Non-Parental Child-Caregivers’ Utilization and Non-Utilization of Treated Mosquito Bed Nets in a Community on the Atlantic Ocean Coast of Lagos, Nigeria
Objective: To evaluate perception, ownership, use and defects in LLINs among non-parental caregivers in Iyaafin community on the Atlantic Ocean coastline of Lagos State, Nigeria. Methods: This cross-sectional, community-based study was conducted between February-April 2014. Residences of 129 non-parental caregivers to children under the age of five years were surveyed, using a convenience sampling method. Semistructured, interviewer-administered questionnaires were used to gather data. NCSS21 statistical software was used for data analysis. Results: Use of “Mosquito coils” a smoky repellent, is what most (72.1%) respondents said was how this coastal community prevent malaria. Only 22 (17.1%; 10, 15.2% male, 12, 19.1% female) said sleeping under mosquito nets prevent malaria. Majority (114, 88.4%) of the respondents said that living in a clean environment is the best way that malaria can be prevented. Approximately half (49.6%) of surveyed households did not have any mosquito nets while only 21 (16.3%) households had 1 mosquito net. Conclusions: Mosquito coil was the most common method of preventing malaria in the community of study. Few people possessed Long Lasting mosquito nets or any other nets and fewer slept under mosquito nets, night before survey.
Introduction
That malaria is a public health burden [1] and a major cause of morbidity and mortality [2], a major killer of children in endemic regions of Africa, is no more news.
According to the World Health Organization, 214 million cases of malaria and approximately 438,000 deaths due to the disease occurred globally in 2015 [3]. Malaria impacts predominantly children under the age of five years and pregnant women [4], especially in the first trimester, with minimal access to adequate and appropriate health care [5] and with inadequate protective immunity. In addition to this, malaria is recognized as one of the major diseases of poverty [6], others being Tuberculosis, HIV/AIDS, Measles, Pneumonia and Diarrheal Diseases [7]. International bodies such as the World Health Organization, UNICEF, World Bank, Global Funds for Aids, Tuberculosis and Malaria just to mention a few, have been in the forefront of reducing the burden of malaria in sub-Saharan Africa and in other malaria endemic parts of the world. In Central Africa Cameroon, where malaria prevalence is 50-70% [8], the disease is responsible for about 45% of clinical consultations, 57% of hospitalization days and 40% of mortality among children below 5 years [9]. WHO identified East Africa Ethiopia as one of the three countries accounting for 90% of the estimated number of Plasmodium falciparum infections in sub-Saharan Africa [10], the others being Nigeria and Democratic Republic of Congo. In West Africa Ghana, malaria is also a major cause of illness and death, especially among children below the age of five and pregnant women, where 13.7% of all admissions of pregnant women in 2006 was due to malaria out of who 9.0% died from the disease [11]. In West Africa Nigeria also, where transmission of malaria occurs throughout the year, the dominant vector of transmission is Anopheles gambiae ss while other species of Anopheles (A. funestus and A. arabiensis) are usually found in lesser density as co-existing with A. gambiae ss, or in isolation [12]. Insecticide-treated mosquito bed-net, when used properly, is currently the most cost-effective malaria prevention strategy in Africa, especially in Nigeria. This commodity has been distributed widely by many organizations at community level, at health facilities and in some cases at hospitality industries since the period after the Abuja Malaria Summit in 2000, to achieve universal access [13]. Insecticide treated net has been claimed to be the safest and most efficacious malaria control intervention [14] and its use consistently has been linked to about 90% reduction in the transmission of malaria [15]. In the first five years of the 21st Century, awareness of ITNs rose from 7% to 60% and is currently close to 100% [16]. Unfortunately, though, the gains of this awareness have been obliterated by low possession and even lower utilization of insecticide treated mosquito bed-nets in Nigeria [16]. There has been little information about ITN accessibility, ownership and use on the Atlantic Ocean coastline of Nigeria. There is an urgent need to apprehend the perceptions and practices of community structures, such as non-parental caregivers for the purpose of designing penetrating communication strategies within the community for better understanding of malaria control interventions. This study evaluated information of behavioral attitude, perception, ownership, and utilization of treated mosquito bed-nets by non-parental caregivers on the Atlantic Ocean coastline of Lagos, Nigeria. The goal was to bring awareness of governments and international agencies to this geographical location for the purpose of achieving universal access and correcting misconceptions of malaria.
Materials and Method
Study Area
Iyaafin community, located in Badagry Local Government Area (lying at 6°25′N 2°53′E) is a farming and trading community of about 3000 people.
Study Population
Data reported here came from caregivers (not biological parents) of children under the age of five years, who were brought for malariometric examinations and for provision of permethrin-based protective clothing against mosquito bites (pCAM) called Moskeeto Armor.
Study Design and Data Collection
The study was descriptive and cross-sectional in design. A semi-structured questionnaire, prepared in English language but communicated in common local language, was used to extract information on perception and behavioral attitude of the non-parental child caregivers who brought under-five year old children for malaria screening. All 129 caregivers were interviewed successfully and without objection. The Community gatekeepers, including the Traditional Ruler gave consent to conduct the study which took place between February and April 2014. Of particular interest in this part of the study were issues relating to ownership, utilization, and non-utilization of, as well as damage to treated mosquito nets among the caregivers.
Inclusion and Exclusion Criteria
To be admitted into the study, a caregiver must have brought a febrile under-five year child for malaria screening, must have been resident in the community and be directly related to the under-five brought for screening. Parents of under-fives, children with severe malaria, severe anemia, congenital diseases, other chronic illnesses, on admission in a health facility, or refusal of parents/caregivers to participate in the study were excluded. A caregiver who is visiting, has not lived with the under-five for at least 12 months and who appeared very ill was also excluded.
Ethical Clearance
The study was approved by the National Health Research Ethics Committee, (No. NHREC 04/04/2008 Ref. No. RFC/10/06/367) and the approval was received on February 2014. The objectives of the study were explained to the Traditional Ruler, Community Gatekeepers, and each participating parent/caregiver. Informed consent was requested for by the researchers and given by parent or care givers of the children.
Training of Fieldworkers
A 2-day preparation to intimate field workers and data collectors with field operations, conflict resolution, and inter-personal relationship on the field was conducted during which the semi-structured questionnaire to be served was reviewed.
The Intervention
The material that was used for the intervention was a permethrin-based fabric, called “Moskeeto Armor®”, a protective clothing for the prevention of malaria (pCAM) manufactured by ING Activewear®, USA. The material was sewn as a wearing apparel to cover almost all parts of the body, for each child in the study to wear daily, especially in the evenings.
Data entry and statistical analysis
Data was initially coded and entered into WPS Spreadsheet 2019 and cleaned before being exported into NCSS 21 (Kaysville, Utah, USA) statistical software for analysis. Descriptive and inferential statistics were adopted in analyzing the data. While the descriptive statistics comprised frequencies, percentages, mean, and standard deviation, the inferential statistic used was logistic regression. Results of the regression analysis were calculated based on 95% confidence level (alpha= 0.05) and tests using measures of association such as odds ratio. A p-value less than 0.05 was considered statistically significant. Utilization was defined as when study subjects responded to the affirmative having slept under the ITN in the night preceding the study. Data were presented as Tables, Map and Figures.
Results
The socio-demographic profiles of the study participants have been reported earlier [17]. Briefly, the mean (±sd) age of the respondents (male = 66, 51.2%; female = 66, 48.8%), was 24.5 (5.5) years with no significant difference between males and females. Most of the respondents were in the age range of 25-29 years (n=46, 35.7%), students (n=62, 48.1%) and singles (n=85, 65.9%). Overall, only 3 (2.3%) females had no formal education, while 19 (76.0%) of the 25 subjects with primary education, 33 (46.5%) of the 71 with secondary education, 3 (33.3%) of the 9 with Diploma and 5 (23.8%) of the 21 with tertiary education were females. Of the 26 traders in the study group, 22 (84.6%) were females and of the 11 civil servants 7 (63.6%) were females. Further, of the
44 married respondents, 32 (72.7%) were females and of the 85 singles, only 31 (36.5%) were females. When this study was carried out 77 (59.7%) respondents were receiving monthly income of <N5000 (approximately US$33.3 then but US$6.7 now) with more males (n=44, 66.7%) than females (n=33, 52.4%) receiving this amount. Table 1 illustrates that the most common method of malaria prevention commonly agreed to by both male (69.7%) and female (74.6%) respondents was the use of mosquito coils. Only 17% of the respondents believed that members of the community sleep under mosquito bed nets to prevent malaria. Only 1.6% of respondents agreed that burning of dried orange peel is still used to prevent malaria. Majority (88.4%) of the respondents believed that living in a clean environment can prevent malaria but very few supposed that the disease can be prevented by wearing protective clothing (7.0%) or taking herbal tea (2.3%). The Table also shows that only 55 (42.6%) respondents currently owned a mosquito net, that females were 1.7 times more likely to own a mosquito net (χ²=2.16, P-value=0.14, OR=1.70, 95% CI: 0.84, 3.43). Of the 55 that own a mosquito net, only 33 (60.0%) were aware that this commodity was treated with an insecticide. Women were 2.1 times more likely to be aware that the mosquito nets they own was treated with insecticide or not (χ²=1.74, P-value=0.19, OR=2.10, 95% CI: 0.70, 6.30). Of the 55 who currently owned a mosquito net, whether treated or not, only 21 (38.1%) slept under it the night before the survey. If the entire study subject is taken into consideration, the proportion of those who slept under mosquito net the night before the survey would drop to 16.3% (21/129). As expected, females were 2.41 times more likely to sleep under mosquito nets than males (χ²=3.17, P-value=0.08, OR=2.41, 95% CI: 0.90, 6.44). Of the 65 households surveyed, 21 (32.3%) had 1 mosquito net, while 18 (27.7%), 15 (23.1%), 3 (4.6%) and 8 (12.3%) had 2, 3, 4 and ≥5 mosquito nets, respectively. Though 21 households each had 1 mosquito net, nobody slept under a mosquito net in 9 (42.9%) of these households the previous night before the survey. Only 2 people slept under a mosquito net in each of the 6 (28.6%) households with one mosquito net. In the 18 (27.7%) households each with 2 mosquito nets, only 4 people slept under this commodity in 5 (27.8%) of these household the previous night. In the 3 (4.6%) households each with 4 mosquito nets 4 people slept under this commodity in 2 (66.7%) of the said household night before the survey. A total of 8 (38.1%), 5 (27.8%) and 3 (20.0%) households with 1, 2 or 3 mosquito nets had a minimum of 1 bed with hanging mosquito net while 10 (47.6%), 7 (38.9%) and 3 (20.0%) households with 1, 2 or 3 mosquito nets had a minimum of one bed in the household. In all, 8 people in households with 2 mosquito nets and 3 people in households with 3 mosquito nets slept on mat with hanging mosquito net night before the survey (Table 2). A total of 43.6% and 32.7% of the respondents had owned a mosquito net for a year and more and for 2 years and more.
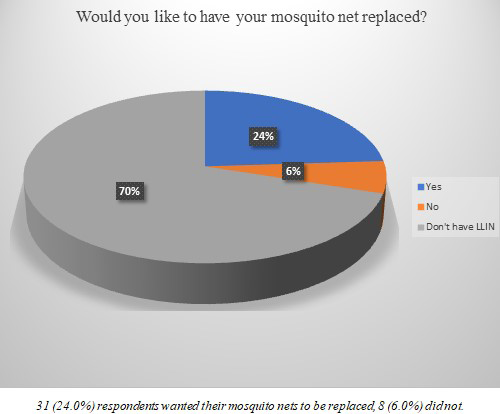
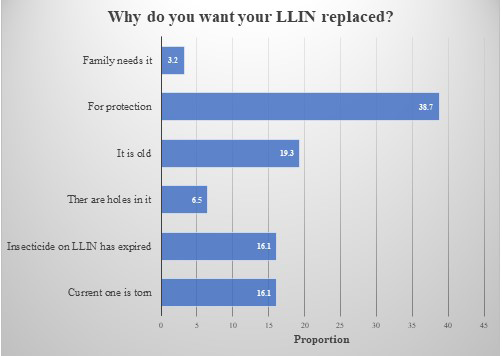
Majority (83.7%) of these mosquito nets were supplied to the study community by the Lagos State Government as part of what Global Fund for Aids, Tuberculosis and Malaria (GFATM) supplied the Federal Government of Nigeria as Long-Lasting Insecticide-treated Nets (LLINs). Only 2 (3.6%) participants purchased the mosquito nets out-of-pocket at open market. During the study, 12 (21.8%) of the mosquito nets were observed to have holes of various numbers, sizes, and dimension on top (3, 25.0%) or on the side (9, 75.0%) of the nets. Of the 12 damaged mosquito nets, 6 (50.0%) had 2 holes, and each of the remaining mosquito nets had 1, or more than 2 holes the maximum of which was 16 holes. The mean (±sd) diameter of the observed holes was 2.75 cm, with a minimum of 1 cm, a maximum of 8 and a mode of 2 cm (Table 3). Of those that own mosquito nets, only 24% would like to have the commodity replaced (Figure 1) primarily for continued protection (38.7%) against malaria (Figure 2).
| Responses | All | Male | Female | |
|---|---|---|---|---|
| How do people in this community prevent malaria | Use of mosquito coils | 93 (72.1) | 46 (69.7) | 47 (74.6) |
| How do people in this community prevent malaria | Use of insect repellent | 8 (6.2) | 6 (9.1) | 2 (3.2) |
| How do people in this community prevent malaria | Sleeping under mosquito bed nets | 22 (17.1) | 10 (15.2) | 12 (19.1) |
| How do people in this community prevent malaria | By burning dried orange peel | 2 (1.6) | 2 (3.0) | 0 (0.0) |
| How do people in this community prevent malaria | Don’t know | 4 (3.1) | 2 (3.0) | 2 (3.2) |
| How can malaria best be prevented | By making sure the environment is clean | 114 (88.4) | 59 (89.4) | 55 (87.3) |
| How can malaria best be prevented | By taking medicine every week | 1 (0.8) | 0 (0.0) | 1 (1.6) |
| How can malaria best be prevented | By wearing protective clothing | 9 (7.0) | 4 (6.1) | 5 (7.9) |
| How can malaria best be prevented | By taking native medicine everyday | 3 (2.3) | 2 (3.0) | 1 (1.6) |
| How can malaria best be prevented | Don’t know | 2 (1.6) | 1 (1.5) | 1 (1.6) |
| Do you currently own a mosquito net? | Yes | 55 (42.6) | 24 (36.4) | 31 (49.2) |
| Do you currently own a mosquito net? | No | 74 (57.4) | 42 (63.6) | 32 (50.8) |
| Do you currently own a mosquito net? | χ2(P-value) | - | 2.16 (0.14) | |
| Do you currently own a mosquito net? | OR (95% CI) | - | 0.59 (0.29, 1.19) | 1.70 (0.84, 3.43) |
| If yes, is it treated with insecticide? | Yes | 33 (60.0) | 12 (50.0) | 21 (67.7) |
| If yes, is it treated with insecticide? | No | 7 (12.7) | 5 (20.8) | 2 (6.4) |
| If yes, is it treated with insecticide? | Don’t know | 15 (27.3) | 7* (29.2) | 8** (25.8) |
| If yes, is it treated with insecticide? | χ2(P-value) | - | 1.74 (0.19) | |
| If yes, is it treated with insecticide? | OR (95% CI) | - | 0.48 (0.16, 1.43) | 2.10 (0.70, 6.30) |
| Did you sleep under a mosquito net last night? | Yes | 21 (38.2) | 7 (10.6) | 14 (22.2) |
| Did you sleep under a mosquito net last night? | No | 108 (83.7) | 59 (89.4) | 49 (77.8) |
| Did you sleep under a mosquito net last night? | χ2(P-value) | - | 3.17 (0.08) | |
| Did you sleep under a mosquito net last night? | OR (95% CI) | - | 0.42 (0.16, 1.11) | 2.41 (0.90, 6.44) |
Table 1: Perception, ownership and utilization of malaria and malaria prevention commodity among residents on the Atlantic Ocean
| Indicator | Freq. | Number of mosquito nets in surveyed household | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ≥5 | ||
| Number (%) of households | ||||||
| 21 (32.3) | 18 (27.7) | 15 (23.1) | 3 (4.6) | 8 (12.3) | ||
| Number of people that slept under a mosquito net previous night before survey | 0 | 9 (42.9) | 1 (5.6) | 0 (0.0) | - | - |
| 1 | 3 (14.3) | 0 (0.0) | 0 (0.0) | - | - | |
| 2 | 6 (28.6) | 4 (22.2) | 4 (26.7) | - | 3 (37.5) | |
| 3 | 2 (9.5) | 4 (22.2) | 3 (20.0) | - | - | |
| 4 | 1 (4.8) | 5 (27.8) | 2 (13.3) | 2 (66.7) | - | |
| ≥5 | 0 (0.0) | 4 (22.2) | 6 (40.0) | 1 (33.3) | 5 (62.5) | |
| Number of beds in surveyed households | 0 | 1 (4.8) | 1 (5.6) | 0 (0.0) | - | - |
| 1 | 10 (47.6) | 7 (38.9) | 3 (20.0) | - | 1 (12.5) | |
| 2 | 5 (23.8) | 7 (38.9) | 1 (6.7) | - | 1 (12.5) | |
| 3 | 3 (14.3) | 2 (11.1) | 7 (46.7) | - | - | |
| 4 | 1 (4.8) | 1 (5.6) | 3 (20.0) | 3 (100.0) | - | |
| ≥5 | 1 (4.8) | 0 (0.0) | 1 (6.7) | - | 6 (75.0) | |
| Number of beds that have mosquito nets hanging on them | 0 | 12 (57.1) | 2 (11.1) | 2 (13.3) | - | 1 (12.5) |
| 1 | 8 (38.1) | 5 (27.8) | 3 (20.0) | - | 0 (0.0) | |
| 2 | 0 (0.0) | 10 (55.6) | 2 (13.3) | 2 (66.7) | 2 (25.0) | |
| 3 | 1 (4.8) | 0 (0.0) | 8 (53.3) | - | - | |
| 4 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (33.3) | - | |
| ≥5 | 0 (0.0) | 1 (5.6) | 0 (0.0) | - | 5 (62.5) | |
| Number of people that slept on a mat night before survey with mosquito net hanging | 0 | 21 (100.0) | 10 (55.6) | 12 (80.0) | 3 (100.0) | 7 (87.5) |
| 1 | - | 1 (5.6) | 1 (6.7) | - | 1 (12.5) | |
| 2 | - | 6 (33.3) | 1 (6.7) | - | - | |
| 3 | - | 0 (0.0) | 1 (6.7) | - | - | |
| 4 | - | 1 (5.6) | - | - | - | |
| ≥5 | - | 0 (0.0) | - | - | - |
Table 2: Profile of households with beds, mosquito nets and people who slept under mosquito nets.
| Variable | Item | All | |
|---|---|---|---|
| n | % | ||
| Duration of time since owning a mosquito net | <1 year | 5 | 9.1 |
| ≥1year | 24 | 43.6 | |
| ≥2 years | 18 | 32.7 | |
| ≥3 years | 5 | 9.1 | |
| ≥4 years | 3 | 5.5 | |
| How did you get the LLIN | Government campaign | 46 | 83.7 |
| Bought it out-of-pocket | 2 | 3.6 | |
| Given by someone | 7 | 12.7 | |
| If bought, from where? | Open market | 2 | 3.6 |
| Is LLIN torn or have holes in it? | Yes | 12 | 21.8 |
| No | 43 | 78.2 | |
| Number of holes in the LLIN? | 1 | 1 | 8.3 |
| 2 | 6 | 50.0 | |
| 3 | 1 | 8.3 | |
| 6 | 1 | 8.3 | |
| 9 | 1 | 8.3 | |
| 13 | 1 | 8.3 | |
| 16 | 1 | 8.3 | |
| Part of LLIN where there are holes | Top | 3 | 25.0 |
| Side | 9 | 75.0 | |
| Mean (±sd) diameter (cm) of holes | 2.75 (1.55) | ||
| Minimum/Maximum diameter (cm) | 1.00/8.00 | ||
| Median/Mode (cm) | 2.0/2.0 |
Table 3: Description and profile of mosquito nets in the community.
Discussion
In parts of the world where malaria is endemic, attempts to reduce the effect of the disease on humans and on countries’ economy have been carried out at governmental, community and individual levels with some measure of success. An old paper observed that, at the community and individual levels, malaria, in most cases, is often treated at home [18], except when it becomes severe or when there are available, appropriate, adequate, and prompt services would people seek treatment at nearby health facilities. A plethora of components are associated with the control of malaria, majority of which have been neglected or disregarded and thus not evaluated at the community level, in different socio- cultural milieu, geo-political conditions and environmental settings. This study documents the malaria control measures, access to, possession and utilization of one such malaria control commodity - insecticide treated mosquito nets - in one rural community on the Atlantic Ocean coast of Lagos, Nigeria. The first major finding in this study is that mosquito coil was identified, mainly by female caregivers, as the main method of malaria prevention by majority of the respondents. One Ethiopian study ascertained that, empowering women with educative information could lead to a better malaria control and thus influence the family and the community [19], a statement that was verified by a Nigerian study [20]. The 72.1% respondents that asserted the use of mosquito coil for malaria prevention is this Nigerian study is far higher than the 44.2% reported from a Ghanaian study [21]. Mosquito coils are usually derived from pyrethroid insect repellent and/or plant-based repellents (e.g., citronella). Liu et al however reported that mosquito coils emit fine particles (particulate matter < 2.5 μm in diameter or PM2.5) such as polycyclic aromatic hydrocarbons (PAHs), aldehydes, and ketones; that a burning mosquito coil emits the same amount of PM2.5 mass as burning 75–137 cigarettes and that the release of formaldehyde from one lit coil can be as high as that released from burning 51 cigarettes [22]. Being exposed to smoke from mosquito coils thus poses acute and chronic health risks as the smoke may contain carcinogenic substances. In the same vein, 88.4% of the caregivers agreed that malaria prevention is consequent on living in a clean environment. This is much higher than the 10.3% who mentioned environmental sanitation in a study conducted in Cameroon [23]. The environment has long been linked with malaria, which derived its name from Italian words mal’aria or “bad air” which was associated with marshes and swamps [24]. As stated by Bradley, “environmental changes and interventions produce a dynamic and changing pattern of malaria” [25]. The long history of mankind has shown repeatedly that diseases of humans such as malaria, tuberculosis, measles, typhoid, and other zoonotic diseases are closely associated with environmental condition. Access to, ownership and utilization of treated mosquito nets in malaria endemic regions have been a topic of debate and various epidemiological studies for over two decades now. The 16.3% non-parental care givers who slept under treated mosquito nets night before survey was lower than the 28.9% reported elsewhere in Nigeria [26, 27], Zimbabwe [28] or the 85.8% in Ghana [29]. This might be due to lack of information on the usefulness of treated mosquito nets in malaria control or non-accessibility to the commodity when it was distributed by the government or by other organizations. Females were approximately two and a half times more likely to utilize treated mosquito nets than males, reinforcing the idea that women mainly should be targets of educational campaign on malaria control. Few households were observed to have no beds, but household members sleep on mats. This highlights an important issue which has not been fully studied - that people who do not have beds to sleep on may think it not worthwhile to possess a treated mosquito net. One critical area in malaria control that has not been investigated is the condition of the treated mosquito nets during and after its lifespan. Majority of those who possessed treated mosquito nets in this study have had it for over one year but less than two years while only a few had possessed it for less than a year or more than four years. Most treated mosquito nets that were torn had just one hole, mainly at the side of the treated mosquito net. Holes in the commodity might be due to weakness of the mesh due to long usage, domestic accident or brought about by a child playing with it. This study did not find out how the holes occurred in the nets. The 2.2 cm2 median total hole area in this study was smaller than the 9.4 cm2 reported and the mean diameter of 2.75 cm2 was less than WHO’s proportionate hole index (pHI) cut-off of <79 cm2 cm which suggests that the treated mosquito nets in the study may still be effective [30].
Conclusion
Mosquito coils were the commodity used by communities on the Atlantic Ocean coastline in Lagos, Southwest Nigeria and ownership of treated mosquito nets was not commensurate with usage. “Mosquito coils” a smoky repellent, is what most respondents said was how this coastal community prevent malaria. Though treated mosquito nets were distributed by the State government to communities in the state, ownership among respondents was low and usage was even lower. Few of the respondents agreed that sleeping under mosquito nets prevent malaria. Majority of the respondents believed that living in a clean environment is the best way that malaria can be prevented. Approximately half (49.6%) of surveyed households did not have any mosquito nets while only 21 (16.3%) households had 1 mosquito net.
Recommendation
There is a need to focus on targeted interventions, promote awareness and prevention, and address misconceptions about use of treated mosquito nets to prevent malaria morbidity and mortality. There is need to address replacement of old insecticide treated nets or employ a new technology to extend the quality and durability of treated mosquito nets that are currently in use.
- Competing Interests: The author(s) declare that they have no competing interests.
- Acknowledgement: We are grateful to all members of Iyaafin community that participated in the study. We also appreciate the cooperation of the community gatekeepers. This study was supported by INGActivewear, USA.
- Access to Data Material: Underlying research materials related to this paper can be accessed by request from the Principal Investigator.
References
-
Oberländer L, Elverdan B (2000) Malaria in the United Republic of Tanzania: Cultural considerations and Health-Seeking Behaviour. Bull World Health Organ 78(11): 1352-1357.
-
Karunamoorthi K, Abdi K (2010) Knowledge, and Health-Seeking Behaviour for Malaria Among the Local Inhabitants in an Endemic area in Ethiopia: Implications for control. Health 2(6).
-
World Health Organization (2015) World Malaria Report 2015. Switzerland.
-
Snow RW, Guerra CA, Noor AM, Myint HY, Hay SI (2005) The Global Distribution of Clinical Episodes of Plasmodium Falciparum Malaria. Nature 434(7030): 214-217.
-
Teklehaimanot A, McCord GC, Sachs JD (2007) Scaling Up Malaria Control in Africa: An Economic and Epidemiological Assessment. Am J Trop Med Hyg 77(6S): 138-144.
-
Barofsky J, Chase C, Anekwe T, Farzadfar F (2011) The Economic Effects of Malaria Eradication: Evidence from an Iintervention in Uganda. PGDA Working Paper pp: 70.
-
Singh AR, Singh SA (2008) Diseases of Poverty and Lifestyle, Well-Being, and Human Development. Mens Sana Monogr 6(1): 187-225.
-
Bowa NC (2022) The Numbers that are Scary Paludisme. National Malaria Control Program, Cameroon, 2006.
-
Ministry of Public Health (2007) National Strategic Plan for Malaria Control in Cameroon, 2007-2010. Ministry of Public Health, Qatar, pp: 1-134.
-
World Health Organization (2014) World Malaria Report 2014. Switzerland.
-
Ministry of Health (2009) Anti-Malaria Drug policy for Ghana. 2nd Revised version, Republic of Ghana, Ghana.
-
Awolola TS, Oyewole IO, Koekemoer LL, Coetzee M (2005) Identification of Three Members of the Anopheles Funestus (Diptera: Culicidae) Group and their Role in Malaria Transmission in two Ecological Zones in Nigeria. Trans R Soc Trop Med Hyg 99(7): 525-531.
-
Federal Ministry of Health (2008) National Malaria Control Programme, Strategic Plan 2009-2013: A Road Map for Malaria Control in Nigeria. Federal Ministry of Health pp: 1-39.
-
Elom MO, Alo MN, Okey EN, Ugah UI, Ibiam AG (2013) A Survey of Utilization and Effectiveness of Insecticide- Treated Bed Nets (ITNs) as Intervention Strategy in Malaria Transmission among Pregnant Women in a Rural Community in Ebonyi State, Southeastern Nigeria. IOSR Journal of Dental and Medical Sciences 9(2): 60-64.
-
Giming JE, Vulule JM, Lo TQ, Kamau L, Kokzak MS, et al. (2003) Impact of Permethrin-Treated Bed Nets on Entomological Indices in an Area of Intense Year-Round Malaria Transmission. American Journal of Tropical Medicine and Hygiene 68 (suppl 4): 16-22.
-
Baume CA, Mavin C (2008) Gains in Awareness, Ownership and Use of Insecticide Treated Bed Nets in Nigeria, Senegal Uganda, and Zambia. Malaria Journal 7: 153.
-
Afolabi BM, Afolabi TM, Aiyesetenikan A, Ganiyu DF (2022) The Perception and Behavioral Attitude to Malaria of Non-parental Caregivers Living on an Atlantic Ocean Coastal Community in Nigeria: Paper 1. Japan Journal of Clinical & Medical Research 2(2): 1-8.
-
Foster S (1995) Treatment of Malaria Outside the Formal Health Services. J Trop Med Hyg 98(1): 29-34.
-
Hwang J, Graves PM, Jima D, Reithinger R, Kachur SP (2007) Knowledge of Malaria and its Association with Malaria-Related Behaviors: Results from the Malaria Indicator survey, Ethiopia. PLoS One 5(7): e11692.
-
Iriemenam NC, Dosunmu AO, Oyibo WA, Fagbenro- Beyioku AF (2011) Knowledge, Attitude, Perception of Malaria and Evaluation of Malaria Parasitaemia Among Pregnant Women Attending Antenatal Care Clinic in Metropolitan Lagos, Nigeria. J Vector Borne Dis 48(1): 12-17.
-
Hogarh JN, Antwi-Agyei P, Obiri-Danso K (2016) Application of Mosquito Repellent Coils and Associated Self-Reported Health Issues in Ghana. Malar J 15: 61.
-
Liu W, Zhang J, Hashim JH, Jalaludin J, Hashim Z, et al. (2003) Mosquito Coil Emissions and Health Implications. Environ Health Perspect 111(12): 1454-1460.
-
Nsagha DS, Njunda AL, Kamga HLF, Assob JCN, Wiysonge CS, et al. (2011) Knowledge and Practices Relating to Malaria in Ndu Community of Cameroon: Signs and Symptoms, Causes and Prevention. Journal of Public Health and Epidemiology 3(6): 294-300.
-
Fagan T (2000) When was malaria first discovered and by whom? How is the disease transmitted? What are its effects?. Scientific American, USA.
-
Bradley DJ (1999) The Last and the Next Hundred years of Malariology. Parassitologia 41(1-3): 11-18.
-
Ordinioha B (2012) The Use and Misuse of Mass Distributed Free Insecticide Treated Bednets in a Semi- Urban Community in Rivers State, Nigeria. Ann Afr Med 11(3): 163-168.
-
Amoran OE, Senbanjo IO, Asagwara CE (2001) Determinants of Insecticide-Treated Nets Use Among Youth Corps Members in Edo State, Niger Biomed Centr Pub Hlth 11: 728.
-
Shedrack SP, Bartholomew M, Addmore C (2012) An Investigation of the Use of Rectangular Insecticide Treated Nets for Malaria Control in Chipinge District, Zimbabwe: A Descriptive Study. The Pan Afr Med J 13: 5.
-
Laar AS, Laar AK, Dalinjong PA (2013) Community Perception of Malaria and its Influence on Health- Seeking Behaviour in Rural Ghana: A Descriptive Study. Malaria World Journal 1: 6.
-
Minta AA, Landman KZ, Mwandama DA, Shah MP, Eng JV, et al. (2017) The Effect of Holes in Long-Lasting Insecticidal Nets on Malaria in Malawi: Results from a Case-Control Study Malar J 16(1): 394.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines