Population Behavioral Dynamics and Government Response to COVID-19 Prevention in Uganda: Insights from Economic Epidemiology and Game Theory
This paper attempts to account for the role of population behavioral dynamics in urgent public health investment-decision making during outbreak of pandemics such as COVID-19. We developed game theory simulations based on the rational epidemics theory of infectious diseases to illustrate population behavior and rational decision making by government prior provision of preventive care during a pandemic such as COVID-19. We discuss the optimal time for government to invest in preventive healthcare such as public provision facemasks at different levels of disease prevalence. From our simulations, it is irrational for government to make a direct investment in preventive healthcare such as public provision of free facemasks to the populations during low disease prevalence (for example, during wave one of COVID-19 in Uganda). For instance, a time when diseases prevalence is below the threshold prevalence for which individuals/population is willing to demand for and utilize protective healthcare such as facemasks to protect themselves from contacting the disease (COVID-19). We conclude that the timing for government investment in relation to disease prevalence levels is critical. Second, during low disease prevalence, government should invest more in health promotion since preventive health care could result into allocative inefficiency. Third, any direct investment in preventive health care should go to the most at risk individuals even when the entire population is seemingly at risk.
Introduction
By the November 2022, about 639.5 Million positive COVID-19 cases and 6.6 Million deaths had occurred globally [1]. The outbreak of Coronavirus Disease (COVID-19) Conceptual Paper prompted unprecedented public health response by governments’ world over. The measures largely aimed to stimulate individual behavior towards preventive health care. These include public awareness, socioeconomic support, subsidies, provision and enforcement of social distancing, face masking and vaccination [2, 3]. The COVID-19 measures came amid economies for both developed and developing countries alike, experiencing distortions in growth targets owing to COVID-19 pandemic. .The World Bank projected a decline global growth rate from 5.5 percent recorded in 2021 to 4.1 percent in 2022, this expected to fall farther to 3.2 percent by2023. Whereas the COVID-19 outbreak led to unprecedented public health investments globally, we argue that resources for health could be used more efficiently when population demand dynamics for preventive health care during pandemics are well articulated. Uganda registered her first case of covid-19 on the 21 March 2020 [4]. With urgent need to ensure the health of all citizens, a multi sectoral approach to contain the spread and negative impacts of COVID-19 was adopted (ref Richard UNDP report). For instance, the Government of Uganda committed to provide facemasks to all people aged six years and above in the earlier phase of COVID-19. Like other infectious diseases, the role of human behavioral dynamics during the COVID-19 pandemic is crucial and thus, a determinant of the timeliness and effectiveness of public health policy intervention. We use perspectives from economic epidemiology to make a case against this public finance decision. The key question this study answered is whether it was timely to make public finance decision before the second wave of COVID-19 in Uganda. The first wave of COVID-19 in Uganda occurred between October 2020 and February 2021 after which, there was a sharp drop in the number of new cases and deaths [5, 6]. In June 2020, the Government of Uganda through the Ministry of Health started to provide facemasks to the entire population to contain transmission, avert death, and optimize the health system. The estimated cost of procurement and distribution of facemasks was over USD 23 Million (UGX 81.2 billion) to cover an estimated population of 32 Million Ugandans above six years of aged [7]. By the end of the first wave, the country had recorded about 40,000 confirmed cases and over 300 deaths with Kampala city having the highest number of cases [5]. Notwithstanding, the government further eased the nationwide lockdown in a phased approach putting more emphasis on wearing facemasks, social distancing and hand hygiene.
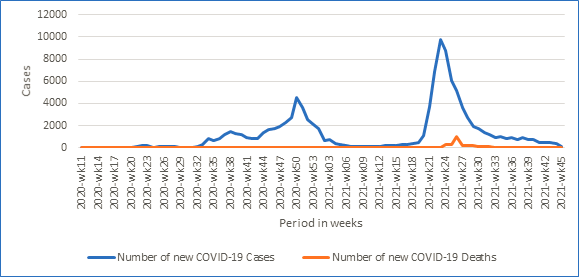
Source: Uganda Ministry of Health, Covid-19 Response Hub. Figure 1: Trend of COVID-19 cases in Uganda, the 1st and 2nd wave between October 2020 and November 2021.
The World Health Organization (WHO) recommended wearing of facemasks as part of a comprehensive public health measure to contain COVID-19 transmission [8, 9]. In Uganda, adherence to wearing of facemasks in public places remained suboptimal before the second wave of COVID-19, Indeed, related studies conducted in and around Kampala in the same period, showed that wearing facemasks in public places was not universally embraced [10, 11], despite awareness and initial public provision and enforcement of face masking. By June 2021, Uganda was experiencing the second wave of COVID-19, where the positivity rate reached 21%, new cases and death more than doubled, daily hospital admissions averaged 142 cases, public hospital beds dedicated for COVID-19 management became unavailable and private hospitals became unaffordable for majority of covid-19 patients [12]. At this point, the risk of acquiring COVID-19 had surpassed the cost of prevention. Consequently, adherence to wearing facemasks and private demand for facemasks increased significantly, the Government reinstated the nationwide lockdown, among other public health measures.
Some studies have been conducted on COVID-19 epidemiology and transmission dynamics [13, 14, 15], while a few have explored the role of behavioral science in COVID-19 response [16, 17]. In addition, two studies conducted in Uganda have explored knowledge, attitudes and acceptability of facemasks [18, 19] and other African studies have looked at determinants of wearing facemask [20, 21]. Other facemask studies related to COVID-19 were conducted outside Africa [22, 23]. The rational of this paper is to account for the role of population behavioral dynamics in public health decisions during outbreak of epidemics. We attempt to validate the untimeliness of public provision of facemasks in Uganda at a time when the perceived risk of acquiring COVID-19 was low in the population. The goal is to inform decision makers on the role of population behavioral dynamics to disease risks and transmission, when considering public provision of preventive health care. We also aim to contribute to theoretical literature on the economics of infectious diseases using COVID-19, a new phenomenon of the 21st Century.
The rest of the paper is organized in such a way that, in section II and III we conceptualize the theoretical foundations of our argument. Section IV we illustrate population preventive behaviors during the first (low prevalence) and second (high prevalence) waves of COVID-19 using game theoretical concepts and assumptions. We then turn to discuss the outputs of our theoretical simulations. Finally, we conclude with some policy imperatives of this paper to health policy decision making.
Theoretical Foundation and Conceptualization
In their earlier work, Geoffard, et al. [24] explored the use of economic modelling to predict the spread of infectious diseases in contrast with assumptions of biological epidemiology. They discuss extensively about the interactions between disease prevalence and individual demand for preventive care. The theory of rational epidemics postulates that during outbreak of epidemics, increase in disease prevalence provides incentive for private demand of preventive care and stimulates risk aversive behavior that, in turn curtail further spread of disease [24, 25]. Key assumptions include; a closed population with two individuals who are either susceptible or infected, who either choose to protect or expose themselves to infection. Individuals continue to interact with each other and at each interaction, they make a choice to protect or get expose to disease. The risk of infection increases with more exposure among susceptible individuals and vice versa. Protective behavior and exposure are costly given the state transition probability from susceptibility to infection.
Further, Geoffard, et al. [24] argue that individual protective behavior is stimulated when the perceived cost of protection in terms of affordability and discomfort of using preventive health care (wearing a facemask in this case) is below the expected cost of risking infection through exposure. This is because there exists a threshold prevalence level for which exposure decreases and protective behavior increases due to increase in transmission probability. Further, they postulate that in economic epidemiology, the hazard rate is a decreasing function of disease prevalence. This is because susceptible individuals face a larger risk of infection and chose protective behaviors. In this paper, we focus our discussion on Government provision of facemasks (one of the immediate preventives measure the government adopted) and individual behavioral response in Uganda based on these theoretical constructs. Rational Behavior and Public Intervention The theory of rational epidemics intersects the private decision problem with the public decision problem. During the outbreak of infectious diseases, individuals face a decision to either protect or expose themselves given their status (infected or susceptible) and other constraints, while Government is responsible to influence individual decision to minimize risk of infection through public policy [26]. Geoffard, et al. [24] extended their model to include the effectiveness of public subsidy on influencing population behavioral response to disease. They argue that, the effectiveness of public health interventions designed to stimulate protective behavior against further spread of disease is a function of individual prevalence elastic behavior and timeliness of the government subsidy. This follows that, during periods of high disease prevalence, a public subsidy is more effective to induce individual protective behavior in terms increased demand for preventive health care; such as increased use of facemasks, which yields economic efficiency of public investment. However, at a time of low disease prevalence, public subsidy is ineffective to induce individual protective behavior and consequently, the demand for preventive health care is ineffective. Additionally, Phillipson (1996) argued that, as population preventive behaviors respond strongly to disease prevalence levels, there is a crowding out effect on the Pigouvian subsidy and other public health measures intended to stimulate demand for prevention and increase in protective behaviors against a disease [25]. This reasoning forms the basis for our argument in the current paper.
Illustration of Theory of Rational Epidemics using Game Theoretic Simulations
We applied game theory simulations to aggregate individual behavior in response to disease prevalence at two scenarios of low (first wave) and high (second wave) COVID-19 prevalence in Uganda. In this section, we illustrate two game theory concepts of “belief revision” and “sequential rationality”. We build on these concepts to make a case for the optimal scenario (timing) for government intervention for example, public provision of facemasks to protect against COVID-19 in this case.
Our starting point is the concept of “belief revision” extensively discussed by Bonanno [27]. Suppose that prior to the first wave of COVID-19 the Ministry of Health (MOH) announces the expected mortality rate due to COVID-19 infections based on expert computations (new information set). Assuming that the actual initial COVID-19 prevalence and mortality rates where very low, and that the population knows this information. Rational individuals upon receiving the new set of information will adjust their beliefs about COVID-19 expected infection and mortality outcomes by assigning new probabilities to each possible state. Given a game form were consists of a set of three players categorized by their risk taking levels, with; player 1 (risk neutral), player 2 (risk averse) and player 3 (risk takers). is an information set with possible states of mortality rate (where and that) and, representing probability distribution on each possible state of mortality given the players belief on the information set.
Let where If Then,
Where represents the possible states of COVID-19 mortality, ranging (between 250 to 1000 deaths per every 100,000 population) in the first wave given the information set. Numbers within each state are arranged in chronology to the player’s risk-taking category, for instance state , means 500 is the expected mortality rate by player 1 (risk neutral), 1000 by player 2 (risk averse) and 250 by player 3 (risk takers). Player’s beliefs on the likelihood of each state given is expressed as a probability distribution over each state. Consider a risk averse individual (player 2), given would assign higher probabilities to states with worst expected outcomes thus, are more likely than all other states. Implying that, risk averse individuals consider it very likely that at least 1000 people will die due to COVID-19 during the outbreak of the first wave. From the above expressions of, we can compute the total probability of a worst outcome (1000 deaths) for players 2 (risk averse) and 3 (risk takers) using probability distributions in table 1.
| U | x 1 | x 2 | x 3 | x 4 | x 5 | x 6 |
|---|---|---|---|---|---|---|
| P2 | 1∕18 | 0 | 7∕18 | 0 | 8∕18 | 2∕18 |
| P3 | 2∕7 | 1∕7 | 2∕7 | 0 | 1∕7 | 1∕7 |
| Pi2 | 3∕18 | 1∕18 | 15∕18 | 1∕18 | 5∕18 | 3∕18 |
| Pi3 | 1∕7 | 2∕7 | 1∕7 | 0 | 2∕7 | 0 |
Table 1: Probability Distribution for Expected Mortality at each state before and after the first wave. Where: U – new informatio
Table 1: Probability Distribution for Expected Mortality at each state before and after the first wave. Where: U – new information set, P – probabilities for U before wave one, Pⁱ – new probabilities for U with additional information after wave one of COVID-19 and, P₂ - player two (risk averse) and P₃ - player three (risk taker). Given that, the probability that at least 1000 deaths will occur due to COVID-19 during the first wave is given as, For Player 2 (risk averse), from We obtain, While, Player 3 (risk takers), In the above expressions, risk-takers (with low demand for preventive care) least expect COVID-19 to be severe during the first wave, with a lower total probability (14%) of at least 1000 deaths occurring during the first wave. However, risk averse individuals (Player 2) expect the worst outcome of 1000 deaths to be more likely with probability. Now suppose that the Ministry of Health (MOH) announces a possible outbreak of the second wave of COVID-19 due to importation of a new and more severe COVID-19 variant. We also suppose that the MOH makes additional announcements that during the first wave of COVID-19, mortality rate was lower than predicted, with the highest mortality rate recorded as 400 deaths per 100,000 population. This additional information implies that initial probabilistic beliefs held by players at each possible state given previous information set are no longer true e.g. states and for player 2 are not reached. Therefore, players will revise their beliefs by assigning new probabilities to each state given additional information on mortality outcomes during the first wave (Table 1).
In response to additional information, we expect players to assign lower probabilities to states with worst mortality outcome such as and assign higher probabilities to states with moderate outcomes such as. We also expect that more people will move from being risk averse to being risk neutral or even risk loving by assigning lower probabilities to states with worst possible outcomes (table 1). Consider Player 2 (risk averse), with a new probability distribution following the additional information (table 1). The total probability assigned to the worst possible outcomes with updated beliefs will fall as shown below;
Player 2: From, Therefore;
Risk averse individuals (Player 2) will therefore revise their belief of a worst outcome such as to lower subjective probabilities thus, yielding a lower total probability). This implies that private demand and utilization of preventive health care will be suboptimal in the entire population during periods of low disease prevalence and risk of infection.
We now turn to the concept of “sequential rationality” building on belief-revision illustrated above. Sequential rationality requires that individual strategy choices at each information set maximize their expected utility given their specified beliefs at the given information set regardless of whether the beliefs are true [27, 28]. For instance, given two players, 1 and 2, two strategies of wearing a facemask or no facemask, and that the expected utility from moving about without wearing a facemask (exposure) is high for risk takers (Player 1) compared to risk averse (player 2) individuals. Sequential rationality requires that Player 1’s strategy choice is not to wear a facemask given their initial belief that COVID-19 prevalence is low and the reverse is true for risk averse individuals.
Using an extensive-form game with hypothetical cardinal payoffs, we illustrate the concept of sequential rationality in two scenarios of low COVID-19 prevalence (wave 1) and high COVID-19 prevalence (wave 2). Given prevalence information set and possible mortality outcome states with corresponding probabilistic beliefs for each possible state given and, a profile of behavioral strategy with corresponding action probabilities (table 2), we illustrate the extensive game-form in two scenarios (first and second wave of COVID-19). Given three players, one (risk neutral), two (risk averse) and three (risk taker). Two strategy profiles of wearing a facemask hereafter, or no facemask hereafter, for each player at every decision node. We assume a system of beliefs on given information set represented by probability distributions () at each information subset. Each player assigns a probability () on their strategy profile or . We denote probability values during the second wave (scenario 2) with superscripts (Table 2). Contextual definitions of some game theory concepts applied here are published elsewhere [29].
| Information sets (u) | Player 1 (risk meutral) | Players 2 (risk averse) | Player 3 (risk taker) | |||
|---|---|---|---|---|---|---|
| H | K | x | y | w | z | |
| p | 1∕2 | 1∕2 | 2∕7 | 5∕7 | 4∕5 | 1∕5 |
| pi | 1∕2 | 1∕2 | 1∕7 | 6∕7 | 6∕5 | 2∕5 |
| Strategies (s) | NM1 | WF1 | NM2 | WF2 | NM3 | WF3 |
| ps | 2∕3 | 1∕3 | 3∕5 | 2∕5 | 1 | 0 |
| pis | 1∕3 | 2∕3 | 0 | 1 | 3∕7 | 4∕7 |
Table 2: Probability Distribution on Information Sets and Individual Strategy during First and Second COVID-19 wave. Where: U – P
Table 2: Probability Distribution on Information Sets and Individual Strategy during First and Second COVID-19 wave. Where: U – Prevalence information on COVID-19. P – probabilities for U during wave 1 , Pᵢⁱ – new probabilities for U with additional information during wave 2, Pₛ - probability for player strategy profile during wave 1, Pⁱₛ - probability for player strategy profile during wave 2. NM – not wearing facemask and WF – wearing a facemask. (h, k), (x, y) and (w, z) are possible states of mortality outcomes given U. i.e. for player 2 (risk averse) x is a state with low expected mortality rates while y represents the worst expected mortality outcome given U. Player 1 (risk neutral) is indifferent between state h and k, with equal probabilistic belief of a half.
We further assume a low behavioral elasticity to disease prevalence information during the first COVID-19 wave scenario 1 such that, the bigger population prefers exposure (risk taking) or at least risk neutral (with low demand for facemasks) and that risk averse individual’s strategy profiles are not consistent with their beliefs during this wave. In the second wave (scenario 2), we assume a higher behavioral elasticity to disease prevalence information and that majority of the population adopt risk aversive behavior (increasing demand for and utilization of facemasks) due to rational belief revision.
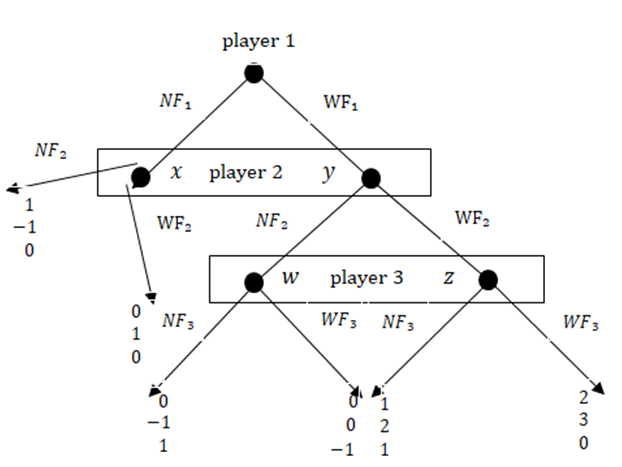
Figure 3: Shows the extensive-form game for three players, player 1-risk neutral, player 2-risk averse and player 3-risk taker during the first wave of COVID-19 (scenario 1). There are two strategies, not wearing a facemask (NF) and wearing a facemask (WF). Player 2 and 3 strategy choice is based on their probabilistic beliefs on the possible mortality outcome states (x, y) and (w, z) respectively. i.e. for player 3 (risk taker), state w represent fewer expected deaths due to COVID-19 while state z shows the worst expected mortality rate given COVID-19 prevalence information during wave 1. Values at the terminal node of each choice strategy represent individual cardinal payoffs given their choice strategy and probability distribution at each possible state of mortality outcome.
In scenario 1 (Figure 1), we verify sequential rationality for Player 2 (risk averse) and Player 3 (risk taker). Sequential rationality requires that Player 2 plays and Player 3 play at their information sets. Consider that player 2’s information set and that Player 3’s optimal strategy is, Player 2 yields an expected payoff for playing. However, suppose Player 2 plays their choice strategy with probability 1, they yield a higher expected payoff. Therefore, Player 2’s strategy profile is suboptimal and thus sequentially irrational in this scenario. Now consider that Player 3’s information set is attained and that Player 2’s strategy is, playing yields while, playing yields thus, playing is sequentially rational for Player 3 (risk taker) in scenario 1 during low covid-19 prevalence.
In scenario 2 (Figure 4 & 5) with high COVID-19 prevalence, consider a risk averse individual (Player 2) knowing that his information set is reached, would play their choice strategy optimally with a higher probability 1 at node Y expecting that Player 3 is most likely to chose . This yields a positive expected payoff. Given high disease prevalence, at information set, Player 3 (risk taker) updates his belief and is forced to play his choice strategy sub-optimally.
Therefore, playing yields, while playing yields a positive expected payoff. Thus, playing is optimal but sequentially irrational for player 3 since they would prefer not to wear a facemask given their initial probabilistic belief on COVID-19 prevalence information. In scenario 2, private demand for and use of facemasks is expected to increase sharply in the population ceteris paribus.
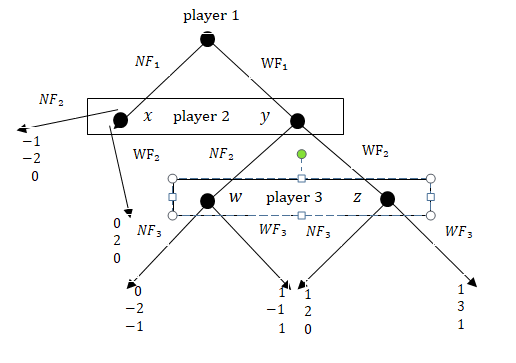
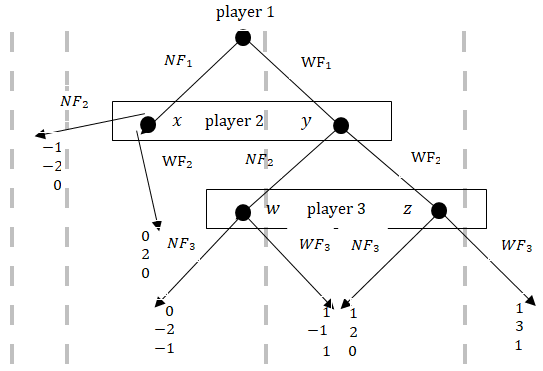
Figure 5: Shows player strategy profiles during the second and high wave of COVID-19 (scenario 2). Two choice strategies, not wearing a facemask (NF) and wearing a facemask (WF). Player 2 and 3 strategy choice is based on their probability distribution on the possible mortality outcome states (x, y) and (w, z) respectively. i.e. for player 2 (risk averse), state x represent few expected deaths due to COVID-19 while state y represents high mortality rates expected during the second wave given the updated COVID-19 prevalence information received by each players. Values at the terminal node of each choice strategy represent individual cardinal payoffs given their choice strategy and probability distribution at each possible state of mortality outcome.
Discussion
Health Behavior and Preventive Healthcare Demand; we explore important features of population demand characteristics for preventive health care at different disease prevalence levels. We incorporate game theory concepts of believe revision and sequential rationality to simulate individual utilization of facemask under different COVID-19 prevalence levels. The important deduction is that preventive health behavior is sensitive to disease prevalence levels.
Individuals through a mechanism of probabilistic belief revision adjust their protective behaviors subject to available prevalence information. We illustrate that in periods of low disease prevalence, individual behavioral response to disease threat is suboptimal. For instance, wearing a facemask would yield a positive but low expected payoff to risk averse individuals thus, it is not an optimal strategy even when they believe there is a potential threat of catching covid-19 (sequentially irrational). Similarly, wearing a facemask during low disease prevalence would yield a negative payoff to risk-taking individuals and they prefer exposure as there is no additional threat to their choice strategy of not wearing a facemask. In contrast, during high covid-19 prevalence illustrated in scenario two (Figure 2), wearing a facemask yields a high and positive payoff to risk averse individuals and a positive payoff to risk-takers due to belief revision mechanism. The intuition is such that, disease prevalence exceeds the threshold prevalence below which risk-taking individuals would continue exposing themselves (not wearing a facemask) thus, disrupting risk taking behaviors. Risk takers become sequentially inconsistent with their strategy choice (not wearing a facemask) given their beliefs and rather choose to protect themselves. Therefore, a public policy decision aimed to stimulate demand and utilization of preventive health care such as free provision of facemasks is more economically efficient, timely and effective at such a time.
Whereas evidence on population behavioral responsiveness to COVID-19 prevalence is still limited, in regards to non-pharmaceutical preventive measures especially wearing of facemasks, there is evidence to suggest that disease prevalence level is an important stimulus of human protective behaviors and consequently affects the timing and strategy of public health interventions. Two human behavioral studies in China showed that knowledge of disease and perceived risk of COVID-19 infection had a significant positive impact on wearing facemasks especially in the urban population [30, 31]. In relation to renowned infectious diseases such as HIV, malaria and measles, an observational study including HIV patients in Uganda showed that condom use was positively associated with HIV risk perception [32]. Another prevalence study showed that a 1% increase in HIV prevalence increased the propensity to use a condom significantly and up to 50% for the most prevalent responsive groups [33]. A related study in sub Saharan Africa showed that malaria prevalence had a positive effect sleeping under an insecticide treated bed net [34]. Prevalence of measles significantly reduced the age in months at which the first measles vaccine occurred [25]. The current paper contributes to previous literature on economic epidemiology by incorporating a discussion on the government decision problem given population behavioral response dynamics using a case of COVID-19.
Public Provision of Preventive Healthcare; This paper evokes a discussion on the timing of public subsidy or public provision of free preventive health care during outbreak of a pandemic in a resource-constrained context like Uganda. The simulation in scenario 1 (first wave) with a low COVID-19 prevalence indicates that demand and utilization of facemasks may remain low even with public provision of free facemasks. This is because with low disease prevalence, risk of infection and mortality, individual disease prevalence elasticity of demand for preventive health care is near zero [24]. This implies that individuals may not use facemasks even when they are available at zero cost. Consequently, a government decision to provide preventive healthcare to the entire population is rendered less effective in such a period due to lack of stimulus for individual demand for preventive health care.
The Grossman theory of health demand postulates that health is a commodity, for which individuals invest their resources and time to increase their health stock to continue working, enjoy leisure and earn more income [35]. Consider a period of high COVID-19 prevalence and mortality illustrated in scenario two (figure 2) individuals through the mechanism of probabilistic believe-revision would adjust their consumption bundles by investing and consuming more healthcare commodities to improve or maintain their health stock. Such an adjustment may include buying and wearing of facemasks, hand hygiene, seeking treatment and vaccination among other prescribed public health measures. This healthcare demand adjustment induces two health policy implications; first, a public health policy-decision to provide or subsidize preventive health care such as facemasks is more effective during periods of high disease prevalence, where individual responsiveness to disease threat is highly elastic. Secondly and more importantly, with high prevalence, private demand for and investment in preventive healthcare is expected to rise and, the population would not necessarily require free provision from government for such items which are relatively accessible and affordable in the open market. This allows focus of government resources towards the most vulnerable groups such as the elderly and border-entry communities (in the case of COVID-19 in Ugandan context) based on affordability and accessibility criteria of the needed preventive healthcare thus, yielding allocative efficiency.
Nonetheless, arguments presented in this paper should be considered in light of some limitations. This was a conceptual study that relied on limited information and published studies on the trends, demand and utilization of facemasks in Uganda. It is likely that the strength of our argument could be limited by the lack of sufficient information on facemask use. Therefore, future research should consider an empirical analysis using data on facemask demand, utilization and COVID-19 prevalence data in different settings for more generalization. Another limitation is the obvious one that COVID-19 outbreak was a new public health threat globally, that demanded unprecedented response by governments from those with more developed health systems to the least developed health systems alike. It is therefore unfair to claim that this kind of reasoning would be envisaged in such times of uncertainty. However, we are confident that this paper contributes to existing knowledge on the economics of infectious disease and will guide future public health approaches on existing infectious diseases and in the face of similar outbreaks to CIVID-19.
Conclusion
This paper explored the theory of economic epidemiology to illustrate a mechanism through which public health decisions such as public provision of preventive health care can be more effective in the face of an epidemic such as COVID-19. The goal is not to assert or estimate the allocative efficiency of government resources towards COVID-19 in Uganda, but rather to provide plausible considerations for public health policy given population behavior dynamics and disease prevalence levels. Beyond free public provision of preventive healthcare during an epidemic, the timing of government action in relation to population behavioral responsiveness to disease threat is crucial. We suggest that public provision or subsidies for preventive healthcare is more effective when directed to the most at risk categories based on affordability and accessibility criteria, even when the entire population is seemingly susceptible. Lastly, during low prevalence of a pandemic such COVID-19, government should invest more in health promotion other than direct investment in preventive care.
References
-
Worldometers (2022) Coronavirus Cases.
-
Ari-veikko A (2021) Successful government responses to the pandemic: contextualizing national and urban responses to the COVID-19 outbreak in East and West. JEPR 10(2): 17.
-
Edwards FL, Ott JS (2021) Government responses to the COVID-19 pandemic. Int J Public Admin 44(11-12): 879- 884.
-
(2020) MOH Ministry of Health, Update on the COVID-19 response in Uganda.
-
(2021) MOH Update on COVID-19 response in Uganda. Ministry of Health.
-
(2020) COVID-19 pandemic in Uganda.
-
(2020) MOH Update on COVID-19 response in Uganda. Ministry of Health.
-
(2020) WHO Mask use in the context of COVID-19: Interim guidance Geneva: World Health Organization.
-
Feng S, Shan C, Xia N, Song W, Fan M, et al. (2020) Rational use of face masks in the COVID-19 pandemic. Lancet Respir Med 8(5): 434-436.
-
Matovu JKB, kabwama SN, Ssekamatte T, Ssenkusu J, Wanyenze RK (2021) COVID 19 Awareness, Adoption of COVID 19 Preventive Measures, and Efects of COVID 19 Lockdown Among Adolescent Boys and Young Men in Kampala, Uganda. J Community Health 46(4): 842-853.
-
Bukuluki PM, Kisaakye P (2021) The Decision to Wear a Face Mask as a Protective Behavioral Measure Against COVID-19: Survey Results From Greater Kampala Metropolitan Area, Uganda. Front Public Health 21(9): 675-734.
-
(2021) MOH(c) The progress on containment of the second wave Press statement. Ministry of Health.
-
Murray EJ (2020) Epidemiology’s Time of Need: COVID-19 Calls for Epidemic-Related Economics. Journal of Econo Perspectives 34(4): 105-120.
-
Keppo J, Quercioli E, Kudlyak M, Smith L, Wilson A, et al. (2021) The behavioral SIR model, with applications to the Swine Flu and COVID-19 pandemics. Virtual Macro Seminar pp: 1-26.
-
Bi Q, Wu Y, Mei S, Ye C, Zou X, et al. (2020) Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: a retrospective cohort study. Lancet Infect Dis 20(8): 911-919.
-
McAdams D (2020) Nash SIR: An Economic- Epidemiological Model of Strategic Behavior During a Viral Epidemic. 16:115-134.
-
Bavel J, Baicker K, Boggio SP, Capraro V, Cichocka A, et al. (2020) Using social and behavioural science to support COVID-19 pandemic response. Nat Hum Behav 4: 460- 471.
-
Mboowa G, Musoke D, Bulafu D, Aruhomukama D (2020) Face-Masking, an Acceptable Protective Measure against COVID-19 in Ugandan High-Risk Groups. Am J Trop Med Hyg 104(2): 502-513.
-
Sikakulya F, Ssebuufu R, Mambo S, Pius T, Kamahoro E, et al. (2021) Use of face masks to limit the spread of the COVID-19 among western Ugandans: Knowledge, attitude and practices. PLoS ONE.
-
Dzisi EKJ, Dei OA (2020) Adherence to social distancing and wearing of masks within public transportation during the COVID 19 pandemic. Transportation Research Interdisciplinary. Perspectives
-
Ditekemena DJ, Nkamba MD, Muhindo HM, Siewe FNJ, Luhata C, et al. (2021) Factors associated with adherence to COVID-19 prevention measures in the Democratic Republic of the Congo (DRC): results of an online survey. BMJ Open 11(1).
-
Carbon C (2021) About the Acceptance of Wearing Face Masks in Times of a Pandemic. iPerception 12(3): 1-14.
-
Taylor S, Asmundson GJG (2021) Negative attitudes about facemasks during the COVID-19 pandemic: The dual importance of perceived ineffectiveness and psychological reactance. PLoS ONE 16(2)
-
Geoffard P, Philipson T (1996) Rational Epidemics and their public control. International Economic Review 37(3): 603-624.
-
Philipson T (1996) Private vaccination and public health: An empirical examination for U.S measles. The Journal of Human Resources 31(3): 611-630.
-
Perrings C, Castillo-Chavez C, Chowell G, Daszak P, Fenichel EP, et al. (2014) Merging Economics and Epidemiology to Improve the Prediction and Management of Infectious Disease. Ecohealth. 11(4): 464–475.
-
Bonanno G (2018) Game theory. In: 2nd (Edn.).
-
Yildiz M (2022) 14.12 Game Theory Lecture Notes Lectures pp: 15-18.
-
Ochanda P, Ssempala R, Kayongo A, Odokonyero T (2022) Insufficient declines in new HIV infection rates amidst high scores in HIV testing and awareness: ‘a game theory simulation’. Journal of Public Health 30: 2829-2834.
-
Kwok APK, Yan M, Huang YT, Gao C, Li WZ (2021) What shapes people’s willingness to wear a face mask at the beginning of a public health disaster? A qualitative study based on COVID-19 in China. Int J Disaster Risk Reduct 65.
-
Zhang B, Li Z, Jiang L (2021) The Intentions to Wear Face Masks and the Differences in Preventive Behaviors between Urban and Rural Areas during COVID-19: An Analysis Based on the Technology Acceptance Model. Int J Environ Res Public Health 18(19): 9988.
-
Innocent N, James M, Fred A, Jonathan O, Natal A (2003) Risk perception and condom use in Uganda. Afr Popul Stud.
-
Hotz V, Philipson T (1996) Responsiveness of the Demand for Condoms to the Local Prevalence of AIDS. Journal of Human Resources 21(4): 869-897.
-
Picone G, Kibler R, Apouey B (2017) Malaria Prevalence, Indoor Residual Spraying, and Insecticide Treated Net Usage in Sub-Saharan Africa. Journal of African Development 19(2): 19-32.
-
Grossman M (1972) On the Concept of Health Capital and the Demand for Health. Journal of Political Economy 80(2): 223-255.
-
Li Q, Guan X, Wu P, Wang X, Zhou L, et al. (2020) Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N Engl J Med 382: 1199-1207.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines