Review on the Global Public Health Issue of Antibiotic Resistance and Potential Solutions
Both industrialized and developing nations are extremely concerned about the worldwide spread of infectious diseases and the rise of antibiotic resistance. It is common for bacteria to develop resistance to antibiotics, and this phenomenon has been observed after the introduction of every antimicrobial drug into clinical practice. When bacteria adapt, the effectiveness of medications used to treat the infection is decreased or eliminated. This phenomenon is known as resistance. As a result, the germs continue to grow and cause additional damage. Due to the fact that the current antibiotics in clinical use were produced through changes to the existing classes and have demonstrated short effect cycles, a report indicated that there would be a global antibiotic shortage. The main contributing variables include population density and mobility, proper use of human antibiotics, and sub-therapeutic and excessive use of antibiotics in food animals. Manufacturers of extended-spectrum beta-lactamases and drug resistance Major concerns to global public health include Neisseria gonorrhoeae, tuberculosis, methicillin-resistant Staphylococcus aureus, and vancomycin-resistant enterococci. At the moment, antibiotic resistance places a significant clinical and financial burden. Due to the requirement for more expensive medications for the second line of therapy and significantly longer hospital stays, antibiotic resistance has a significant financial impact on the patient and family, the hospital, and society. According to the Centers for Disease Control and Prevention, antibiotic resistance causes 23,000 fatalities and over 2 million illnesses annually in the United States alone. With 27.3 deaths per 100,000 people, Africa has the highest mortality rate from AMR infections in the whole globe.
Introduction
Penicillin’s invention in the 1940s resulted in a dramatic decline in infectious disease-related sickness and fatalities. However, immediately after the drug’s introduction, patients’ isolates of penicillin-resistant bacteria were discovered [1]. The development of a bacterial strain resistant to antibiotics was recognized in the late 1950s. It later became evident that microorganisms such as Salmonella typhimurium and Salmonella Dublin which are resistant to one or more antibiotics can transfer resistance to other bacteria. Since then, numerous new antimicrobial agents have become available, many of which have been rendered ineffective by the remarkable ability of bacteria to become resistant through mutation or acquisition of resistance genes from other organisms [1, 2, 3, 4]. Disease-causing bacteria respond to drugs by developing resistance to them over time. This can happen naturally through mutations that emerge from errors made when bacteria divide and replicate their DNA. The bacteria can survive thanks to these changes. The widespread use of antibiotics in both humans and animals has sparked concerns about the emergence of drug-resistant and multidrug-resistant bacteria, which could pose a threat to both humans and animals and lead to treatment failure [5, 6]. Whenever new antimicrobial agents are developed, resistance follows, sometimes quickly, and this occurs for all antimicrobials. Furthermore, resistant bacteria pose the greatest threat to human health [7]. The rapid emergence of resistant bacteria is occurring worldwide, endangering the efficacy of antibiotics, which have transformed medicine and saved millions of lives [8]. Numerous bacteria have been identified by the Centers for Disease Control and Prevention (CDC) as posing urgent, serious, and worrying risks. Many of these bacteria are already to blame for inflicting a significant clinical and financial burden on the health care system of patients and their families. A current major worldwide public health problem is the continued rise of multidrug resistant bacteria including Extended-spectrum beta- lactamase producers, drug resistant Neisseria gonorrhoeae, Tuberculosis, Methicillin-resistant Staphylococcus aureus, and Vancomycin-resistant enterococci.
The lack of new antibiotics threatens hospitalized patients’ lives and significantly increases health care expenses, especially for patients with illnesses brought on by multidrug-resistant pathogens [9]. In Ethiopia, some studies on in human patients, food animals, foods and the environment showed increasing levels of AMR. However, as the studies are not comprehensive and difficult to compare to get the full picture of the problem. These studies had limited scope, coverage and focused on single microorganisms isolated from either human cases or foods of animal origin only. The pooled prevalence of AMR in bacteria from food producing live animals was 20%. High estimates were found in bacteria identified from milk, food handlers and the environmental samples with 29%, and 28% in meat. In foods of non-animal origin, the prevalence was lower with 13% [10]. Therefore, the objectives of this seminar paper are to examine a few key issues related to antibiotic resistance and how it is evolving, as well as to briefly discuss its present public health significance and potential remedies.
Overview of Antibiotics
In 1942, Selman Waksman and his collaborators used the term antibiotic to describe any substance produced by a microorganism that is antagonistic to the growth of other microorganisms. This definition excluded substances that kill bacteria, but that are not produced by microorganisms. It excluded synthetic antibacterial compounds such as the sulfonamides . But antibiotics are normally defined as substances which kill or inhibit the growth of a microorganism. They can be synthetic or naturally produced by other microorganisms [11]. In 1928, Alexander Fleming identified penicillin, the first chemical compound with antibiotic properties. Fleming was working on a culture of disease causing bacteria when he noticed the spores of little green mold in one of his culture plates. He observed that the presence of the mold killed or prevented the growth of the bacteria [12].
Antimicrobials are used to cure illnesses in humans, animals, and plants by eradicating or stopping the development of bacteria. Each antimicrobial kind targets a distinct anatomical feature or physiological function unique to its target bacterium. Antimicrobials can either be wide, focusing on a characteristic that all members of a group of bacteria share, or narrow, influencing a characteristic that is exclusive to one or a few species within a group. Antimicrobials that work against one species or group do not work against another species or group that does not share the targeted characteristic.
Several antibiotics are also effective against fungi and protozoans, and some are toxic to humans and animals, even when given in therapeutic dosage. Antibiotics are not effective against viruses such as the common cold or influenza, and may be harmful when taken inappropriately [8]. Antibiotics are screened for any negative effects on humans or other animals before approval for clinical use, and are usually considered safe and most are well tolerated. However, some antibiotics have been associated with various adverse side effects that range from mild fever and nausea to severe major allergic reactions; depending on the antibiotics used, the dosage, and the individual patient. Safety profiles of newer drugs are often not as well established as for those that have a long history of use [1]. The successful outcome of antimicrobial therapy with antibacterial compounds depends on several factors. These include host defense mechanisms, the location of infection, and the pharmacokinetic and pharmacodynamics properties of antibacterial gents [13].
Antibiotic Resistance
AMR is a naturally occurring process, which arises when a pathogenic microbe pathogen has a genetic mutation that significantly alters an aspect of its anatomy or physiology, allowing it to evade or resist the action of an antimicrobial medicine [6] or acquisition of resistance genes from other organisms [1, 2, 3, 4]. The resistant strain therefore survives exposure to the antibiotic, where other strains without this mutation do not. The genetic advantage can then be passed on when the resistant microbe replicates and divides itself or, in some instances, between species through horizontal gene transfer . An infected individual or host human, animal, or plant can spread their anti-microbial resistant strain to others, via direct or indirect transmission, e.g. between animals and humans by direct contact, via food products or the environment [14]. In time, the resistant strain becomes the most prevalent in the species, rendering the antimicrobial medicine widely ineffective.
Mechanisms of Resistance
Microorganisms develop resistance by various mechanisms and resistant genes are incorporated in the organism and genetic transfer of resistance occurs [15]. Infection caused by resistant microbes fails to respond to treatment and selection of resistant strains occurs. As far as mechanisms of resistance are concerned, some bacterial species are normally insensitive to certain antibiotics, whereas others are sensitive. Resistance may be natural or acquired. Natural is whereby microorganisms naturally do not possess target sites for the drugs and therefore the drug does not affect them, or they naturally have low permeability to those agents because of the differences in the chemical nature of the drug and the microbial membrane structures, especially for those that require entry into the microbial cell in order to affect their action [3, 16]. Acquired resistance is described as whereby a naturally susceptible microorganism acquires a way of not being affected by the drug. Bacteria in many environments can readily exchange genes coding for antibiotic resistance with neighboring bacteria. This can occur through spontaneous mutations, the result of mistakes when bacteria copy their DNA as they divide. Mutated genes allow bacteria to survive and pass on to successive generations. Antibiotic resistance genes are often located on mobile genetic elements, especially plasmids, transposons and interferon which can easily move between bacteria of the same or different species and facilitate the spread of resistance to multiple drugs by multiple types of bacteria [2, 3, 4, 17].
A plasmid, which is a circular chunk of bacterial DNA that exists naturally inside many bacterial cells, may contain genes that confer antibiotic resistance. The plasmids are spread to other bacterial cells by different mechanisms such as transformation, transduction, conjugation and transposition. Transformation of genetic material occurs when a bacterium dies, at which point it breaks up and releases its DNA into its environment. Nearby bacteria can pick up bits of this free floating DNA and integrate it into their own genomes, creating a potential pathway for antibiotic resistance dissemination. Transposition is when a segment of DNA that has a repeat of an insertion sequence element at each end that can migrate from one plasmid to another within the same bacterium, to a bacterial chromosome, or to a bacteriophage. The mechanism of the transposition seems to be independent of the host’s usual recombination mechanism. Conjugation is when two bacteria are near each other, genetic material can be passed directly between cells, or via a hollow structure called a pilus, or a pore, that can form between the two cells. Plasmids can use this pilus like a bridge, sending copies of themselves to the other cells [18].
Source: (SGM, 2015) [18] Figure 1: Conjugation.
Transduction occurs when a virus attacks a bacterium and takes over the cell to make copies of its own. Sometimes, bits of bacterial DNA are included in the DNA of the virus particles produced. The viruses then carry these chunks of bacterial DNA to other bacteria they infect [18].
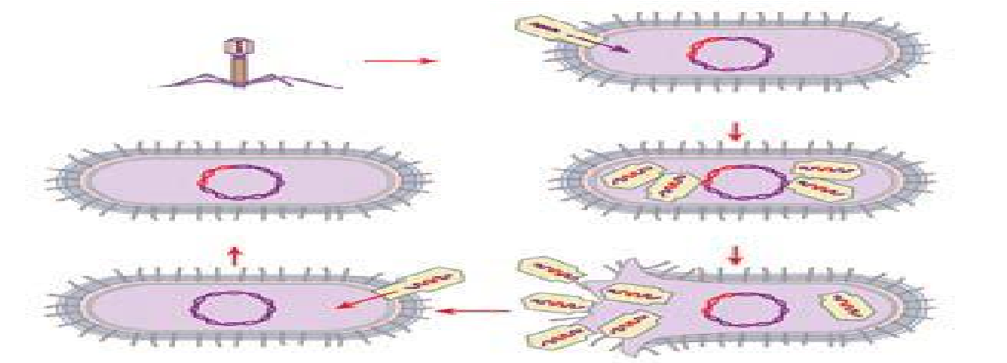
Source: (SGM, 2015) [18] Figure 2: Transduction.
Efflux pumps remove antibiotics from cells; modifying enzymes alter the drug’s structure; and degrading enzymes completely break down the antibiotic. These are some strategies used by plasmids to cause resistance. The minimal inhibitory concentration that prevents bacterial growth is used to determine the bacterial sensitivity to antibacterial agents [15].
Contributing Factors for the Occurrence of Antibiotic Resistance
Population density and mobility: Without continued cooperation from regional and international partners, no one country can effectively identify, manage, and prevent antibiotic resistance inside its boundaries [19]. The potential for the emergence and rapid spread of new or variant forms of known pathogens has increased as a result of factors including highly mobile populations, the ease of expanding international trade and travel, high density populations, the expansion of industrial agricultural practices, environmental changes, ongoing pathogen evolution, and increasingly complex health care treatments. These factors also present a variety of new challenges to clinicians, microbiologists, and public health officials. The pace and volume of international travel nowadays opens up new channels for the transmission of viruses that are resistant to antibiotics, as is the case with all infectious illnesses.
Faulty usage of antibiotic in Human Medication: Antibiotic usage is definitely a factor in the development of resistance. Epidemiology research has shown a link between the use of antibiotics and the establishment and spread of bacterial strains that are resistant to treatment. Genes in bacteria can be inherited from close relatives or acquired from unrelated individuals via mobile genetic components like plasmids. With this horizontal gene transfer (HGT), antibiotic resistance may spread between several bacterial species. Moreover, resistance can evolve on its own through mutation. Drug-sensitive rivals are eliminated by antibiotics, leaving drug-resistant microorganisms remaining to proliferate through natural selection. Despite recommendations against excessive usage, antibiotics are widely prescribed globally [20].
Hoarding: The act of skipping doses of prescription antibiotics may not have a significant impact on the patient’s immediate clinical prognosis. Yet, when the remaining course material is “hoarded” in anticipation of a foreseeable need, there is a far higher risk of applying antimicrobial treatment incorrectly to organisms that are not sensitive to it. People can fail to entirely rid their bodies of a bacterial illness by not taking the recommended number of medicines for the recommended duration of time. As some of the surviving bacteria were exposed to the antibiotic but were not entirely killed by it, this incomplete removal of the infection increases the likelihood that some of them would acquire antibiotic resistance [21, 22].
Inappropriate prescription: Inappropriate prescribing methods are influenced by a lack of understanding regarding differential diagnosis, infectious illnesses, microbiology, and the proper selection of antibiotics for diverse infections. The pharmacology of antibiotic drugs, their mechanisms of action, range of activity, and concerns linked to resistance receive little attention in medical school curricula, even in industrialized nations, leaving prescribers with inadequate knowledge. Thus, global collaboration and coordinated efforts to inform the public about drug resistance and the consequences of incorrect antibiotic usage will be necessary to control antibiotic resistance on a larger, international scale [21, 23].
Non-prescription purchase: Access to controlled antimicrobials is not universal. Antimicrobials are produced and sold in numerous nations with little or no regulation. As a result, medicinal products of wildly varying quality are produced and made widely and inexpensively available to the general population. Before the Internet, only returning tourists could get such supplies of antimicrobials in first- world nations [24]. Outside the United States and Europe, the non-prescription usage of antibiotics can range from 19 to well over 90% [19]. 88% to 91% of all antibiotic sales in Vietnamese pharmacies, including urban and rural, occurred without a prescription in 2010.
Faulty usage of Antibiotic in food animals: Since roughly 70 years ago, there has been a significant usage of antibiotics in animal feed, and in 2019 over 11,000 tons of antibiotics were administered to farm animals [25].
Most antibiotics are administered to animals in Africa, the European Union, and the United States in order to enhance animal development and avoid bacterial illness [26].
In 2030, it is expected that the amount of antibiotics used on animals for food would rise by 11.5% (to 200,235 tons) [27]. The body excretes around 75% of antibiotics that are not absorbed by animals through feces and urine, which can pollute and harm the environment [28]. Meanwhile, improper or excessive use of antibiotics in animal agriculture has produced a variety of antibiotic-resistant organisms (ARO) and antibiotic resistance genes (ARG), which can spread between people and animals [3]. There is mounting evidence that the widespread use of nontherapeutic antibiotics in animals is primarily responsible for human antibiotic resistance. Animal farms are a huge source of ARB and ARGs, which is one of the new worldwide concerns for dangers to both human and animal health [29]. Including beta-lactams, aminoglycosides, tetracycline, sulfonamide, macrolide-lincosamide streptogramin-B fluoroquinolone, quinolone, florfenicol, chloramphenicol, and amphenicol, as well as vancomycin, colistin, and multidrug, respectively, this ARB and there carried mobile ARGs confer resistance to nine major antibiotic classes [30]. Moreover, discovered that the transmission of mobile ARGs, notably concentrated in Proteobacteria, Bacteroidetes, Actinobacteria, and Firmicutes, is primarily responsible for the spread of antibiotic resistance between farm animals and humans, humans shared more ARGs with chicken than with other animals (such pigs and cattle) from other nations, and these common ARGs between animals and people confer resistance to chloramphenicol, MLSB, and sul [30].
Increased infections that are hardly ever treated with antibiotics may be caused by a variety of exposure pathways for ARB and ARGs from farms to humans, including direct or indirect contact with animals, manure, or products as well as inhalation of bio aerosol that contains them [31].
Some ARBs (such as Staphylococcus spp., Escherichia coli, Salmonella, etc.) and ARGs can be transferred to humans by direct contact with animals, exposure to animal feces or wastewater, and consumption of contaminated animal food products [31]. Additionally, airborne ARB and ARGs have also been frequently detected in the farms, and the abundance of some ARGs in farm bio aerosols are up to 2.3
10.6 log copies/m3 [29]. Recent work by showed that Staphylococcus, Acinetobacter, and Sphingomonas were identified in farm airborne; numerous ARGs were dispersed from the animal farms to a distance of 10 km. Multidrug-resistant (MDR) bacteria (including Staphylococcus spp., Enterococcus spp., Salmonella spp., E. coli, etc.) and ARGs were transferred to workers and residents in the surrounding environment via inhalation, thus, posing the risk of diseases [4].
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \frac {1}{2} \mathrm {B} ^ {2} + \frac {1}{2} \mathrm {C} ^ {2} $$
Trend of Major Threat Resistant Bacteria
Extended-Spectrum Beta-Lactamase Producers
Extended-spectrum beta-lactamases (ESBLs) are a family of enzymes, produced by Gram-negative bacteria that confer resistance to some of the world’s most widely prescribed antibiotics [9]. ESBLs can inactivate all penicillin and cephalosporin, including third generation cephalosporin (e.g., ceftriaxone, cefotaxime, and ceftazidime) and monobactams (aztreonam [32]. In Europe, 17 countries reported that 85 to 100 percent of E. coli isolates were ESBL positive, and for K. pneumoniae, 13 countries reported ESBL percentages in the same range . In the United States, 14 percent of E. coli isolates and 23 percent of K. pneumoniae isolates were found to be ESBL-producer [11]. In New Zealand, ESBL-producing Enterobacteriaceae incidence increased from 10 people per 100,000 populations in 2000 to 2013 per 100,000 in 2013.
In Australia, 7 percent of E. coli and 5 percent of K. pneumoniae isolates were found to be ESBL producers [33]. In 2009 and 2010, 28% of all Enterobacteriaceae from urinary tract infections in 11 countries in Asia were ESBL producers, and resistance to third- and fourth-generation cephalosporins ranged from 26 to 50 percent. In Latin America in 2014 resistance in K. pneumoniae ranged from 19% in Peru to 87% in Bolivia. In sub-Saharan Africa, the median prevalence of resistance to third-generation cephalosporin ranged from 0 to 47 percent. In Central Africa, the prevalence of ESBL was found to be 55 to 83 percent from the hospital samples. In West Africa, ESBLs were detected in 10 to 40 percent of hospital samples and 10 to 96 percent of community samples [34] Antibiotic-resistant Neisseria gonorrhoeae Gonorrhea is a sexually transmitted infection, mainly of the reproductive tract, caused by the bacterium N. Gonorrhoeae. According to WHO 106 million new cases of gonorrhea occurred worldwide in 2008 alone. Neisseria gonorrhoeae has developed resistance to several former first-line antibiotics, including sulfonamides, penicillin, tetracycline, and fluoroquinolones. Currently, treatments of choice are third generation cephalosporin (parenteral ceftriaxone and oral cefixime), the last remaining option for single-drug treatment. However, treatment failures have been reported from different part of the world as to third- generation cephalosporin has been declining in several parts of the world [11].
Several countries have reported treatment failures with oral cephalosporin (cefixime), and there are now some verified reports of treatment failure with the parenteral cephalosporin (ceftriaxone) in patients with gonorrhoea. The gonococcal strains causing those clinical failures were resistant to most other antibacterial drugs relevant for treatment, and have been classified as multidrug-resistant gonococci or even extensively drug-resistant gonococci. It is anticipated to be only a matter of time before gonococci with full resistance to the third-generation extended spectrum cephalosporin emerge and spread internationally. Consequently, gonorrhoea may become untreatable. There are 36 countries that report decreased susceptibility to third-generation cephalosporin’s [6].
In Europe the proportion of resistance to third generation cephalosporin was found to be 0–36 % [9]. In the United States, decreasing susceptibility to cefixime prompted the CDC to change treatment guidelines to dual therapy in 2012 [11]. In Canada, resistance has been on the rise, and 4 percent of isolates showed decreased susceptibility to a cephalosporin in 2013 [35]. Carbapenem-resistant Enterobacteriaceae (CRE) Carbapenems, the most broad-spectrum betalactam antibiotics active against Gram-negative organisms, are very slowly hydrolyzed by most beta lactamases. Because of this, agents from this class have been used successfully and have served as the last line of defense against multidrug-resistant Gram-negative organisms since their introduction in the early 1980s. Carbapenems used for infections that are resistant to first, second and even third-line antibiotics. Infections with CRE are increasingly reported from health care facilities around the world [36]. In 2012, 11%and 2% of Klebsiella spp. and E. coli isolates were resistant to carbapenems respectively in the United States. CRE isolation has been associated with all-cause hospital mortality ranging from 29% to 52% [11]. In 2013, resistance of K. pneumoniae to carbapenems in the Dominican Republic found to be 28%. In India, 10 % of E. coli isolates were resistant to carbapenems in 2008, increasing to 13 % in 2013. For K. pneumoniae, 29% were resistant in 2008, increasing to 57 % in 2014 [37].
Drug resistance Tuberculosis
Tuberculosis remains a major global health problem, responsible for ill health among millions of people each year. Tuberculosis ranks as the second leading cause of death from an infectious disease worldwide. Tuberculosis is caused by the bacterium Mycobacterium tuberculosis. Mycobacteria grow only slowly; consequently, culture in the laboratory, which is necessary to study resistance to anti-TB drugs, is difficult. Also, Mycobacteria can survive inside the body’s immune defense cells, which is one of the reasons for the long duration of tuberculosis treatment. Despite the progress in prevention and treatment of tuberculosis in recent years, 8.7 million people developed tuberculosis in 2012, and 1.3 million died as a result of the disease. The development of resistance to anti-TB drugs began shortly after the initial introduction of antibacterial drugs for the treatment of tuberculosis. Globally, 3.5% of new and 20.5% of previously treated TB cases was estimated to have had MDR-TB in 2013. This translates into an estimated 480, 000 people having developed MDR-TB in 2013 [9]. Methicillin-Resistant Staphylococcus Aureus (MRSA) MRSA was first identified five decades ago. Since then, MRSA infections have spread worldwide, appearing at a high incidence in several countries. MRSA is a common pathogen responsible for skin and soft tissue infections, severe bloodstream infections, and pneumonia. MRSA was once a predominantly hospital acquired infection but in recent years has been increasingly found in community- onset infections. The proportion of S. aureus that is resistant to methicillin has declined in Europe and the United States over the past eight years, from 22 to 18 percent and from 53 to 44 percent, respectively (EARS-Net, 2014; CDDEP, 2015). MRSA rates have also declined in Canada, from 21 to 16 percent since 2009, particularly in hospitals. In Australia, MRSA prevalence increased from 12 percent in 2000 to 19 percent in 2013 [33]. In Africa, MRSA prevalence still on the rise, it ranges from 12 -80% but it has decreased since 2011 in South Africa (from 34 to 28 percent) [37].
Vancomycin-Resistant Enterococci and Drug Resistance Nontyphoidal Salmonella
Vancomycin-resistant enterococci (VRE) and are another high-priority pathogen whose presence has grown enormously over the past few years. The first isolates were discovered in 1987. In Europe in 2013, the E. faecium vancomycin resistance range was found to be 0-43%. In United States 25 percent of Enterococcus blood stream infections is in hospitals. By 2013, 77 percent of E. faecium infections in the United States were resistant to vancomycin [11]. In New Zealand, Vancomycin resistance among Enterococcus spp. increased from 0.3 percent in 2002 to 2 percent in 2013. Similarly, in Australia in 2013, 41 percent of E. faecium bloodstream isolates were vancomycin resistant [37]. Most Salmonella strains cause gastroenteritis, while some strains, particularly Salmonella enterica serotypes Typhi and Paratyphi, are more invasive and typically cause enteric fever. Enteric fever is a more serious infection that poses problems for treatment due to ABR in many parts of the world. Multidrug resistance has also been increasingly detected in Salmonella enterica serotype. For instance, Salmonella enterica Typhimurium carries the genomic element that resistance to five antimicrobials (ampicillin, chloramphenicol, streptomycin, sulfonamides and tetracycline) [9, 39].
Global Health and Economic Burden of Antibiotic Resistant Bacteria
Antimicrobial resistance (AMR) is a global public health concern, with the World Health Organization designating it a leading health threat [6]. The 2022 GRAM Global Burden Report, calculated bacterial AMR to be associated with 4.95 million deaths in 2019, including 1.27 million attributable deaths, placing AMR as a leading cause of mortality globally. This data updates the 2016. Moreover, which then estimated the yearly AMR attributable deaths to be 700 000 [39]. The Global Burden Report also presented regional AMR mortality, as well as the leading pathogens associated with resistance. Within the European Union (EU)/European Economic Area (EEA), a study using data from 2015, showed bacterial AMR to be responsible for 33 000 deaths that year [16]. Studies from Tanzania and Mozambique indicate that resistant infections result in increased mortality in neonates and children under five [40]. Invasive nontyphoidal Salmonella infections are responsible for more than 600,000 deaths per year, 55 percent of them in Africa [41]. The consequences are already being felt by health services, as patients with antimicrobial resistant infections are often hospitalized for longer, require more expensive medicine courses, and are more likely to have worse health outcomes, with some infections untreatable. Vulnerable groups, such as preterm infants and the immunocompromised, have an additional risk due to their increased susceptibility to infections generally [42]. AMR also threatens outcomes of surgical, medical, and dental treatments, putting patients at increased danger of serious complications, including disability and death, if they acquire antimicrobial-resistant infections during the treatment process Compounding the situation are issues including a lack of new antimicrobial medicines being developed, due to a lack of viable market; problems of access – financially and practically; and quality of existing antimicrobials. A 2017 WHO report confirmed that the entire world would be run out of antibiotics, as the existing drugs in clinical use were developed through modifications to the existing classes, and have shown to have short impact cycles [43]. However, the direct replacement of antimicrobials only offers a short-term solution. The establishment of long-term preventative measures, under an inter-sectoral One Health approach considering human, animal, plant, and environmental aspects – is essential to ending the crisis [6].
Alternative Solutions
Bacteriophage Therapy
Bacteriophages are bacterio-specific viruses that interact only with bacterial cells or prokaryotes. The bacterial biochemical machinery that enables the interaction of bacteriophages and bacterial cells does not exist in the cells that constitute our bodies or eukaryotic cells. This is why bacteriophages are bacterio-specific and non- interactive with our body cells and in principle it is safe to use. One advantage of bacteriophages over antibiotics is their availability and thought to be the most abundant organisms on Earth; they are so diverse that no two identical phages have ever been found. This means that the bacterial hosts and phage co-evolve so when bacteria become resistant to a phage the phage will often evolve to re-infect it [44]. The bacteriophage injects its genomic material (composed of a nucleic acid) into the bacterial cell where it can be amplified. This results in the production of many of newly formed bacteriophages that will spread to other bacteria after the infected bacterium is lysed. This bacterium killing process is independent of the bacterium’s antibiotic resistance status. This means that, as well as a sensitive pathogen, a resistant pathogen will also be killed by the bacteriophage.
Vaccines
Vaccines are considered among the most cost-effective ways to prevent morbidity and mortality from infectious diseases. Indeed, vaccines against infectious diseases have had a huge impact on human health in the last 50 years by controlling, and in some cases eradicating, many diseases, both viral (for example, smallpox, measles and polio) and bacterial (for example, diphtheria and tetanus) that were the cause of much death and disability in the 20th century. Vaccines potentially provide a major means of limiting the clinical impact of emerging antibiotic resistance. Vaccines that prevent bacterial infections directly reduce the need for antibiotics. The vaccines in widespread use today are true public health interventions which also intended to reduce overall morbidity and mortality; the reductions in antibiotic use and resistance are also side benefits [11]. The first category is vaccines that prevent bacterial infections commonly acquired by the general population, often called ‘Community- acquired infections’. These vaccines prevent bacterial infections, thereby protecting individuals, while also negating the need for antibiotics, reducing the opportunity for bacteria to develop resistance, E.g. Diphtheria and tetanus. The second category is vaccines that would prevent bacterial infections commonly acquired in hospital, often called hospital-acquired infections’. Hospitals are where many fatal resistant infections often develop. Rather than being used across large sections of the population, such vaccines might typically be used on a more targeted basis amongst particularly high-risk populations [43]. These infections are often caused by bacteria such as S. aures and E.coli. The third category is vaccines that prevent viral infections From the perspective of bacteria becoming resistant to antibiotics, these vaccines are important because a large proportion of unnecessary prescribing of antibiotics occurs for patients who have viral infections, even though the drugs will not help in these cases E.g. flu. The fourth category is vaccines to prevent infections in animals, particularly farm animals, where a large volume of antibiotics are used. These can protect livestock and fish from infection, reducing the need for prophylactic and therapeutic antibiotic use [9].
Improved Diagnostic Tools
The most powerful weapon directed at antibiotic resistance is techniques for the rapid and accurate identification of bacteria and determination of their susceptibility to antibiotics. Health care providers need rapid diagnostic tests that can distinguish between bacterial and viral infections, between bacterial infections that require treatment with antibiotics and those that do not, and between bacteria with susceptible and resistant strains to certain antibiotics. Such tests would have the potential to improve both antibiotic prescribing and patient outcomes [5, 45]. Limiting the Spread of Drug Resistant Bacteria Prevention of infection should be the primary goal to improve health and reduce the need for antibiotic therapy [9]. Several measures could be used to prevent the spread of drug resistant bacteria. First, it is better to use appropriate treatment strategies; better immunization programs; improved hygiene and nutrition; and initiatives targeting the poor populations. Second, it might be useful to establish antibiotic resistance surveillance programs. Third, better education of health care professionals is required to prevent the prescription of unnecessary antibiotics. It is not worthy that significant investment of time, effort, and money is necessary in order to control the spread of antibiotic resistant bacteria. But as long as antibiotics are used, antibiotics resistance is bound to occur. However, we might be able to reduce the drug resistance problem [7, 11]. Development of New Antibiotics Another possibility is to develop new antibiotics. However, this is not an easy task. Identification of new antibiotics presents a challenge to the drug discovery sector because it is difficult to identify new compounds with antibacterial activity. There has been a significant decline in the rate of identification of new antibacterial compounds since the 1970s. For instance, Isolation of new antibiotics from soil has also become more difficult as many soil bacteria produce similar range of antibiotics. Most of the antibiotic classes currently in use were identified in the golden era of antibiotic discovery between 1945 and 1960 and only few new classes of antibiotic have been discovered in the past 50 years. This indicates how it is difficult to create new classes of antibiotics [6]. Promote Antibiotic Resistance Surveillance Surveillance involves the systematic collection and analysis of health related data, and dissemination to those who will use them in decision making on public health issues. The surveillance of antimicrobial are used tracks both how much antimicrobials are being used and how they are used by patients and health-care providers. Use of Bacteriocins as Human Therapeutics Bacteriocins are proteins produced by bacteria that are toxic to similar or closely related bacteria. Bacteriocins that attack pathogens and are produced by bacteria that are harmless to us would make ideal antibiotics. A number of bacteriocins are now being studied for potential use as antibacterial medication. They are also increasingly used to prevent the growth of dangerous bacteria in food, extending shelf life and delaying food spoilage [31]. Promoted Herbal Medication Medicinal plants are part and package of human society to fighting against diseases from the dawn of civilization. Medicinal plants are rich sources of antimicrobial agents. Plants are used medicinally throughout the world and are the source of potential and powerful drugs. Antimicrobial properties in plants are attributed to the presence of active compounds, e.g., quinones, phenols, alkaloids, flavonoids, terpenoids, essential oil, tannins, lignans, glucosinolates and some secondary metabolites. Other antimicrobial agents of plants include the peptides forming their defense systems which are similar to human antimicrobial peptides in structure and function. The herbal products today indicate safety in distinction to the synthetics that are regarded as dangerous to human and environment [30]. Due to the overuse of prescription antibiotics which can lead to the development of antibiotic-resistant strains of bacteria, many medical experts are taking a new look at natural, safe antibiotic alternatives. There are a number of natural herbal antibiotics that should be studied and keep on hand repeatedly. To battle against any kind of infection or illness, medicines prepared from the natural herbs can be used which are relatively inexpensive, and can be stored for a year or more at room temperature [45].
Conclusion and Recommendations
Antibiotic resistance now has been universally identified as public health priority and necessary plan of action is needed to combat this resistance. The development of antibiotic resistance is a natural phenomenon in microorganisms, and is accelerated by the selective pressure exerted by overuse and misuse of antibiotic agents both in humans and animals. It is beyond the ability of any one country to detect, control and prevent ABR within its own borders without ongoing engagement of regional and global partners. Extended- spectrum beta-lactamase producers, Antibiotic-resistant Neisseria gonorrhoeae, Drug resistance Tuberculosis Methicillin-resistant Staphylococcus aureus (MRSA), Vancomycin-resistant enterococci and drug resistance nontyphoidal Salmonella are currently causing serious public health threat. The economic and public health burden of resistant bacteria is enormous and it is serious threat of the world. Therefore it needs urgent and coordinated effort to compact the crisis posed by resistant bacteria. Based on the above conclusions the following recommendations are forwarded:
- Awareness should be created on the appropriate use of antibiotics
- Research on plant-based drugs should be increased
- Strong surveillance and reporting systems should be developed on the use and regulations of antibiotics
- Sustainable investment should be encouraged, and strong control strategies of bacterial infection should be implemented.
References
-
Nesme J, Cécillon S, Delmont TO, Monier JM, Vogel TM, et al. (2014) Large-scale metagenomic-based study of antibiotic resistance in the environment. Current Biology 24(10): 1096-1100.
-
He Y, Yuan Q, Mathieu J, Stadler L, Senehi N, et al. (2020) Antibiotic resistance genes from livestock waste: occurrence, dissemination, and treatment. NPJ Clean Water 4: 1-11.
-
Liu ZH, Wang K, Zhang YR, Xia LN, Zhao L, et al. (2022) High prevalence and diversity characteristics of blaNDM, mcr, and blaESBLs harboring multidrug-resistant Escherichia coli from chicken, pig, and cattle in China. Front Cell Infect Microbiol 11: 755545.
-
Yang L, Shen YB, Jiang JY, Wang XY, Shao DY, et al. (2022) Distinct increase in antimicrobial resistance genes among Escherichia coli during 50 years of antimicrobial use in livestock production in China. Nat Food 3: 197- 205.
-
Bloom G, Wolcott S (2013) Building institutions for health and health systems in contexts of rapid change. Social Science and Medicine 96: 216-222.
-
WHO (2021) Factsheets: Antimicrobial Resistance.
-
Silver LL (2011) Challenges of antibacterial discovery. Clinical Microbiology Review 24(1): 71-109.
-
Golker Z, Bagasra OP, Donald G (2014) Bacteriophage therapy a potential solution for the antibiotic resistance crisis. Journal of Infection in Developing Countries 8(2): 129-136.
-
WHO (2014) Antimicrobial resistance: global report on surveillance. Geneva.
-
Gemeda BA, Megarsa AA, Jaleta B, Amenu K, Wieland B (2021) Antimicrobial resistance in Ethiopia 2021: A systematic review and meta-analysis of prevalence in foods, food handlers, animals, and the environment. One Health 13: 100286.
-
CDC (2013) Antibiotic resistance threats in the United States, Atlanta.
-
Spellberg B, Gilbert DN (2014) The future of antibiotics and resistance: a tribute to a career of leadership by John Bartlett. Clinical Infectious Disease 59: 71-75.
-
European Commission. Public Health. EU Action on Antimicrobial Resistance.
-
Morel C (2019) Transmission of antimicrobial resistance from livestock agriculture to humans and from humans to animals. OECD Food, Agriculture and Fisheries Papers, No. 133.
-
Kumar S, Varela MF (2012) Biochemistry of bacterial multidrug efflux pumps. International journal of molecular sciences 13(4): 4484-4495.
-
Alessandro C (2018) Attributable deaths and disability- adjusted life-years caused by infections with antibiotic- resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. The Lancet-Infections Diseases 19(1): 565-566.
-
Marshall BM, Levy SB (2011) Food animals and antimicrobials: Impacts on human health. Clinical microbiology reviews 24(4):718-733.
-
SGM (2015) Antibiotic resistance: a challenge for the 21century.
-
Morgan DJ, Okeke IN, Laxminarayan R, Perencevich EN, Weisenberg S (2011) Non-prescription antimicrobial use worldwide: a systematic review. The Lancet infectious diseases 11(9): 692-701.
-
Luyt CE, Brechot N, Trouillet JL, Chastre J (2014) Antibiotic stewardship in the intensive care unit. Critical Care 18(5): 480.
-
Michael CA, Dominey Howes D, Labbate M (2014) The antibiotic resistance crisis: causes, consequences, and management. Front Public Health 2: 145.
-
Bbosa GS, Mwebaza N, Odda J, Kyegombe DB, Ntale M (2014) Antibiotics/antibacterial drug use, their marketing and promotion during the post-antibiotic golden age and their role in emergence of bacterial resistance. Health 6(05): 410.
-
Bartlett JG, Gilbert DN, Spellberg B (2013) Seven ways to preserve the miracle of antibiotics. Clinical Infectious Disease 56(10): 1445-1450.
-
Al-Faham Z, Habboub G, Takriti F (2011) The sale of antibiotics without prescription in pharmacies in Damascus, Syria. The Journal of Infection in Developing Countries 5(05): 396-399.
-
Food and Drug Administration (2019) Summary Report on Antimicrobials Sold or Distributed for Use in Food- Producing Animals.
-
Van TTH, Yidana Z, Smooker, PM, Coloe, PJ (2020) Antibiotic use in food animals worldwide, with a focus on Africa: pluses and minuses. J Glob Antimicrobial. Resist 20: 170-177.
-
Tiseo K, Huber L, Gilbert M, Robinson TP, and Van Boeckel TPV (2020) Global trends in antimicrobial use in food animals from 2017 to 2030. Antibiotics (Basel) 9(12): 918.
-
Zhou J, Yun X, Wang J, Li Q, Wang Y (2022) A review on the Eco toxicological effect of sulphonamides on aquatic organisms. Toxicol Rep 29(9): 534-540.
-
Gwenzi W, Shamsizadeh Z, Gholipour S, Nikaeen M (2022) The air-borne antibiotic resistome: occurrence, health risks, and future directions. Sci Total Environ 15(8040: 150-154.
-
Hu Y, Yang X, Li J, Lv N, Liu F, et al. (2016) The bacterial mobile resistome transfer network connecting the animal and human microbiomes. Appl Environ Microbiol 82(22): 6672-6681.
-
Founou LL, Founou, RC, and Essack SY (2021) Antimicrobial resistance in the farm-to-plate continuum: more than a food safety issue. Future Science 7(5).
-
Reuland EA, Al Naiemi N, Raadsen SA, Savelkoul PHM, Kluytmans J, et al. (2014). Prevalence of ESBL-Producing Enterobacteriaceae in Raw Vegetables. Eur J Clin Microbiol Infect Dis 33(10): 1843-1846.
-
Turnidge JD, Gottlieb T, Mitchell DH, Coombs GW, Daly AD et al. (2014) Enterobacteriaceae Sepsis Outcome Programme annual report, 2013 Commun Dis Intell Q Rep 38(4): E327-333.
-
Leopold SJ, Van Leth F, Tarekegn H, Schultsz C (2014) Antimicrobial drug resistance among clinically relevant bacterial isolates in Sub-Saharan Africa: A Systematic review. J antimicrob chemother 69(9):2337–2353.
-
Martin I, Sawatzky P, Liu G, Mulvey MR (2015). Antimicrobial resistance to Neisseria gonorrhoeae in Canada: 2009-2013. CCDR 41(2): 35-41.
-
Temkin E, Adler A, Lerner A, Carmeli Y (2014) Carbapenem resistant Enterobacteriaceae: biology, epidemiology, and management. Ann N Y Acad Sci 1323(1): 22-42.
-
Gelbrand H, Miller-Petrie M, Pant S, Gandra S, Levinson J, et al. (2015) The State of the World’s Antibiotics. Wound Healing Southern Africa 8(2): 30-34.
-
Feasey NA, Gaskell K, Wong V, Msefula C, Selemani G, et al. (2015) Rapid emergence of multidrug resistant, H58- lineage Salmonella typhi in Blantyre, Malawi. PLoS Negl Trop Dis 9(4): e0003748.
-
(2016) The Jim O’Neil Report acknowledged that their figure may be a low estimate given the scarcity of data then available, therefore these two statistics cannot be directly compared. O’Neil, Jim. Tackling Drug-Resistant Infections Globally. Review on Antimicrobial Resistance.
-
Kayange N, Kamugisha E, Mwizamholya DL, Jeremiah S, Mshana SE (2010). Predictors of positive blood culture and deaths among neonates with suspected neonatal sepsis in a tertiary hospital, Mwanza-Tanzania. BMC Pediatr 10(1): 39.
-
Kariuki S, Gordon MA, Feasey N Parry CM (2015) Antimicrobial resistance and management of invasive Salmonella disease. Vaccine 3(3): 21-29.
-
Prestinaci F, Pezzotti P, Pantosti A (2015) Antimicrobial resistance: a global multifaceted phenomenon. Pathog Global Health 109(7): 309-318.
-
World Health Organization (2017) The World is running out of Antibiotics, WHO Report Confirms.
-
Reardon S (2014) Phage therapy gets revitalized. Nature 510 (7503): 15-16.
-
Xu C, Kong L, GAO H, Cheng X Wang X (2022) A Review of Current Bacterial Resistance to Antibiotics in Food Animals. Front Microbial 13: 822-689.
-
Sengupta S, Chattopadhyay MK, Grossart HP (2013) The multifaceted roles of antibiotics and antibiotic resistance in Nature. Front Microbiol 4: 47.
-
Bai H, He LY, Wu DL, Gao FZ, Zhang M (2022) Spread of airborne antibiotic resistance from animal farms to the environment: dispersal pattern and exposure risk. Environ Int 158: 106927.
-
Ahmed SM, Evans T, Standing H, Mahmud S (2013) Harnessing Pluralism for Better Health in Bangladesh. Lancet 382(9906): 1746–1755.
-
Antimicrobial Resistance Collaborators (2022) The Lancet 399(10325): 629-655.
-
Kirkcaldy RD, Kidd S, Weinstock HS, Papp JR, Bolan GA (2013). Trends in antimicrobial resistance in Neisseria gonorrhoeae in the USA: the Gonococcal isolate surveillance project. Sexually transmitted infections 89: 5-10.
-
Leekha S, Terrell LC, Edson RS (2011) General Principles of Antimicrobial Therapy. Mayo Clin Proc 86(2),156-167.
-
Mahmood T, Roy S, Siddiqui HH, Shamim A (2014) Antibiotic resistance a silent global threat. World journal of pharmacy and pharmaceutical science 4(02): 1177- 1197.
-
O’Neill J (2014) Antimicrobial resistance: tackling a crisis for the health and wealth of nations. Rev Antimicrobial Resist 20: 1-16
-
Rosen T (2011) Antibiotic resistance. An editorial review with recommendations. J Drugs Dermatol 10 (7): 724- 733.
-
Van Boeckel TP, Brower C, Gilbert M, Grenfell BT, Levin SA, et al. (2015) Global trends in antimicrobial use in food animals. Proc Natl Acad Sci 112(18): 5649-5654.
-
WHO (2009) UNICEF, World Bank, State of the world’s vaccines and immunization, 3rd Ed. Geneva, World Health Organization.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines