination in early pregnancy is crucial for policy formulation and individual treatment decisions. Malaria is common in pregnant women compared to their non- pregnant counterparts, more so in pregnant women who are HIV positive [7]. In high malaria transmission areas, asymptomatic malaria is more common in expectant women and has a statistically significant association with pregnant women’s hemoglobin levels [8, 9]. Due to the adverse effects of Malaria in Pregnancy, there is need to come up with an effective, safe and high-quality treatment method to reduce its prevalence rates. The WHO recommends using intermittent preventive treatment in pregnancy (IPTP), which involves administering a three tablets single dose of sulphadoxine- pyrimethamine (SP). ACT is currently recommended to treat uncomplicated Plasmodium falciparum malaria in pregnant women after the first trimester. Artemisinins are only recommended in the first trimester in the absence of quinine, which is recommended to treat malaria in the first trimester. However, Quinine is characterized a by low adherence due to its predominant side effects, such as the occurrence of hearing impairment, tinnitus, postural hypotension, and the number of doses required to complete treatment [10, 11].
Animal studies have shown that the use of artemisinins is embryotoxic and teratogenic [12]. During a sensitive organ development period, oral doses administered to rats resulted in embryo deaths and malformations [13]. ACT is highly available in high transmission malaria settings and is one of the most dispensed drugs in pharmacies. Pregnant women in this area are more likely to get exposed to ACTs in their first trimester of pregnancy since they may be unaware of their pregnancy status when seeking treatment, and the healthcare providers never ask; hence may not be aware of the pregnancy status of the woman when prescribing the drug [14, 15]. This study seeks to obtain knowledge and perception of ACT use in the first trimester of pregnancy among pregnant women who presented themselves to ANC clinics in Western Kenya. Also, we indent to determine at what point during pregnancy these women were exposed to malaria if they were told, and the type of treatment they were given.
Methods
Study Area
The study was conducted in Siaya County Referral Hospital (SCRH) and Bondo Sub-County Hospital of Siaya County, Kenya. Siaya and Bondo hospitals receive an average of 118 Antenatal Care Clinic (ANC) first visits per month, giving an estimate of about 1416 pregnant women per year as a study population with a monthly average of 52 clients having attended at least 4 ANC visits as per the Kenya Health Information System website accessed in 2014-DHIS2 giving a target population of 624 pregnant women.
Study Population
The study participants were pregnant women and who had attended SCRH and Bondo Sub-County hospital for ANC clinic visit.
Study Design
A descriptive cross-sectional design was used in this study. The data was collected using pre-tested questionnaires. A team of ten community interviewers selected by the principal investigator were taken through Good Clinical Practices (GCP), the objective of the study, and ways of obtaining consent and data from the participants for four days. Data collection was done through face-to-face interviews.
Statistical Analysis
Data Analysis was done using STATA 17 (STATA Corp, Texas and USA). The respondent’s demographic and social characteristics were presented using frequencies and percentages. Means, median and interquartile ranges were used to describe continuous data. Fisher’s Exact and Chi square test was performed to show comparison of categorical data.
Results
The study included 237 pregnant women aged 18 to 45. 14 women were aware of the effects of ACTs in the first trimester, while 223 were not aware of the impact of ACTs in the first trimester. The median age (IQR) for women and gestational age at enrolment was 26(22, 30.0) years and 18(14,20) weeks, respectively. The majority of the respondents
- were below 25 years (46.4%). A total of 213(90%) of the respondents stated that they were married. More than half of the respondents had primary school education, while only 30(12.6%) had completed university education. Only
- 49(20.5%) were in their first pregnancy during this study.
- Not Aware of the Effects of ACTs in the First
- Trimester, N=223 p-Value (chi/ exact) n (%) n (%) n (%)
- Age
- All, N=237
- Aware of Effects of ACTs in the 1st Trimester=14
- < 25 years
- 109(46.4)
- 6(42.6)
- 104(46.4)
- 0.525
- 25 - 35 Years
- 110(46.3)
- 7(49.6)
- 103(46.0)
- ≥ 35 years
- 18(7.6)
- 1(7.8)
- 17(7.5)
- Median (IQR)
- 25.5(21.9,30.0)
- 26.3(22.7-30.3)
- 25.5(21.9,30.0)
- 0.093
- Gestation
- Median (IQR)
- 18(14,20)
- 15.5(12.0,19.0)
- 18.0(14.0,20.0)
- <0.001
- Marital status
- Single
- 22(9.5)
- 1(7.0)
- 21(9.6)
- 0.042
- Married
- 213(90.0)
- 13(91.7)
- 200(89.9)
- Widowed
- 1(0.4)
- 0(1.3)
- 1(0.3)
- Education Level
- Never attended school
- 2(0.7)
- 0(0.0)
- 24(0.7)
- 0.006
- Primary
- 127(53.3)
- 7(50.0)
- 120(53.8)
- Secondary
- 79(33.2)
- 4(30.0)
- 75(33.4) college
- 29(12.6)
- 3(20.0)
- 27(12.1)
- First Pregnancy
- 49(20.5)
- 2(16.5)
- 46(20.7)
- 0.126
Table 1: Demographic Characteristics of the respondents.
Knowledge of Malaria Treatment Practices
Most participants, 170(7173%), reported that the type of malaria drug prescribed depended on the availability of the drug (78.9%) and the age of the patient (62. 8%). The majority of the participants also reported that their most preferred drug for treatment was AL 165(69.2), followed by artesunate-amodiaquine 16(6.7%). The main reasons for choosing AL over other antimalarial include; the availability 100 (60%) and affordability 42(25.45%) of the drug in various clinics and drug stores (Table 2).
| Knowledge of types of ACT | ||
|---|---|---|
| Known | Available | |
| n(%) | n(%) | |
| Artemether-Lumefantrine | 215(90.7) | 210(88.6) |
| Artesunate Amodiaquine | 30(12.7) | 15(6.3) |
| Artemisinin-SP | 14(5.9) | 10(4.2) |
| Dihydroartemisinin-piperaquine | 0 | 0 |
| Piperaquine-Artesunate | 20(8.4) | 15(6.3) |
| Chloroproguanil-Dapsone | 0 | 0 |
Table 2: Knowledge of Artemisinin Based combinations.
Knowledge and Availability of Different Types of ACT
Majority of the participants were aware of or had heard about at least one ACT and were able to mention at least a single type of ACT 215(90.7%) and stated that they were available in various pharmacies and clinics 210(88.6%). Artesunate Amodiaquine was the second most known ACT 30(12.7%). None of the participants was aware of the Dihydroartemisinin-piperaquine and Chloroproguanil- Dapsone. The majority of the participants could not identify the drugs with generic names; hence they reminded the participants of the trade names (Figure 1).
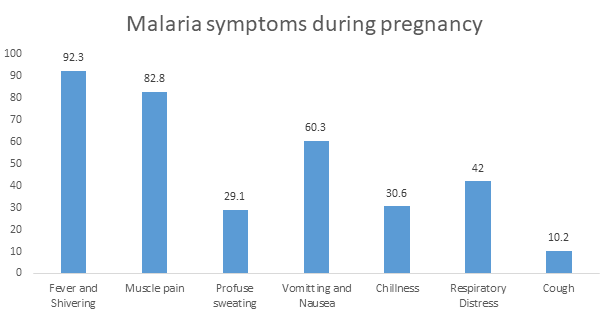
Malaria Symptoms During Pregnancy
Fiver and shivering was the most common malaria symptom experienced by most mothers 92.3%. During pregnancy other common malaria symptoms stated by the participants include; Muscle pain 82.8%, vomiting and nausea 60.3%, respiratory distress 42%, chilliness 30.6%, profuse sweating 29.1% and intermittent cough 10.2%. Majority of the participants indicated having a combination of more than two symptoms during the malaria episode (Figure 2).
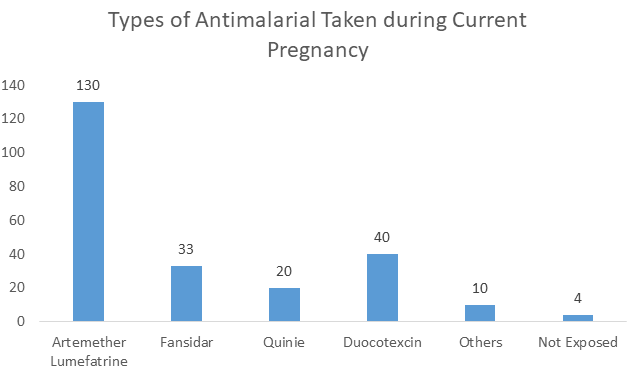
Types of Antimalarial taken During the Current Pregnancy
Artemether Lumefantrine was the drug majority of the participants had been exposed to during their current Pregnancy 130(54.85%). This represents more than half of the participants. The next most popular drug was duocotexcin which 40(16.87%) of the mothers reported to have been exposed to. A total of 33(13.92%) of the mothers indicated to have been exposed to Fansidar, 20(8.44%) and 10(4.22%) of the mothers reported to have used other malaria drugs. They could not remember their names. Only 4(1.68%) reported not being exposed to any antimalarial during their current pregnancy.
| Side Effect | n (%) |
|---|---|
| Vomiting | 44(18.57%) |
| Dizziness | 46(19.41%) |
| Diarrhea | 38(16.03%) |
| Headache | 17(7.17%) |
| Abdominal pain | 41(17.30%) |
| Weakness/fatigue | 12(5.06%) |
| Nausea | 54(22.78%) |
Table 3: Side Effects of taking ACTs.
Reported Side Effects of Taking ACTs
Most participants, 54(22.78%), indicated that dizziness was the most notable side effect of ACT. They also noted that other symptoms such as dizziness 46(19.41%), vomiting 44(18.57%), abdominal pain 41(17.30%), and diarrhea were also common after taking ACTs. The participants also indicated that more than one side effect would occur during a malaria episode, i.e., nausea and dizziness (Figure 3).
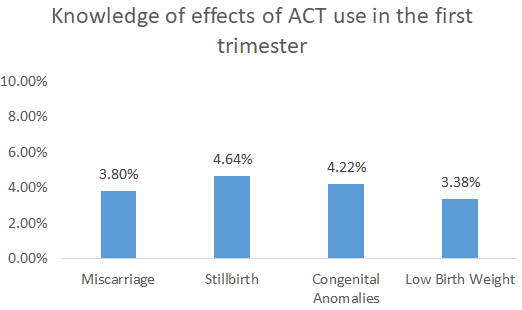
Knowledge of Effects of ACT use in the First Trimester of Pregnancy
The participants were asked about their knowledge of the effects of ACT use in the first trimester of pregnancy. The significant effects probed were Miscarriage, Stillbirth, congenital anomalies, and low birth weight. More than 90% of the participants were unaware of the effects of ACT use in early pregnancy. A total of 11 (4.64%) of the participants were aware that ACT use in early pregnancy could cause stillbirth, 10 (4.22%) congenital anomalies, 9 (3.8%) miscarriage, and 8(3.4%).
Discussion
The study aimed at assessing the level of knowledge and attitude of pregnant women on ACT use in early pregnancy. Majority of the participants were aware of malaria and its signs and symptoms. However, they were not aware of the risk associated with malaria and ACT use in the first trimester of pregnancy. Most participants 90%, knew at least one type of ACT (Artemether Lumefantrine), the most common malaria drug in the region, and could name at least two common malaria symptoms fever 92.3% and shivering 82.8%. Majority of the participants who stated that they had been exposed to malaria stated to have been prescribed AL for treatment and reported nausea 22.78% and dizziness 19.41% as the most common side effects experienced after consuming the drugs. There was low awareness of adverse pregnancy outcomes due to exposure to ACTs in the first trimester of pregnancy.
WHO guidelines on maternal and neonatal health specify that the first ANC visit should come before the 16th week of Pregnancy [11]. This study found that the majority of the women presented themselves for their first ANC late at around 18 weeks or more. Most pregnant women in rural areas are not equipped with adequate information on importance of early antenatal care (Warri and George 2020). This shows that these women present themselves to the ANC clinic in the second or third trimester hence unable to receive the required two doses of SP for IPT [17]. Late ANC would also support why most women reported having experienced at least malaria episode during pregnancy. IPT with SP has been shown to effectively prevent malaria and adverse outcomes associated with malaria [18, 19]. Early ANC attendance results in higher chances of complete dose uptake of SP hence increasing chances of preventing malaria during pregnancy.
Even though ACT is common and readily available in most hospitals and clinics, it is not recommended for malaria treatment in first trimester of pregnancy unless the mother’s life is at risk or quinine is not available [20]. This study found that more than half of the women were given AL for treatment of malaria in the first trimester of pregnancy. This can be attributed to little knowledge among healthcare workers and the failure of women of child-bearing age to disclose their pregnancy status to the healthcare providers before seeking treatment [21]. Majority of those who took AL reported mild side effects such as nausea and vomiting as side effects of the drug. Despite this, AL has one of the highest adherence rates among malaria drugs compared to other drugs, such as quinine which has unpleasant side effects such as blurred vision, high-tone hearing impairment, and tinnitus [22]. AL, therefore, becomes the following readily available alternative for malaria treatment.
The study had the following limitations. The research used a convenience sample of participants who presented themselves to the ANC clinics in SCRH and Bondo Sub- County Referral hospital and did not involve pregnant participants at home who might have had a different opinion from the individuals who participated in this study. Some participants could not remember the medicine’s exact drug names, hence failure to capture all the information. There is a need to conduct extensive studies to understand if the level of knowledge of ACT use in pregnancy in urban areas would be different. The study managed to obtain critical information on the knowledge of pregnant women in Siaya County on ACT use.
Conclusion
Most pregnant women had little knowledge about the effects using Artemisinin-based combination for malaria treatment in the first trimester of pregnancy. There needs to regularly sensitize women about the risks of using ACT for malaria treatment in the first trimester. They also need to always state their pregnancy status to the doctor or pharmacist whenever they seek malaria treatment. Sensitization should be done to reach pregnant women presenting themselves at the clinic or those still in the community.
Conflict of Interest
Authors declare no conflict of interest.
Funding
The study expenses were fully met by the corresponding author Mr. Michael Otieno.
Informed Consent
Written informed consent was obtained from the study participants prior to starting the study.
Authors’ Contribution
Michael Otieno wrote the first draft of the manuscript. Denis Odhiambo Omondi, Jorim Opiyo Ayugi helped with data analysis. George Ayodo, Martina Oneko, Nancy Atieno Otieno, Bryan Otieno Nyawanda, Cliff Oduol and Denis Odhiambo reviewed and made inputs into the intelectual content and further agreed on its publication.
References
-
(2020) World Malaria Report 2020: 20 Years of Global Progress and Challenges. World Health Organization, pp: 299.
-
(2012) World Malaria Report: 2012. World Health Organization.
-
Briand V, Saal J, Ghafari C, Huynh BT, Fievet N, et al. (2016) Fetal Growth Restriction Is Associated with Malaria in Pregnancy: A Prospective Longitudinal Study in Benin. J Infect Dis 214(3): 417-425.
-
Lawn JE, Blencowe H, Waiswa P, Amouzou A, Mathers C, et al. (2016) Stillbirths: Rates, Risk Factors, and Acceleration towards 2030. The Lancet 387(10018): 587-603.
-
Ouedraogo S, Koura GK, Bodeau-Livinec F, Accrombessi MM, Massougbodji A, et al. (2013) Maternal Anemia in Pregnancy: Assessing the Effect of Routine Preventive Measures in a Malaria-Endemic Area. Am J Trop Med Hyg 88(2): 292-300.
-
Walker PG, Floyd J, Ter Kuile F, Cairns M (2017) Estimated Impact on Birth Weight of Scaling up Intermittent Preventive Treatment of Malaria in Pregnancy given Sulphadoxine-Pyrimethamine Resistance in Africa: A Mathematical Model. PLoS Med 14(2): e1002243.
-
Kwenti TE (2018) Malaria and HIV Coinfection in Sub- Saharan Africa: Prevalence, Impact, and Treatment Strategies. Res Rep Trop Med 9: 123-136.
-
Nega D, Dana D, Tefera T, Eshetu T (2015) Prevalence and Predictors of Asymptomatic Malaria Parasitemia among Pregnant Women in the Rural Surroundings of Arbaminch Town, South Ethiopia. PloS One 10(4): e0123630.
-
Adepeju IS (2017) Prevalence of Malaria Parasite among Asymptomatic and Symptomatic Students of Federal University of Technology, Akure, Ondo State. Br J Res 4(1).
-
Burger RJ, van Eijk AM, Bussink M, Hill J, Ter Kuile FO, et al. (2016) Artemisinin-Based Combination Therapy versus Quinine or Other Combinations for Treatment of Uncomplicated Plasmodium Falciparum Malaria in the Second and Third Trimester of Pregnancy: A Systematic Review and Meta-Analysis. Open Forum Infect Dis 3(1): ofv170.
-
(2004) A Strategic Framework for Malaria Prevention and Control during Pregnancy in the African Region. World Health Organization.
-
White TE, Clark RL (2008) Sensitive Periods for Developmental Toxicity of Orally Administered Artesunate in the Rat. Birth Defects Res B Dev Reprod Toxicol 83(4): 407-417.
-
Clark RL (2009) Embryotoxicity of the Artemisinin Antimalarials and Potential Consequences for Use in Women in the First Trimester. Reprod Toxicol 28(3): 285-296.
-
Hill J, D’Mello-Guyett L, Hoyt J, van Eijk AM, ter Kuile FO, et al. (2014) Women’s Access and Provider Practices for the Case Management of Malaria during Pregnancy: A Systematic Review and Meta-Analysis. PLoS Med 11(8): e1001688.
-
Manyando C, Mkandawire R, Puma L, Sinkala M, Mpabalwani E, et al. (2010) Safety of Artemether- Lumefantrine in Pregnant Women with Malaria: Results of a Prospective Cohort Study in Zambia. Malar J 9: 249.
-
Warri D, George A (2020) Perceptions of Pregnant Women of Reasons for Late Initiation of Antenatal Care: A Qualitative Interview Study. BMC Pregnancy Childbirth 20(1): 70.
-
Doku DT, Zankawah MM, Adu-Gyamfi AB (2016) Factors Influencing Dropout Rate of Intermittent Preventive Treatment of Malaria during Pregnancy. BMC Res Notes 9(1): 460.
-
Nyarko AY, Newton SK, Annor RB, Owusu-Dabo E (2020) The Effectiveness of the Revised Intermittent Preventive Treatment with Sulphadoxine Pyrimethamine (IPTP-SP) in the Prevention of Malaria among Pregnant Women in Northern Ghana. Journal of Tropical Medicine 2020: 9.
-
Olaleye A, Okusanya BO, Oduwole O, Esu E, Meremikwu M, et al. (2019) A Systematic Review and Meta‐analysis of Dihydroartemisinin‐piperaquine versus Sulphadoxine‐ pyrimethamine for Malaria Prevention in Pregnancy. Int J Gynaecol Obstet 146(1): 43-55.
-
(2007) Assessment of the Safety of Artemisinin Compounds in Pregnancy: Report of Two Joint Informal Consultations Convened in 2006. World Health Organization.
-
Riley C, Dellicour S, Ouma P, Kioko U, Omar A, et al. (2018) Knowledge and Adherence to the National Guidelines for Malaria Diagnosis in Pregnancy among Health-Care Providers and Drug-Outlet Dispensers in Rural Western Kenya. Am J Trop Med Hyg 98(5): 1367-1373.
-
Yeka A, Achan J, D’Alessandro U, Talisuna AO (2009) Quinine Monotherapy for Treating Uncomplicated Malaria in the Era of Artemisinin-Based Combination Therapy: An Appropriate Public Health Policy? Lancet Infect Dis 9(7): 448-452.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines