Study Females Intention to Practice Female Genital Mutilation for their Daughters at Beni Suef
Background: Female Genital Mutilation/Cutting practice became documented within the 28 countries of the European Union, Norway, and Switzerland as a result of migrations of females. The WHO originally prohibited the medicalization of FGM/C in 1979, at the first international conference on the subject. Aim: The present study was carried out to assess Females' Intention to practice Female Genital Mutilation for their Daughters at Beni-Suef. Subject & Methods: A Descriptive Cross-sectional study carried out in family health centers (FHCs) in different sitting at Beni- Suef Governorate. А Structured Interviewing Questionnaire sheet which includes knowledge regarding complications Female Genital Mutilation/Cutting, Intention to practice FGM/C, and Causes for intention or not to practicing FGM/C. Results: About 64% and 59.6% of females knew that FGM/C causes psychological and social problems, respectively, 56% had a misconception that FGM/C does not affect the woman's sexual satisfaction. About 29.7% are suffering from complications after FGM. About 47.9% of females had the intention to mutilate their daughters and support the continuation of FGM for young generations, 39.8% had already mutilated their daughters or sisters. The procedures were performed by physicians (61.1%), and 6.9% had complications. Conclusion: Most of females knew that FGM/C causes psychological problems and social problems; however most of them had misconception that FGM/C does not affect the woman's sexual satisfaction. Most the study sample had the intention to mutilate their daughters and support the continuation of FGM for young generations. The highest percent of procedures were performed by physicians. Recommendations: Motivations and behavior change of females and health care workers to perform FGM/C.
Introduction
Female Genital Mutilation/Cutting practice became documented within the 28 countries of the European Union, Norway, and Switzerland as a result of migrations of females. An estimated 578,068 out of 1,353,970 females in Europe had experienced FGM/C. As nearly half of these females live in the UK and France, it’s not surprising to seek that one out of two females who had experienced FGM/C in Europe lives in UK or France [1, 2, 3, 4, 5]. Female Genital Mutilation/Cutting is an ancient cultural practice, predating the Bible and therefore the Koran, and has no basis in any religion [6, 7, 8, 9]. Female Genital Mutilation/Cutting is related to deep social and cultural ideas impeded in several societies regarding femininity and modesty because it is viewed as girls clean and delightful only after being genitally cut. FGM/C is additionally viewed as a protection of virginity, and it prevents premarital sex [10, 11, 12, 13]. The WHO originally prohibited the medicalization of FGM/C in 1979, at the first international conference on the subject. This prohibition was reaffirmed in 1982 in a formal statement to the United Nations Commission on Human Rights. In 1993, the World Medical Association decided to stop medicalizing FGM/C. Other medical organizations, including the International Federation of Gynecology and Obstetrics, as well as governmental and non- governmental groups, as well as international organizations, later outlawed the operation. In a joint statement issued by WHO, UNICEF, and UNFPA in 1997, as well as an interagency statement on the elimination of FGM/C in 2008, this desertion was highlighted once more [14].
Medicalized cutting is largely carried out by doctors in Egypt, rather than other health workers, and has its origins in a 1994 Ministry of Health edict requiring state hospitals to set aside one day per week for trained physicians to perform FGM/C [15, 16, 17, 18]. Medical care practitioners continue to perform medicalized FGM/C although it is against the law in Egypt for several reasons, including financial gain; the conviction that they could conduct it safely, or because they are encouraging the continuation of FGM/C [19]. In the present study, the procedure of FGM was commonly performed at home, in agreement with other studies [20, 21, 22, 23, 24]. The Legislative Position on Female Genital Mutilation in Egypt: When the Child Law was amended by Law No. 126 of 2008; the text of Article 242 was added to the Penal Code to toughen the punishment for an intentional wound if it occurred through “female circumcision.” The new law contains two important articles. Article One: A number of recent legal amendments to the article of the Penal Code relating to female genital mutilation were approved in accordance with Law No. 78 of 2016, which was published in the Official Gazette on September 26, 2016. Article 242 bis of the Penal Code reads: “A penalty of imprisonment for a period of no less than five Years and not more than seven years for anyone who performs female circumcision by partially or completely removing any of the external genitalia or inflicting injuries on those organs without medical justification”. Article Two: It added to the Penal Code an updated text for the first time, which is the text of Article 242 (a). Anyone who promotes encourages, or calls in one of the ways set forth in Article (171) of this law to commit the crime of female circumcision, even if there is no effect from his action, shall be punished by imprisonment (Replaced by Law No. 10 of 2021 published in the Official Gazette on 4/28/2021).
Aim of the Study
The present study was carried out to assess Females’ Intention to practice Female Genital Mutilation for their Daughters at Beni-Suef.
Research Questions
Are Females at Beni-Suef intended to practice Female Genital Mutilation for their Daughters?
Subjects and Methods
Research Design
A Descriptive Cross-sectional study was used to achieve the aim of the current study.
Subjects & Setting
Setting
The study was conducted in ten family health centers (FHCs) in different sitting at Beni-Suef Governorate as the following mention: Salah Salem MCH Eastern MCH Taha Bosh MCH Beba Medical Center Tarshoup MCH Bani Saleh MCH Al-shantour MCH El- Mamalik MCH Elnouira MCH Kamen El-Arouse MCH Sample Sample Type A Convenient sample was used.
Sample size
The study population consisted of all females who were accepted to participate in the study at the time of data collection (A period of six months from the start of data collection) and will be included in the study.
Tools of Data Collection
A pre-designed structured questionnaire was used to collect data. Data were collected through personal interviews. The questionnaire is divided into three sections:
- Section I: А Structured Interviewing Questionnaire sheet which includes knowledge regarding complications Female Genital Mutilation/Cutting.
- Section II: Intention to practice FGM/C: It included questions about the following:
- Section III: Reasons for practicing FGM/C and reasons for refusing FGM Section.
Validity & Reliability of the Tool
The tool was reviewed by a panel of three experts in women health and obstetric nursing to examine their face and content validity. Modification of the content and rephrasing of some statements were done according to their recommendations. The reliability of the attitude scales was examined through assessing their internal consistency, and they showed a good level of reliability as shown by their Cronbach alpha coefficients.
Ethical Considerations
The researchers obtained required ethical and administrative approvals to conduct the study. The aim and process of the study were explained to each potential participant woman, and their oral informed consent was obtained before any data collection. They were informed about their rights to refuse or withdraw from the study at any time. They were reassured about the confidentiality of any obtained information. Professional help was provided to women when needed.
Pilot Study
A pilot study was conducted on approximately 10% of the samples of women to test the clarity and applicability of the data collection tools, and to determine the time required to fill them. The data collection forms were finalized based on the pilot results.
Field Work
Data were gathered over six months beginning in November 2021 and ending in April 2022. The researcher was present at the previously mentioned location until the entire sample size was gathered. Before data collection, the researcher introduced herself to the women and explained the purpose of the study.
Statistical Analysis
All data were collected, tabulated and statistically analyzed using IBM SPSS 25. Data was supplied, and appropriate analysis was performed for each parameter based on the type of data obtained.
Descriptive Statistics data were expressed as:
- Count and percentage: Used for describing and summarizing categorical data.
- Arithmetic mean (X-), Standard deviation (SD): Used for normally distributed quantitative data, these are used as measurements of central tendency and dispersion.
Analytical Statistics • Cronbach alpha and Spearman-Brown coefficients: The internal consistency of the generated tools was measured to assess their reliability.
Graphical presentation
- Data visualization was done with graphs.
- Coulum chart
- Bie in 3D chart
Results
Reveals the distribution of females according to their knowledge regarding side effects and health consequences of FGM/C. About 64% and 59.6% of females knew that FGM/C causes psychological problems and social problems, respectively, 56% had a misconception that FGM/C does not affect the woman’s sexual satisfaction. About 29.7% of participants are suffering from complications after FGM (Table 1).
| Variables | Values (no=2837) | |
|---|---|---|
| No. | % | |
| FGM causes psychological problems | ||
| No | 505 | 17.8 |
| Yes (correct) | 1816 | 64 |
| I don’t know | 516 | 18.2 |
| FGM causes social problems | ||
| No | 708 | 25 |
| Yes (correct) | 1690 | 59.6 |
| I don’t know | 439 | 15.5 |
| FGM does not affect sexual desire (late effect) | ||
| No (correct) | 1590 | 56 |
| Yes | 461 | 16.2 |
| I don’t know | 786 | 27.7 |
| Did you have complications from the mutilation? | ||
| Yes | 602 | 29.7 |
| No | 1419 | 70.3 |
Table 1: Knowledge Related To Complications of FGM and FGM Effects among the Studied Participants.
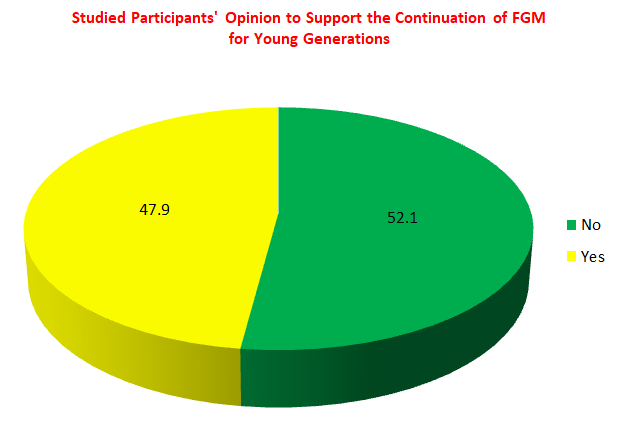
Presents the Studied Participants’ Opinion to Support the Continuation of FGM for Young Generations, and their intention to practice FGM/C for their daughters. About 47.9% of females in the study sample had the intention to mutilate their daughters and support the continuation of FGM for young generations (Figure 1).
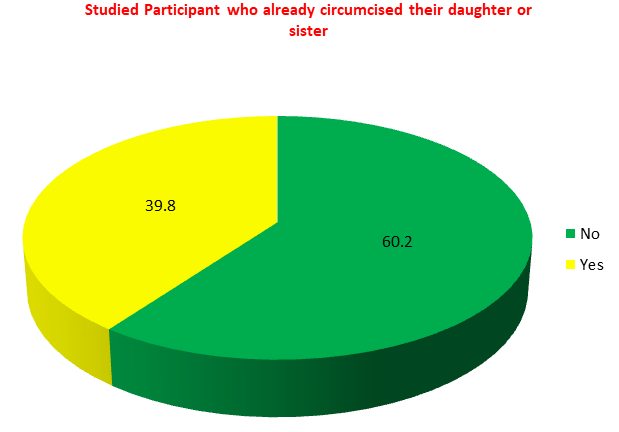
Portrays the Studied Participant who already circumcised their daughter or sister. The figure shows that 39.8% had already mutilated their daughters or sisters; with a mean age of 10.9±2.3 years (Figure 2).
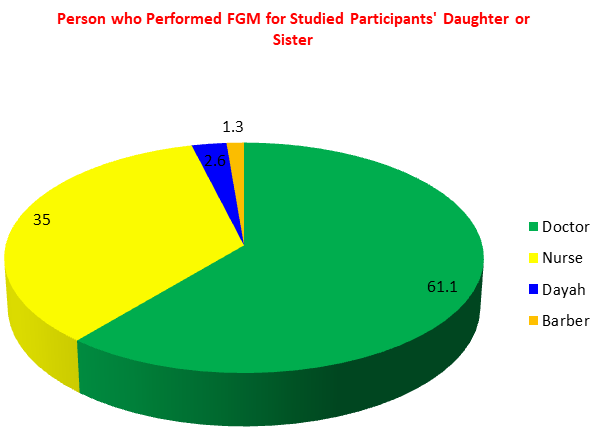
Presents the Person who Performed FGM for Studied Participants’ Daughter or Sister. The highest percent of procedures (61.1%) were performed by physicians, followed by nurses and dayah (35% and 2.6%), respectively (Figure 3).
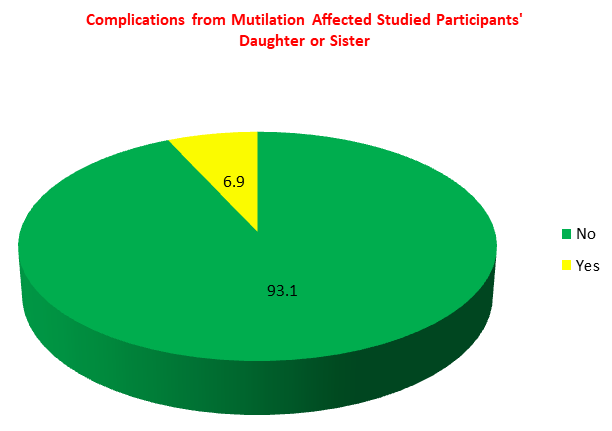
Presents Complications from Mutilation Affected Studied Participants’ Daughter or Sister. The mutilated daughters who had complications during or after the FGM/C procedure amounted to 6.9%, while 93.1% hadn’t (Figure 4).
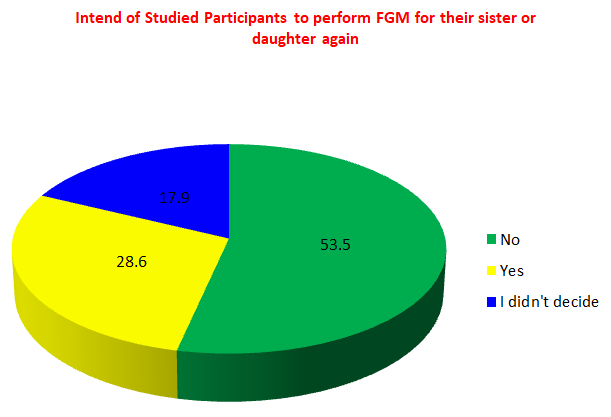
Shows Intend of Studied Participants to perform FGM for their sister or daughter again. About 28.6% of females who had mutilated their daughters were planning to mutilate their other daughters in the future (Figure 5).
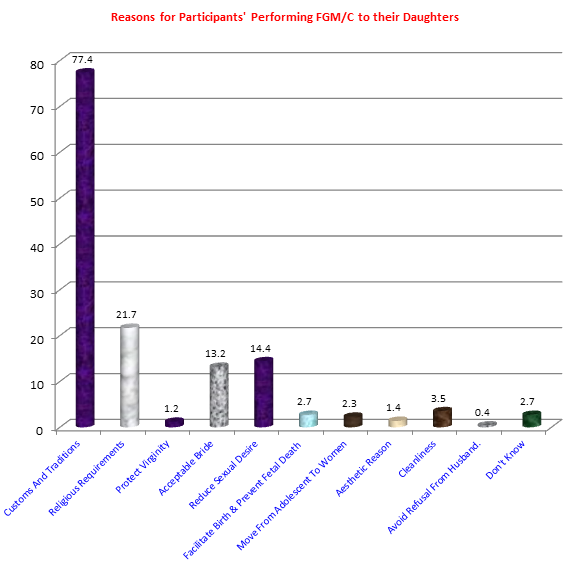
Presents Prospects of Reasons for Performing and Reasons FGM/C. Traditions and culture was the main reason for performing FGM/C as stated by females (77.4%), followed by religious requirements 21.7 %, decrease the sexual desire of females (14.4%), while 14.4% and 13.2% mentioned that they prefer FGM to reduce female sexual desire, and to be an acceptable pride, respectively. About 2.7% of females did not know the reasons for performing FGM/C (Figure 6).
Discussion
Female genital mutilation/cutting FGM/C is extensively done in societies where it is believed to promote marriageability. As a result, the practice of FGM/C will continue because parents believe it will provide a better future for their daughters, and some girls may even desire to be mutilated to find a husband. The hypothesis also suggests that in places where FGM/C is a part of the culture, no one will want to stop doing it because families are afraid of deviating from community norms [25]. Regarding females’ knowledge regarding side effects and health consequences of FGM/C, the results of the present study revealed that around two-thirds of females knew that FGM/C causes psychological problems and social problems. WHO reported that Female genital mutilation/cutting has no benefits; on the contrary, it has both physiological and psychological consequences, including short- and long-term effects [26]. The approach used to perform the procedure may influence the severity of the short-term consequences [27].
Regarding Participants’ Opinion to Support the Continuation of FGM for Young Generations, and their intention to practice FGM/C for their daughters, the results revealed that around half of females support the continuation of FGM for young generations. Moreover, they had an intention to mutilate their daughters. This attributed to most of studied female were rural residences who had culture, custom, and tradition support performing FGM/C as religious requirements, and to decrease the sexual desire of females. Also, their intention related to that she did not expose to complication or their rational that it will be performed by doctors. These reasons were comparable to those reported by many researches in Egypt [28, 29, 30, 31].
Additionally, more than one third had already mutilated their daughters or sisters; this may be attributed that they pressured by others or by their culture to practice FGM to their daughters. The highest percent of procedures were performed by physicians. This significantly greater percentage of participants underwent medically-assisted FGM or C points practice in Egypt. Egypt legalized the medicalization of FGM/C in 1994, citing the possibility of reducing the danger of health repercussions [32]. Medicines Sans Frontières (MSF) provided surgical equipment for FGM/C in 1999, claiming that it was a first-aid response to avoid complications that could arise from using non-sterile equipment.
Medicines Sans Frontières (MSF) did not support the practice but claimed that it was a first-aid response to avoid complications that could arise from using non-sterile equipment. Following the abandonment of FGM/C, the MSF issued a policy paper criticizing the practice [10]. In the most recent EHIS, the rate of medicalized FGM/C was more than doubled between mothers and daughters (38 percent and 84 percent, respectively) [33]. The Egyptian government has made many changes to the medicalization of FGM/C. It
was approved in 1994, but after a girl died during the FGM/C operation, the approval was changed in 1995. The FGM/C operation was outlawed in government hospitals, followed by private institutions, unless it was medically required. Until 2006, the medical necessity was approved. In 2007, all licensed medical care practitioners, whether public or private, were prohibited from conducting FGM/C in any hospital [14].
On the other hand, about two fifth had already mutilated their daughters or sisters. Near to one third of females who had mutilated their daughters were planning to mutilate their other daughters in the future. According to a study of female schoolteachers, in Cairo, near to one third of them mutilated all of their daughters [30]. Concerning reasons for performing and reasons FGM/C. Traditions and culture was the main reason for performing FGM/C as stated by females (77.4%), followed by religious requirements 21.7 %, decrease the sexual desire of females (14.4%), while 14.4% and 13.2% mentioned that they prefer FGM to reduce female sexual desire, and to be an acceptable pride, respectively. About 2.7% of females did not know the reasons for performing FGM/C. This was in accordance of which reported by WHO (2020). World Health Organization and UNICEF reported that he most common reasons includes; Respect for tradition FGM is usually seen as a part of the history and cultural tradition of the community [25]. Social convention where FGM is widely practiced. Marriageability there’s often an expectation that men will marry only women who have undergone FGM. Cleanliness and beauty in some communities. Religion as some communities believe that FGM may be a religious requirement and a few religious leaders may promote the practice [34].
Conclusion
Most of females knew that FGM/C causes psychological problems and social problems; however most of them had misconception that FGM/C does not affect the woman’s sexual satisfaction. Most the study sample had the intention to mutilate their daughters and support the continuation of FGM for young generations. The highest percent of procedures were performed by physicians.
Recommendations
- Motivations and behavior change of females and health care workers to perform FGM/C.
- Clarification through all available media tools about the risk of female genital mutilation aimed at behavioral change both for women and health professionals.
References
-
Johansen REB, Ziyada MM, Shell-Duncan B, Kaplan AM, Leye E (2018) Health sector involvement in the management of female genital mutilation/cutting in 30 countries. BMC Health Serv Res 18(1): 240.
-
Hassan H, Abd-ELhakam F, Ebrahim R, Mohammed M (2022) Call for Change Enhancement Upper Egyptian Females’ Knowledge Regarding Effect of Female Genital Mutilation. American J Public Health Res 10(5).
-
Abd-ELhakam F, Ebrahim R, Mohammed M, Hassan H (2022) Relationship between Socio Demographic Data and Female Genital Mutilation. Archives of Medical Case Reports and Case Study 6(4).
-
Ebrahim R, Mohammed M, Hassan H, Abd-ELhakam F (2022) Relationship between Personal Characteristics and the Person Performing Female Genital Mutilation. Journal of Community Medicine and Public Health Reports pp: 3.
-
Hassan H, Abd-ELhakam F, Ebrahim R, Mohammed M (2022) Prevalence of Female Genital Mutilation in Northern Upper Egypt. American Journal of Nursing Research 10(3).
-
Sabry HA, Elamir RY (2020) Knowledge, Attitude and Intention to Future Practice of Female Genital Mutilation among Medical Students, Egypt. The Egyptian Family Medicine Journal 4(2): 7-21.
-
Hassan H (2020) Evidence-Based Practice in Midwifery and Maternity Nursing for Excellent Quality of Care Outcomes. Am J Nurs Res 8(6): 606-607.
-
Abd-ELhakam F, Hassan H, Ebrahim R, Mohammed M (2022) Relationship between Females’ Intention of Mutilating Their Daughters and Demographic Characteristics. J Psychol Neurosci 4(3).
-
Hassan H, Abd-ELhakam F, Zakria M, El-sayed R (2022) Female Genital Mutilation in Northern Upper Egypt: Prospects of Reasons for Performing and Refusing. Int J Nurs Sci 12(1).
-
Abdou MS, Wahdan IM, El-Nimr NA (2020) Prevalence of Female Genital Mutilation, and Women’s Knowledge, Attitude, and Intention to Practice in Egypt: A Nationwide Survey. J High Institute of Public Health 50(3): 139-145.
-
Hassan H (2019) The Impact of Evidence-Based Nursing as The Foundation for Professional Maternity Nursing Practices. Open Acc J Repro & Sexual Disord 2(2): 195- 197.
-
Ebrahim R, Abd-ELhakam F, Hassan H, Mohammed M (2022) Relationship between Females’ Knowledge and Attitude and Intention of Female Genital Mutilation. Res Psychol Behav Sci 10(1).
-
Hassan H, Ebrahim R, Mohammed M, Abd-ELhakam F (2022) Female Genital Mutilation: Impact on Knowledge, Attitude, Sexual Score Domains and Intention of Females in Northern Upper Egypt. Archives of Medical Case Reports and Case Study 6(4).
-
Leye E, Eekert NV, Shamu S, Esho T, Barrett H (2019) Debating medicalization of Female Genital Mutilation/ Cutting (FGM/C): learning from (policy) experiences across countries. Reproductive health 16(1): 1-10.
-
Kimani S, Shell-Duncan B (2018) Medicalized female genital mutilation/cutting: contentious practices and persistent debates. Curr Sex Health Rep 10(1): 25-34.
-
Hassan H, Abd-ELhakam F, Ebrahim R, Mohammed M (2022) Female Genital Mutilation: Females’ Intention in Northern Upper Egypt. Journal of Obstetrics Gynecology and Reproductive Sciences 6(4).
-
ELhakam FA, Ebrahim R, Mohammed M, Hassan H (2022) Female Genital Mutilation: Relationship Association between Upper Egyptian Females’ Knowledge and Attitude. American Journal of Medical Case Reports 10(12).
-
Hassan H, Saber N, Sheha E (2019) Comprehension of Dyspareunia and Related Anxiety among Northern Upper Egyptian women: Impact of Nursing Consultation Context Using PLISSIT Model. Nursing Care Open Access Journal 6(1): 1-19.
-
Ghattass S, Tawab NGA, Hussein SA (2016) Ending the medicalization of female genital mutilation/cutting in Egypt. pp: 1-9.
-
Eldin MAT, Gadallah MA, Tayeb MNA, Aty MA, Mansour E, et al. (2008) Prevalence of female genital cutting among Egyptian girls. Bull World Health Organ 86(4): 269-274.
-
ELhakam FA, Ebrahim R, Mohammed M, Hassan H (2022) Relationship between Women’s Intention for Female Genital Mutilation and their Exposure to Complication and Pressure. Journal of Medical Case Reports and Case series.
-
Zayed AA, Ali AA (2012) Abusing female children by circumcision is continued in Egypt. J Forensic Leg Med 19(4): 196-200.
-
ELhakam FA, Ebrahim R, Mohammed M, Hassan H (2022) Female Genital Mutilation: Females’ Related Knowledge. Biomedical Research and Clinical Reviews 7(2).
-
Elwahed AYA, Ali WK, Ghattas VN (2019) Experience of Female Genital Cutting and Sexual Satisfaction Among Rural Married Women in El Beheria Governorate. International Journal of Studies in Nursing 4(1): 46.
-
UNICEF (2016) Female genital mutilation/cutting: a global concern. Geneva.
-
Young J, Nour NM, Macauley RC, Narang SK, Agbakwu CJ, et al. (2020) Diagnosis, management, and treatment of female genital mutilation or cutting in girls. Pediatrics 146(2): e20201012.
-
Klein E, Helzner E, Shayowitz M, Kohlhoff S, Norowitz TAS (2018) Female genital mutilation: health consequences and complications-a short literature review. Obstetrics and gynecology international, pp: 7365715.
-
Allam MF, Estevez JDI, Navajas RFC, Castillo ASD, Hoashi JS, et al. (2001) Factors associated with the condoning of female genital mutilation among university students. Public health 115(5): 350-355.
-
Hassan H, Ebrahim R, Mohammed M, ELhakam FA (2022) Prevalence and Determinants of Female Genital Mutilation at Beni-Suef. Current Trends in Biomedical Engineering and Biosciences.
-
ELhakam FA (2022) Prevalence of Female Genital Mutilation at Beni-Suef Governorate, Egypt.
-
Hassan H, Abd-ELhakam F, Ebrahim R, Mohammed M (2022) Study Females' Attitude toward Female Genital Mutilation. Journal of Gynecology and Women’s Health 24(3): 1-9 DOI: 10.19080/JGWH.2022.24.556137.
-
Hassan H, ELhakam FA, Ebrahim R, Mohammed M (2022) Study Females’ Attitude toward Female Genital Mutilation. Current Trends in Biomedical Engineering and Biosciences.
-
Duncan BS, Njue C, Moore Z (2018) Trends in the medicalization of female genital mutilation/cutting: What do the data reveal?.
-
Khalil AI, Orabi AM (2017) A Community-Based Intervention: Impact of an Educational Program in Exchanging Knowledge, Attitude, and Practices of Female Genital Mutilation (FGM). Health Care Current Reviews 5(4).
-
World Health Organization (WHO) (2022) Female genital mutilation, Geneva.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines