The COVID-19 Impact on Inpatient Hospital Admissions in Indiaa Cross-Sectional Study
Health is a subject of state as per the constitution of India. Hence different states of India have autonomy in deciding and reserving different percentages of beds for the COVID-19 cases as per their needs as well as availability of beds. As an example, Delhi had reserved 50% of ICU (intensive care unit) beds for COVID-19 patients. Due to the novel corona virus disease 2019 (COVID-19), we found that there have been widespread changes in healthcare access by different types of patients suffering from different diseases. Besides fear of COVID-19 Nosocomial infection, this new arrangement and prioritization of the sudden needs of huge number of COVID-19 patients it is anticipated that this situation may have reduced the IPD patients suffering from other diseases. The key researcher has observed significant change in period prevalence of IPD patients during his duties at health centres in the COVID-19 era which tempted him to find out answer to title research question. This study was done to assess that, does the COVID-19 era has affected IPD services utilization by patient (positively or negatively) of other disease on a large countrywide basis? This study will definitely help policy and decision makers to visualize the health services delivery to IPD patients of diseases other than COVID-19. This research study is an attempt to highlight the COVID-19 impacts on IPD patients of other diseases. We have started this novel study with key aim to assess positive or any negative impact of COVID-19 situation on IPD (other than COVID-19) hospital admissions count in India to assess IPD services utilization by them. We included all (public/ private/rural/urban) health facilities across 36 states and union territories of India. The data were obtained from online HMIS (Health Management Information System) of Ministry of Health and Family Welfare, GoI (Government of India). This study was not a sample survey and we included all IPDs (indoor patients) of 36 states and union territories of India. The GoI enforced an obligatory nationwide lockdown from 25th March 2020, ending on 31st May 2020. This study revealed that the mean IPD admission reduced during COVID-19 pandemic period of this study by 2048459 numbers or in percentage it was reduced by 27.55%. This study found that there is a significant reduction in various IPD admissions for medical conditions other than COVID-19, during the COVID-19 period which must be a matter of concern to important stakeholders of the health system, in the light of our knowledge that it is not possible to reduce the burden of disease in India in a small period or overnight. Governments of India should make strategies on priority to trim down burden of morbidity and mortality due to CDs as well as NCDs, in order to reap the benefits of Demographic Dividend. The COVID-19 or any such pandemic and distress management should not be prioritized at the cost of other NCDs and CDs management
Introduction
Background/Rationale
The COVID-19 pandemic have a global negative impact on the utilization of health services through changes in demand for services as well as disruptions in the delivery of ordinary medical care [1]. From the start of the corona virus disease 2019 (COVID-19) epidemic and ensuing pandemic, there have been significant changes to healthcare systems all around the world [2]. Patients were advised to separate themselves due to the contagious nature of COVID-19, and medical professionals relocated a significant portion of their practise to virtual visits and telemedicine for those who needed more immediate follow-up [3]. In addition to influencing the transition to virtual healthcare, COVID-19 also had an impact on non-COVID-19-related hospital admissions and visits [4]. There is mounting evidence from other nations that COVID-19 has an impact on variances in healthcare utilisation trends [5, 6].
Popularly known as indoor in India, the indoor patient department (IPD) is a part of the hospitals for admitting usually the patients from the outdoor department (OPD), emergency department (ED), or a referred patient from any lower health centres for special medical trouble that oblige hospital admission for treatment [7]. IPD of any hospital is equipped with medical beds, medical equipment, and a medical team [8]. Index case of SARS-CoV-2 (severe acute respiratory syndrome-coronavirus-2) causing COVID-19 was foremost established from the Wuhan, Hubei, China in December 2019, with first confirmed COVID-19 case outside china in Thailand on 13th January, 2020 [9]. Subsequently, COVID-19 spread to more than 200 countries [10]. As per IHR (International Health Regulations-2005) guidelines, World Health Organization (WHO) affirmed COVID-19 (CORONAVIRUS DISEASE-2019) as an International Public Health Crisis on January, 30th 2020 [11]. WHO advised nations with various protocols, strategies, advisories, and guidelines to stop the outbreak [11]. In India index case of COVID-19 infection was first suspected on January, 27th 2020, in Kerala which was subsequently affirmed as COVID-19 infection by the NIV (National Institute of Virology), Pune, Maharashtra, on January 30th 2020 [12]. The Government of India (GoI), enforced an obligatory nationwide lockdown, in order to stop the COVID-19 (25th march 2020 to 31st may 2020) [13]. This novel lockdown intervention had disrupted the normal functioning of the health services in India [14]. The health services are significant in India due to needs of large population with restricted resources, poor old infrastructure amidst massive demand [15]. New-born, old citizens, pregnant women’s are especially vulnerable to this novel crisis due to COVID-19 situations because of special requirements [16]. The pandemic challenged the healthcare systems of even well to do nations as well as India [17]. Most of available resources of healthcare like infrastructure, ambulance services, medical personnel’s, were deployed to stop the pandemic which had affected essential health services [18]. There are wide gaps in healthcare services delivery among various 36 states and union territories (UTs) in India, evident from the annual reports of NITI (National Institution for Transforming India) AAYOG SHI (State Health Index) [19]. There is lack of PUBLIC HEALTH MANAGEMENT CADRE (PHMC) in some states of India [20]. The WHO report had queried the COVID-19 mortality figures provided by the GoI [21]. The GoI also followed strategies of other nations like closing borders, restrictive social interaction, making segregation wards for COVID-19 mostly in existing hospitals [22]. The Prevalence of COVID-19 cases in INDIA on September, 09th, 2022, were 44,482,411, mortality count 528,090 [23]. Health is a subject of state as per the constitution of India [24]. Hence different states of India have autonomy to decide and reserve different percentages of COVID-19 beds for the COVID-19 cases as per their needs as well as availability of beds. As an example, Delhi had reserved 50% of ICU (intensive care unit) for COVID-19 patients [25].
Besides fear of COVID-19 Nosocomial infection, this new arrangement and prioritization of needs of the COVID-19 patients may have reduced other diseases IPD patients. The key researcher has observed significant change in period prevalence of IPD during his duties at health centres in the COVID-19 era. This study was done to assess that, does the COVID-19 era has affected IPD service utilization by patient (positively or negatively) of other disease? Delay or abstinence from hospital admission can impose an undue public health challenges by health deterioration or even death of many patient. This research study is an attempt to highlight the COVID-19 impacts on IPD admissions of other prevalent significant diseases in India. This study will definitely help policy and decision makers to visualize health services delivery to IPD patients of diseases other than COVID-19.
Aim & Objectives
We have started this novel study with key aim to assess positive or any negative impact of COVID-19 situation on IPD (other than COVID-19) hospital admissions count in India. We included all (public/private/rural/urban) health facilities across 36 states and union territories in India. The data were obtained from online HMIS (Health Management Information System) of GoI, Ministry of Health and Family Welfare (MoHFW). This study has done an analysis on IPD health service utilization during COVID-19 situation, of significant and more prevalent diseases in India. The key objective of this study is to assess the increase / decrease in the IPD patients during the covid-19 years in comparison to the pre-pandemic period. The Mean IPD patient is considered for comparison.
Methods & Materials
This research study is done for assessing the COVID-19 impact on IPD service utilization. Change in the numbers of IPD patients during COVID-19 epoch is assumed to be effects of pandemic. COVID-19 era IPD patient’s data is compared to pre-pandemic years for above purpose. As the index case was reported in January 2020, epoch before 1st January 2020 is called the pre-pandemic era. From 1st January 2020 onward the period is taken as the pandemic epoch as discussed above.
This study was not sample survey and included all IPDs (indoor patients) of 36 states and union territories of India. Hence there is no requirement of any statistical t-test or ANOVA. There is no question of generalisability of data as the data included the entire population of IPD admissions. Hence we do not feel any requirements for applying inferential statistical methods. This is a novel, comparative, cross- sectional, research study to assess the extent of the invisible impacts of the COVID-19 as stated above. Health facility- based retrospective study was conducted for IPD admissions in India, across 36 states and UTs from 1st January 2018 to 31st May 2021. The data collected from HMIS, for IPD admissions during this study period is available in Table- 1and presented as Figure-1 for easy visualization. The HMIS reporting arrangement is used by all 36 states and UTs of India [26]. This study included all the (Public-private-rural- urban) health facilities of 36 states and UTs of India, on HMIS.
Study Variables and Operational Definition
The variables included for this study were IPD count of following inpatients:-
- Inpatient (Male)- Children<18yrs
- Inpatient (Male)- Adults
- Inpatient (Female)- Children<18yrs
- Inpatient (Female)- Adults
- Inpatient - Malaria
- Inpatient - Dengue
- Inpatient - Typhoid
- Inpatient - Asthma, Chronic Obstructive Pulmonary Disease (COPD), Respiratory infections
- Inpatient - Tuberculosis
- Inpatient - Pyrexia of unknown origin (PUO)
- Inpatient - Diarrhoea with dehydration
- Inpatient - Hepatitis Any unusual change, in the pattern or count of above mentioned variables during the COVID-19 pandemic compared to pre-pandemic period in IPD services utilization is considered as COVID-19 pandemic impact for this study purpose. Microsoft office and stata15.1 software were only utilized for this study data collection and analysis.
| variable | Inpatient (Male)- Children<18yrs | Inpatient (Male)- Adults | Inpatient (Female)- Children<18yrs | Inpatient (Female)- Adults | Inpatient - Malaria | Inpatient - Dengue | Inpatient - Typhoid | Inpatient - Asthma, Chronic Obstructive Pulmonary Disease (COPD), Respiratory infections | Inpatient - Tuberculosis | Inpatient - Pyrexia of unknown origin (PUO) | Inpatient - Diarrhoea with dehydration | Inpatient - Hepatitis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18-Jan | 684699 | 1574918 | 563919 | 2678916 | 20456 | 6728 | 36655 | 144382 | 17726 | 167898 | 149561 | 11965 |
| 18-Feb | 681371 | 1628263 | 597415 | 2759214 | 21223 | 2874 | 39239 | 148166 | 19116 | 172680 | 171802 | 17066 |
| 18-Mar | 726858 | 1791078 | 632809 | 2957897 | 28899 | 2278 | 44393 | 139901 | 19216 | 191845 | 211370 | 12607 |
| 18-Apr | 681470 | 1752082 | 632745 | 2853456 | 36400 | 3274 | 38096 | 158459 | 21490 | 178071 | 256333 | 11851 |
| 18- May | 742325 | 1963800 | 667019 | 3150982 | 24301 | 5311 | 39988 | 131532 | 21387 | 181025 | 299387 | 13284 |
| 18-Jun | 701940 | 1875796 | 650402 | 3077431 | 30100 | 10274 | 44392 | 132608 | 24224 | 184425 | 297469 | 12927 |
| 18-Jul | 740319 | 1943982 | 683178 | 3229387 | 33824 | 10717 | 47647 | 142359 | 20632 | 222390 | 313703 | 13836 |
| 18-Aug | 799787 | 2186194 | 727566 | 3473204 | 31856 | 13138 | 52114 | 149881 | 20207 | 240156 | 280927 | 17606 |
| 18-Sep | 853391 | 2290216 | 754869 | 3440361 | 38323 | 22720 | 63007 | 171255 | 20665 | 291630 | 245127 | 17506 |
| 18-Oct | 803515 | 2254968 | 740055 | 3374097 | 38738 | 27996 | 66121 | 166784 | 20154 | 316880 | 200439 | 13327 |
| 18-Nov | 718558 | 2069608 | 648514 | 3076557 | 33515 | 19838 | 50157 | 150142 | 20954 | 256961 | 173187 | 12603 |
| 18-Dec | 648337 | 1907330 | 611454 | 2883320 | 24911 | 8217 | 37597 | 154418 | 19332 | 182316 | 161920 | 13027 |
| 19-Jan | 686179 | 1639004 | 575306 | 2895626 | 21813 | 4268 | 30305 | 149579 | 27353 | 158822 | 162888 | 12470 |
| 19-Feb | 640078 | 1645341 | 569909 | 3813163 | 20334 | 2382 | 36250 | 153516 | 20996 | 169448 | 172174 | 11351 |
| 19-Mar | 701015 | 1786303 | 629191 | 3131875 | 21502 | 2919 | 40836 | 164308 | 20010 | 192519 | 214957 | 27057 |
| 19-Apr | 700426 | 1866593 | 640817 | 3141545 | 15868 | 2203 | 38331 | 140434 | 20551 | 174534 | 263588 | 11684 |
| 19- May | 752464 | 2087793 | 694781 | 3471198 | 18779 | 3360 | 41083 | 143818 | 22421 | 200440 | 319861 | 13575 |
| 19-Jun | 755337 | 2124433 | 721481 | 3464597 | 24376 | 6732 | 41580 | 141213 | 22849 | 210881 | 326535 | 11930 |
| 19-Jul | 845104 | 2177848 | 767206 | 3724697 | 28194 | 12126 | 51768 | 158915 | 20660 | 249832 | 335329 | 13279 |
| 19-Aug | 903031 | 2232026 | 810121 | 3744344 | 34913 | 18951 | 65049 | 166547 | 20730 | 307207 | 315993 | 13869 |
| 19-Sep | 943497 | 2293607 | 838354 | 3866960 | 31140 | 31487 | 74914 | 174504 | 22310 | 380334 | 267409 | 19041 |
| 19-Oct | 878571 | 2134394 | 786222 | 3555016 | 31156 | 46730 | 67030 | 167454 | 21175 | 403146 | 216945 | 15102 |
| 19-Nov | 869053 | 2090392 | 782772 | 3443596 | 26179 | 41206 | 56135 | 164036 | 21808 | 284287 | 188179 | 10614 |
| 19-Dec | 855819 | 1931149 | 795053 | 3311131 | 22759 | 18546 | 42296 | 155979 | 20977 | 194387 | 154212 | 13558 |
| 20-Jan | 840458 | 1916716 | 761127 | 3193577 | 17540 | 7782 | 35078 | 152303 | 20390 | 155433 | 155688 | 10966 |
| 20-Feb | 719106 | 1778147 | 613589 | 3046363 | 17097 | 6670 | 38487 | 165303 | 22438 | 171027 | 180727 | 10775 |
| 20-Mar | 643595 | 1601093 | 572698 | 2761780 | 13527 | 2826 | 32485 | 137689 | 23819 | 156460 | 176884 | 11288 |
| 20-Apr | 389987 | 920123 | 351525 | 1849306 | 6821 | 1349 | 11343 | 56325 | 9294 | 61620 | 79227 | 5313 |
| 20- May | 436795 | 1113843 | 406811 | 2046145 | 7076 | 2779 | 13489 | 57399 | 10656 | 68789 | 98533 | 10212 |
| 20-Jun | 481895 | 1292371 | 451571 | 2252284 | 10509 | 4955 | 15582 | 63435 | 10661 | 65750 | 106061 | 6234 |
| 20-Jul | 497378 | 1352235 | 450734 | 2361914 | 22605 | 4768 | 15089 | 72126 | 14188 | 78590 | 104179 | 7758 |
| 20-Aug | 508227 | 1403440 | 468758 | 2425176 | 18978 | 2756 | 16253 | 80182 | 9224 | 83778 | 89278 | 8434 |
| 20-Sep | 552825 | 1531763 | 519696 | 2584574 | 11357 | 3602 | 19960 | 86221 | 10257 | 90296 | 89258 | 9986 |
| 20-Oct | 559988 | 1437472 | 526542 | 2578263 | 14669 | 6422 | 20497 | 85493 | 11685 | 99700 | 84429 | 8980 |
| 20-Nov | 566007 | 1428260 | 516503 | 2530869 | 12853 | 5261 | 21419 | 90168 | 10931 | 88579 | 82289 | 9271 |
| 20-Dec | 533973 | 1384966 | 491615 | 2600425 | 11926 | 3394 | 18576 | 88000 | 13493 | 74787 | 84294 | 14467 |
| 21-Jan | 508088 | 1385723 | 480950 | 2505200 | 8969 | 2708 | 20724 | 91694 | 14746 | 80713 | 96094 | 10292 |
| 21-Feb | 504279 | 1518640 | 460082 | 2534441 | 11049 | 2881 | 21182 | 95191 | 14801 | 87639 | 113497 | 10389 |
| 21-Mar | 607158 | 1774289 | 540008 | 2860296 | 13821 | 3835 | 25576 | 119992 | 16906 | 105348 | 161084 | 12997 |
| 21-Apr | 534535 | 1631732 | 457325 | 2404670 | 8388 | 4118 | 23880 | 139756 | 12412 | 101448 | 134668 | 9568 |
| 21- May | 416723 | 1456718 | 354881 | 2037041 | 6111 | 3026 | 14949 | 164378 | 9817 | 91453 | 68375 | 7741 |
| Total | 27614161 | 72174649 | 24945573 | 121090894 | 872855 | 393407 | 1509552 | 5415845 | 742661 | 7173524 | 7603860 | 505806 |
| Mean | 673516.1 | 1760357 | 608428.6 | 2953436.4 | 21289.1 | 9595.2 | 36818.3 | 132093.8 | 18113.6 | 174964 | 185460 | 12336.7 |
| No. of Obs. | 41 | 41 | 41 | 41 | 41 | 41 | 41 | 41 | 41 | 41 | 41 | 41 |
| Max. | 943497 | 2293607 | 838354 | 3866960 | 38738 | 46730 | 74914 | 174504 | 27353 | 403146 | 335329 | 27057 |
| Min. | 389987 | 920123 | 351525 | 1849306 | 6111 | 1349 | 11343 | 56325 | 9224 | 61620 | 68375 | 5313 |
Table 1: Statistical analysis with mean number of IPD admissions during Pre-pandemic and Pandemic epoch of study period.
Table1: Total IPD admissions of Public-private-rural-urban health facilities of 36 states and UTs of India registered during different months of the study period (study size of variables).
Participants Inclusion criteria - Any IPD registered on HMIS related to Operational Definition given above.
Exclusion criteria - Any IPD services not related to Operational Definition given above.
- Data sources / measurement The Data source link is given below. - https://hmis.nhp.gov.in/#!/standardReports
- Ethical Consideration This study did not require ethical endorsement and informed consent. The data utilized for this study were publicly available for anyone. This study is in acquiescence with Indian data policy.
- Data Analysis Stata 15.1 and Microsoft office were only utilized for different calculations such as difference in IPD and mean IPD cases as well as for comparison of 24-month pre-pandemic epoch (2018–2019) with 17-month pandemic epoch in 2020-2021, (Table 2 & Figure 2).
- Pre-pandemic Epoch – January 2018 to
- December 2019
- Pandemic Epoch – January 2020 to May 2021
- S.No.
- Variable
- No. of
- Obs.
- Mean
- Std. Err.
- 95 % conf. Interval No. of
- Obs.
- Mean
- Std. Err.
- 95 % conf. Interval
- 1
- Inpatient
- (Male)-
- Children<18yrs
- 24
- 763047.7 17692.6 726447.6 799647.7
- 17
- 547118.6 26767.6 490373.7 603863.6
- 2
- Inpatient
- (Male)- Adults
- 24
- 1968630
- 45900.5
- 1873677
- 2063582
- 17
- 1466325
- 58560.2
- 1342183
- 1590467
- 3
- Inpatient
- (Female)-
- Children<18yrs
- 24
- 688381.6 16763.4 653703.7 723059.5
- 17
- 495553.8 23513.8 445706.7 545400.9
- 4
- Inpatient
- (Female)-
- Adults
- 24
- 3271607
- 69318.7
- 3128210
- 3415004
- 17
- 2504254
- 84495.9
- 2325131
- 2683378
- 5
- Inpatient -
- Malaria
- 24
- 27481.6
- 1332
- 24725.9
- 30237.2
- 17
- 12546.8
- 1114.3
- 10184.4
- 14909.1
- 6
- Inpatient -
- Dengue
- 24
- 13511.4
- 2584.5
- 8164.8
- 18858
- 17
- 4066.5
- 412.1
- 3192.9
- 4940.2
- 7
- Inpatient -
- Typhoid
- 24
- 47707.6
- 2426.5
- 42687.8
- 52727.4
- 17
- 21445.2
- 1861.3
- 17499.3
- 25391.1
- Inpatient -
- Asthma, Chronic
- Obstructive
- Pulmonary
- Disease (COPD),
- Respiratory infections
- 8
- 24
- 152924.6
- 2472.1
- 147810.6 158038.6
- 17
- 102685.6
- 8866.8
- 83888.7
- 121482.4
- 9
- Inpatient -
- Tuberculosis
- 24
- 21122.6
- 384.9
- 20326.1
- 21919
- 17
- 13865.7
- 1108.4
- 11516
- 16215.4
- Inpatient -
- Pyrexia of unknown origin (PUO)
- 10
- 24
- 229671.4 13979.7 200752.2 258590.7
- 17
- 97730
- 7916.9
- 80946.8
- 114513.2
- 11
- Inpatient -
- Diarrhoea with dehydration
- 24
- 237470.6 12884.5 210816.9 264124.3
- 17
- 112033.2
- 8727.7
- 93531.2
- 130535.3
- 12
- Inpatient -
- Hepatitis
- 24
- 14213.9
- 709.4
- 12746.3
- 15681.5
- 17
- 9686.5
- 546.4
- 8528
- 10845
Table 2: Statistical analysis with mean number of IPD admissions during Pre-pandemic and Pandemic epoch of study period.
For determining the magnitude of IPD count change due to the pandemic, we compared it to the pre- pandemic mean IPD for above mentioned 12 variables; (Table 3 & Figure 3). The period prevalence for IPD admissions were taken as a count of inpatient admissions during specified period divided by the total population during that period (population source- The World Bank data 2018-2021[27]).
Results
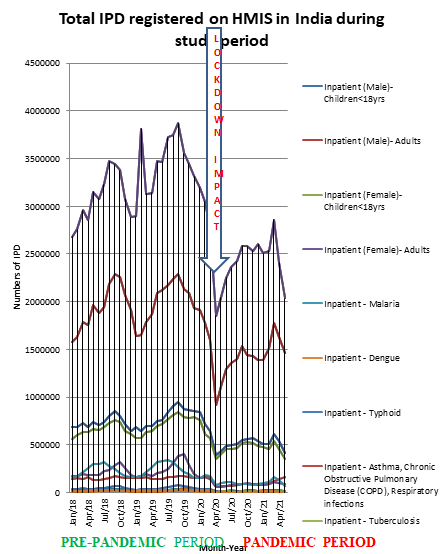
The total numbers of IPD of different variables mentioned above during the study period is presented as Table 1 and Figure 1. The Figure 1 is also highlighting lockdown period impact on IPD. The GoI (Government of India) enforced an obligatory nationwide lockdown from 25th March 2020 ending on 31st May 2020. The figure-1 clearly demonstrates an unusual decline/dip in IPD admissions count during this lockdown period highlighted with an arrow. Figure 2 show that all mean IPDs under study reduced during COVID-19 era of this study.
The total registered IPD during the study period were Table 1
- 27614161number of Inpatient (Male)- Children<18yrs;
- 72174649 number of Inpatient (Male)- Adults;
- 24945573number of Inpatient (Female)- Children<18yrs;
- 121090894 number of Inpatient (Female)- Adults;
- 872855 number of Inpatient of Malaria,
- 393407 number of Inpatient of Dengue,
- 1509552 number of Inpatient of Typhoid,
- 5415845 number of Inpatient of Asthma, Chronic Obstructive Pulmonary Disease (COPD), Respiratory infections,
- 742661 number of Inpatient of Tuberculosis,
- 7173524 number of Inpatient of Pyrexia of unknown origin (PUO),
- 7603860 number of Inpatient of Diarrhoea with dehydration,
- 505806 number of Inpatient of Hepatitis Outcome data The outcome data of this study is presented as Tables 2-4 and Figures 2-4 for easy visualization of readers.
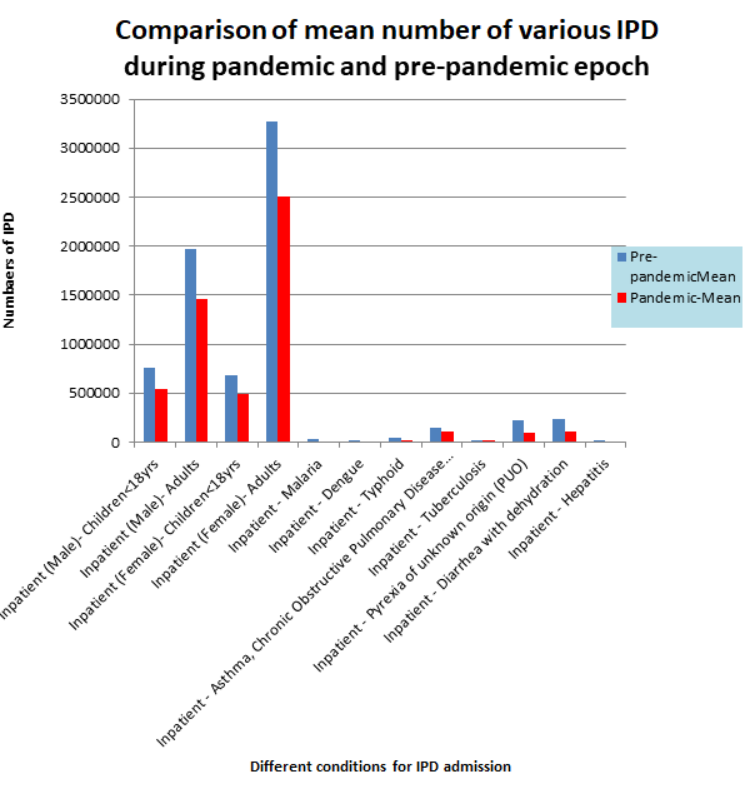
Table-2, 3, 4 and figure-2, 3, 4 demonstrates that the mean IPD admissions during COVID-19 period were 5387311 whereas the mean IPD admissions for pre-pandemic period were 7435770.
The mean IPD admission reduced by 2048459 numbers during COVID-19 pandemic period of this study or in percentage reduced by 27.55% presented as Table 2 and Figure 2 for easy visualization. This study found that there is a significant reduction in various IPD admissions for medical conditions other than COVID-19, during the COVID-19 period which must be a matter of concern for important stakeholders of the health system in the light of our knowledge that it is possible to reduce the burden of disease in a small period.
Comparison of various IPD hospital not admissions during Pre-pandemic and Pandemic period
Inpatient (Male) - Children<18yrs
During the Pre-pandemic Epoch the mean IPD admissions for Male Children <18yrs was 763047.7 (Std. Err.-17692.6; 95 % conf. Interval-726447.6 -799647.7) whereas during Pandemic period it was 547118.6 (Std. Err.-26767.6; 95 % conf. Interval - 490373.7-603863.6), presented as Table 2 and Figure 2 for easy visualization.
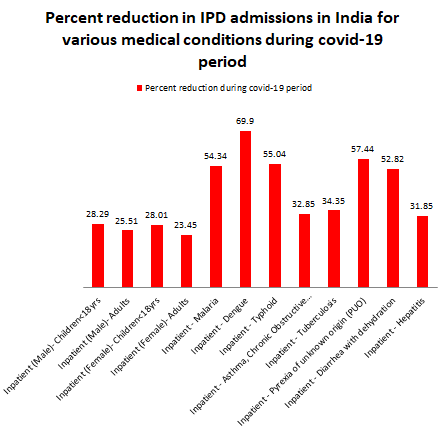
The mean IPD for Inpatient (Male) - Children<18yrs reduced by 215929.1 numbers or 28.29 % during covid-19 period as compared to Pre-pandemic period, presented as Table3 and Figure3 for easy visualization.
| Variable | Pre-pandemic Mean | Pandemic- Mean | Decrease in mean IPD during covid-19 period | Percent reduction during covid-19 period |
|---|---|---|---|---|
| Inpatient (Male)- Children<18yrs | 763047.7 | 547119 | 215929.1 | 28.29 |
| Inpatient (Male)- Adults | 1968630 | 1466325 | 502305 | 25.51 |
| Inpatient (Female)- Children<18yrs | 688381.6 | 495554 | 192827.8 | 28.01 |
| Inpatient (Female)- Adults | 3271607 | 2504254 | 767353 | 23.45 |
| Inpatient - Malaria | 27481.6 | 12546.8 | 14934.8 | 54.34 |
| Inpatient - Dengue | 13511.4 | 4066.5 | 9444.9 | 69.9 |
| Inpatient - Typhoid | 47707.6 | 21445.2 | 26262.4 | 55.04 |
| Inpatient - Asthma, Chronic Obstructive Pulmonary Disease (COPD), Respiratory infections | 152924.6 | 102686 | 50239 | 32.85 |
| Inpatient - Tuberculosis | 21122.6 | 13865.7 | 7256.9 | 34.35 |
| Inpatient - Pyrexia of unknown origin (PUO) | 229671.4 | 97730 | 131941.4 | 57.44 |
| Inpatient - Diarrhoea with dehydration | 237470.6 | 112033 | 125437.4 | 52.82 |
| Inpatient - Hepatitis | 14213.9 | 9686.5 | 4527.4 | 31.85 |
Table3: Comparison of the mean IPD hospital admissions of Pre-pandemic and pandemic period for 12 variables of this study.
Inpatient (Male)-Adults
The mean number of IPD hospital admissions during the Pre-pandemic period of Inpatient (Male) -Adults was 1968630 (Std. Err. - 45900.5; 95 % conf. Interval-1873677-2063582) whereas during Pandemic it was 1466325, (Std. Err. - 58560.2; 95 % conf. Interval -1342183-1590467), presented as Table 2 and Figure 2 for easy visualization.
The mean IPD hospital admissions of Inpatient (Male)- Adults decreased by 25.51 % or 502305 numerically during covid-19 as compared to Pre-pandemic period, (Table 3 and Figure 3).
Inpatient (Female) - Children<18yrs
The mean number of IPD hospital admissions during the Pre-pandemic Epoch was 688381.6, (Std. Err. - 16763.4; 95 % conf. Interval-653703.7-723059.5) whereas during Pandemic Epoch it was reduced to 495553.8, (Std. Err. - 23513.8; 95 % conf. Interval -445706.7-545400.9), (Table 2 and Figure 2). The mean IPD hospital admissions of Inpatient (Female) - Children<18yrs decreased by 192827.8 or 28.01 % during covid-19 period of this study, (Table 3 and Figure 3).
Inpatient (Female)-Adults
The mean number of IPD hospital admissions in India for Inpatient (Male) – Adults was 3271607, (Std. Err. - 69318.7; 95 % conf. Interval-3128210-3415004) in Pre-pandemic period whereas during Pandemic Epoch of this study it was 2504254, (Std. Err. -84495.9; 95 % conf. Interval -2325131- 2683378). The mean IPD admissions of Inpatient (Female) – Adults reduced by 767353 numbers or 23.45 % during covid-19 compared to Pre-pandemic period of this study. This is the lowest reduction seen among all variables of this study.
Inpatient-Malaria
During the Pre-pandemic Epoch the mean IPD was 27481.6, (Std. Err. - 1332.0; 95 % conf. Interval-24725.9-30237.2) whereas during Pandemic it was reduced to 12546.8, (Std. Err. -1114.3; 95 % conf. Interval -10184.4-14909.1). The mean Inpatient – Malaria admissions decreased by 14934.8 or 54.34 % during covid-19 compared to Pre-pandemic period. Inpatient-Dengue During the Pre-pandemic study period the mean number of IPD was 13511.4, (Std. Err. - 2584.5; 95 % conf. Interval-8164.8-18858.0) it was reduced to 4066.5 during Pandemic Epoch (Std. Err. -412.1; 95 % conf. Interval -3192.9-4940.2).
The mean IPD Inpatient – Dengue reduced by 9444.9 or 69.90 % during covid-19 period of this study compared to Pre-pandemic period. This is the greatest reduction seen among all variables of this research study.
Inpatient -Typhoid
During the Pre-pandemic Epoch the mean number of Inpatient – Typhoid was 47707.6, (Std. Err. - 2426.5; 95 % conf. Interval-42687.8-52727.4) whereas during Pandemic it was reduced to 21445.2, (Std. Err. -1861.3; 95 % conf. Interval -17499.3-25391.1).
The mean IPD Typhoid admissions reduced by 26262.4 or 55.04 % during covid-19 compared to Pre-pandemic study period.
Inpatient - Asthma, Chronic Obstructive Pulmonary Disease (COPD), Respiratory infections
During the Pre-pandemic Epoch IPD hospital admissions in India for Asthma, COPD, Respiratory infections was 152924.6, (Std. Err. - 2472.1; 95 % conf. Interval-147810.6-158038.6) whereas during Pandemic it was reduced to 102685.6, (Std. Err. -8866.8; 95 % conf. Interval -83888.7-121482.4).
The mean IPD for Asthma, COPD, Respiratory infections reduced by 50239 or 32.85 % during covid-19 compared to Pre-pandemic study period, (Table 3 & Figure 3).
Inpatient – Tuberculosis
The mean number of IPD hospital admissions during the Pre-pandemic for Tuberculosis was 21122.6, (Std. Err. - 384.9; 95 % conf. Interval-20326.1-21919.0) whereas during Pandemic it was reduced to 13865.7, (Std. Err. -1108.4; 95 % conf. Interval -11516.0-16215.4).
The mean IPD Tuberculosis admissions decreased by 7256.9 or 34.35 % during covid-19 compared to Pre- pandemic study period.
Inpatient - Pyrexia of Unknown Origin (PUO)
During the Pre-pandemic the mean IPD for Inpatient – Pyrexia of unknown origin (PUO) was 229671.4, (Std. Err. - 13979.7; 95 % conf. Interval-200752.2-258590.7) whereas during Pandemic it was reduced to 97730, (Std. Err. -7916.9; 95 % conf. Interval -80946.8-114513.2).
The mean IPD PUO admissions decreased by 131941.4 or 57.44 % during covid-19 compared to Pre-pandemic study period.
Inpatient - Diarrhoea with dehydration
The mean IPD hospital admissions for Inpatient – Diarrhoea with dehydration during the Pre-pandemic was 237470.6, (Std. Err. - 12884.5; 95 % conf. Interval-210816.9-264124.3) whereas during Pandemic it was reduced to 112033.2, (Std. Err. -8727.7; 95 % conf. Interval -93531.2-130535.3).
Diarrhoea with dehydration mean IPD admissions decreased by 125437.4 or 52.82 % during covid-19 compared to Pre-pandemic study period.
Inpatient-Hepatitis
During the Pre-pandemic the mean number of IPD for Hepatitis was 14213.9, (Std. Err. - 709.4; 95 % conf. Interval-12746.3-15681.5) whereas during Pandemic it was reduced to 9686.5, (Std. Err. -546.4; 95 % conf. Interval -8528.0-10845.0).
The mean IPD Hepatitis admissions decreased by 4527.4 numbers or 31.85 % during covid-19 compared to Pre- pandemic study period.
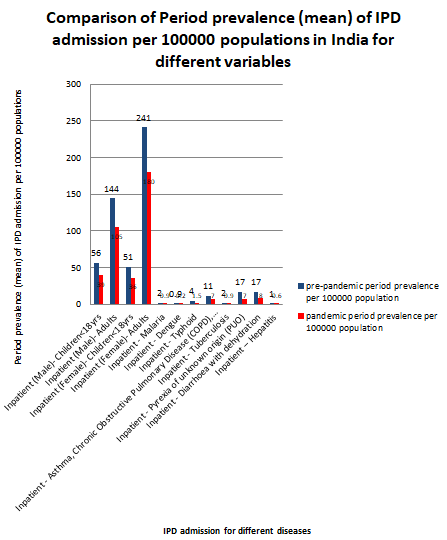
Comparison of Period prevalence (mean) of IPD admission per 100000 populations in India for different variables of this study.
The period prevalence (PP) was calculated by utilizing The World Bank population Data for India.
This Study Revealed that the PP (mean) of IPD Admission for Study Variables Reduced Significantly During COVID-19 as Compared to Pre-Pandemic Study Period which is a Matter of Concern for Stakeholders.
Inpatient (Male) - Children<18yrs
Pre-pandemic PP per 100000 populations was 56 whereas during COVID-19 period it was reduced to 39.
Inpatient (Male) – Adults
Pre-pandemic PP per 100000 populations was 144 whereas during COVID-19 it was reduced to 105 see Tables 4 & 5; Figure 4.
Inpatient (Female)
Children<18yrs - Pre-pandemic PP per 100000 population was 51 whereas during COVID-19 period it was reduced to 36.
| Variable | Pre-pandemic- Mean | pre-pandemic period prevalence per 100000 population | pandemic period prevalence per 100000 population | Pandemic- Mean |
|---|---|---|---|---|
| Inpatient (Male)- Children<18yrs | 763047.7 | 56 | 39 | 547119 |
| Inpatient (Male)- Adults | 1968630 | 144 | 105 | 1466325 |
| Inpatient (Female)- Children<18yrs | 688381.6 | 51 | 36 | 495554 |
| Inpatient (Female)- Adults | 3271607 | 241 | 180 | 2504254 |
| Inpatient - Malaria | 27481.6 | 2 | 0.9 | 12546.8 |
| Inpatient - Dengue | 13511.4 | 0.9 | 0.2 | 4066.5 |
| Inpatient - Typhoid | 47707.6 | 4 | 1.5 | 21445.2 |
| Inpatient - Asthma, Chronic Obstructive Pulmonary Disease (COPD), Respiratory infections | 152924.6 | 11 | 7 | 102686 |
| Inpatient - Tuberculosis | 21122.6 | 2 | 0.9 | 13865.7 |
| Inpatient - Pyrexia of unknown origin (PUO) | 229671.4 | 17 | 7 | 97730 |
| Inpatient - Diarrhoea with dehydration | 237470.6 | 17 | 8 | 112033 |
| Inpatient – Hepatitis | 14213.9 | 1 | 0.6 | 9686.5 |
Table 4: Period prevalence (mean) of IPD admission in India for different variables.
Inpatient (Female)-Adults
Pre-pandemic PP per 100000 populations was 241 whereas during COVID-19 period it was reduced to 180.
Inpatient-Malaria
Pre-pandemic PP per 100000 populations was 2.0 whereas during COVID-19 period it was reduced to 0.9. Inpatient-Dengue Pre-pandemic PP per 100000 populations was 0.9 whereas during COVID-19 period it was reduced to 0.2.
Inpatient-Typhoid
Pre-pandemic PP per 100000 populations was 4.0 whereas during COVID-19 period it was reduced to 1.5.
Inpatient-Asthma, Chronic Obstructive Pulmonary Disease (COPD), Respiratory infections
Pre-pandemic PP per 100000 populations was 11 whereas during COVID-19 it was reduced to 7.
Inpatient-Tuberculosis
Pre-pandemic PP per 100000 populations was 2 whereas during COVID-19 it was reduced to 0.9.
Inpatient - Pyrexia of Unknown Origin (PUO)
Pre-pandemic PP per 100000 populations was 17 whereas during COVID-19 it was reduced to 7.
Inpatient-Diarrhoea with Dehydration
Pre-pandemic PP per 100000 populations was 17 whereas during COVID-19 it was reduced to 8.
Inpatient-Hepatitis
Pre-pandemic PP per 100000 populations was 1.0 whereas during COVID-19 it was reduced to 0.6 see Tables 4 & 5; Figure 4.
- The World Bank Population Data For India
- 2018
- 1352642283
- 2019
- 1366417756
- 2020
- 1380004385
- 2021
- 1399335837 projected
- Pre-pandemic mean population
- 1359530020 pandemic mean population
- 1389670111
Table 5: The World Bank Population Data for India.
Other Analyses This deductive study revealed that all IPD admissions have shown a radical reduction during COVID-19 period illustrated through various tables and figures above. It’s a well-known fact that burden of diseases is increasing by in India. Hence it is apparent from study that a COVID-19 induced situation in India tends to have a disadvantageous impact on medical conditions other than COVID-19 IPD health services utilization.
Discussion
This research study observed a massive drop in IPD admissions during April 2020, after imposition of national lockdown in India. The mean numbers of IPD admission decreased during COVID-19 as compared to pre-pandemic epoch. IPD admissions other than COVID-19 reduced by 27.55 percent in India, during the COVID-19 period of this study. Actually this IPD should have increased due to the fact that COVID-19 aggravates pre-existing medical and social conditions like domestic violence etc. as indirect effect of COVID-19 [28, 29]. There are wide geographical variations in prevalence of COVID-19 in India [30]. The mortality count increased at emergency ward in India, inducing a sense of fear among the population [31]. The prevalence of sexually transmitted disease (STD) was also altered during COVID-19 [32, 33, 34]. IPD admissions are critical for NCD (non- communicable diseases) like cancers as well as incidence of such NCDs are also increasing in India [35]. Due to the above mentioned facts it is questionable that how the IPD admissions decreased during COVID-19. Why? Naturally such question is coming to researcher mind. Possible factors responsible for this reduction in IPD admissions may be
- Lockdown induced reduced mobility.
- Fear of COVID-19 infection at hospital.
- Reduced income due to loss of jobs as indirect COVID-19 impact, leading to reduced OOPE (out of pocket expenditure) capacity.
- Scarcity of bed for IPD admissions other than COVID-19 cases.
- Self or family ignorance and social ignorance or negligence.
- Lack of doctors and staff for attending medical conditions other than COVID-19.
- COVID-19 illness and mortality among healthcare workers.
- Disturbance within the hospital system due to pandemic.
- Decrease in the referral rate as a result of reduction in (OPD) outpatient.
- Encouragement by medical insurance companies and others to find alternative way to receive medical care like telemedicine.
- Regular news about the patient death and excessive IPD costs charged by hospital spread through media or non medical healthcare professionals.
A decrease in IPD for conditions which prevalence or incidence is not dependent on COVID-19, may pose a grave risk if left untreated. The question arises what happened to these patients? Like other nations, the response of healthcare in India to this unexpected COVID-19 was to mitigate the perceived requirements of COVID-19. This study of HMIS data revealed that, the pandemic resulted in a universal reduction of IPD services utilization of all study variables. The future consequences of this reduction in IPD services utilization in India may augment mortality rates in the coming years for diseases other than COVID-19. Added to this COVID-19 hampered several other essential health services utilization as direct/indirect impact of COVID-19 [36, 37, 38, 39, 40]. The readers may love to read key researcher other papers discussing COVID-19 impact on health services available at WHO Covid-19 research database [41].
Future VERSION of this research study will try to reveal that up to what time and magnitude IPD services recovers during upcoming years.
The influence of COVID-19 on patients of chronic medical conditions who require regular IPD care may be of grave consequences. It is quite predictable that the majority of the population could not manage to pay for private hospitals due to cost factors. Patients recently diagnosed with NCDs may not be able to get the IPD treatment, as well as previous NCDs patients missed their regular therapy. It is quite obvious from this study that patients with conditions other than COVID-19 will face an amplified risk in coming years for complications, morbidity and mortality owing to missed IPD services utilization. Deferred initiations and interruption in treatment may augment NCDs disease progression, reappearance, as well as stress, and premature mortality with morbidity.
COVID-19 epoch negative impact on IPD is due to factors, such as health workers shifting for the COVID-19 pandemic control, etc [42]. The IPD decline may be due to prior information of COVID-19 by media and channels which may have prejudiced health-seeking behaviour.
Strength and Limitations of this Study
The strength of this study is the data set on IPD activity for all HMIS (MoHFW) registered hospitals in India. Furthermore this is a unique attempt to describe the bearing of SARS-CoV-2 pandemic on IPD in India. A limitation of this study is lack of data from any other source as well as lack of data for other significant medical conditions.
Conclusions and Recommendations
The HMIS data should be more regular and frequent for making judicious decision in responding to emergencies like COVID-19. Moreover, an in-depth HMIS data set can make us available insights into epidemiology, utilization patterns, and burden outcomes like mortality rates. There is room for improvement in HMIS data. The lesson learnt from this pandemic is the need to prepare strategies and policies whereby the reaction to pandemics is not at the cost of other health care needs. One area for upgrading is timeliness and health authorities need to take into description the population health needs, equity and notify the public accordingly [43]. The strategy should take into account an evaluation of the negative consequences to population health needs if already existing healthcare resources are shifted from one care need to another. For hospitals, the framework or action plan would denote that their reaction to pandemic situations is phased-in and in line with clinical need. The framework should be prearranged around specialist with the aim to reduce disruption to the prerequisite of other medical conditions. This requires the orderliness of hospitals with flexibility in their ability to react to different conditions, and for providing a safe patient environment at times of distress. Telemedicine and well-targeted information drive to educate the community of consequences of not seeking care may improve outcome. The states at bottom ranks in the NITI AAYOG health index report must be focussed more by the centre [44, 45]. The Government of India advised all the states for PHMC establishment by the end of 2022 [46].
The civil registration system of birth and death should be improved with transparency for satisfaction of the accredited organizations like WHO [47].
We Recommend the Following:
- Governments of India should make strategies on priority to trim down burden of morbidity and mortality, in order to reap the benefits of Demographic Dividend. The COVID-19 management should not be prioritized at the cost of other NCDs and CDs.
- Government need a robust and flexible framework to respond to distress with considerations of rigorous restrictions which interrupt routine essential health services, leading to a vicious cycle on the health need of population.
- Government of India should focus on proper and timely data collection.
- The states of India must comply with the central government guidelines [48, 49, 50, 51].
Funding
The author declares that no fund has been taken for this research study from any individual or agencies.
Declarations
This version of paper has not been previously published in any peer reviewed journal and is not currently under consideration by any journal. The document is Microsoft word with English (India) language and 8059 words Total including all. Ethics approval and consent to participate: Not applicable. This study has not involved any human or animals in real or for experiments. The submitted work does not contain any identifiable patient/participant information. Consent for publication: The author provides consent for publication. Availability of data and materials: Electronic records from HMIS (health management information system) of MoHFW (ministry of health and family welfare), Government of India. Conflicts of Interest/ Competing Interest: There are no conflicts / competing of interest Authors’ contributions: The whole work is done by the key Author - Dr Piyush Kumar, M.B.B.S., E.M.O.C., P.G.D.P.H.M., -Senior General Medical Officer- Bihar Health Services- Health Department- Government of Bihar, India, and Co- authors, Advocate Anupama, Senior Lawyer, Bar-council, Patna, Bihar, Dr Abhishek Sinha, Dr. Priyanka Verma, Dr Alok and Harshika Singh. Acknowledgements I am thankful to Advocate Anupama my wife and daughters Aathmika-Atheeva for cooperation. Author information: The author is currently working as Senior General Medical Officer for the government of Bihar.
References
-
Moynihan R, Sanders S, Michaleff ZA (2021) Impact of COVID-19 pandemic on utilisation of healthcare services: a systematic review. BMJ Open 11(3): e045343.
-
World Health Organization (WHO) Home/News/ COVID-19 continues to disrupt essential health services in 90% of countries.
-
Webster P (2020) Virtual health care in the era of COVID-19. Lancet. 395(10231): 1180-1181.
-
Vaishya R, Sibal A, Kumar AP (2020) Severe impact of COVID-19 pandemic on non-COVID patient care and health delivery: An observational study from a large multispecialty hospital of India. 73(2): 159-163.
-
Gasch-Illescas A, Calle-Serrano M, Vallejo-Vaz AJ (2023) Impact of the first wave of the COVID-19 pandemic on non-COVID inpatient care in southern Spain. Sci Rep 13: 1634.
-
Santi L, Golinelli D, Tampieri A, Farina G, Greco M, et al. (2021) Non-COVID-19 patients in times of pandemic: Emergency department visits, hospitalizations and cause-specific mortality in Northern Italy. PLoS ONE 16(3): e0248995.
-
Chapter-4 In-Patient Services.
-
Bryan E, Christensen Ryan P (2020) Fagan-CDC- EIS-Epidemiology Training & Resources-Chapters- Healthcare Settings.
-
WHO Timeline COVID-19.
-
Sharma A, Tiwari S, Deb MK, Marty JL (2020) Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): a global pandemic and treatment strategies. International journal of antimicrobial agents 56(2): 106054.
-
World Health Organization (WHO) COVID-19 Public Health Emergency of International Concern (PHEIC) Global research and innovation forum.
-
Andrews MA, Areekal B, Rajesh KR, Krishnan J, Suryakala R, et al. (2020) First confirmed case of COVID-19 infection in India: A case report. The Indian journal of medical research 151(5): 490-492.
-
Guidelines for containment of COVID-19-Ministry of Home Affairs, Government of India.
-
World Health Organization (WHO) News-COVID-19 continues to disrupt essential health services in 90% of countries.
-
Kasthuri A (2018) Challenges to Healthcare in India - The Five A’s. Indian journal of community medicine: official publication of Indian Association of Preventive & Social Medicine 43(3): 141-143.
-
Kotlar B, Gerson E, Petrillo S (2021) The impact of the COVID-19 pandemic on maternal and perinatal health: a scoping review. Reprod Health 18: 10.
-
Kumar A, Rajasekharan Nayar K, Koya SF (2020) COVID-19: Challenges and its consequences for rural health care in India. Public health in practice (Oxford, England) 1: 100009.
-
Moynihan R, Sanders S, Michaleff ZA (2021) Impact of COVID-19 pandemic on utilisation of healthcare services: a systematic review BMJ Open 11: e045343.
-
Healthy States (2020) Progressive India Report on the Ranks of States and Union Territories.
-
Public Health Management Cadre (2022) Guidance for Implementation.
-
(2022) Ministry of Health and Family Welfare-Excess Mortality Estimates by WHO-India strongly objects to the use of mathematical models for projecting excess mortality estimates in view of the availability of authentic data Validity and robustness of the models used and methodology of data collection are questionable-Posted.
-
Krishnakumar B, Rana S (2020) COVID 19 in INDIA: Strategies to combat from combination threat of life and livelihood. Journal of microbiology, immunology, and infection 53(3): 389-391.
-
COVID-19-Data from Worldometer.
-
Gowd KK, Veerababu D, Reddy VR (2021) COVID-19 and the legislative response in India: The need for a comprehensive health care law. J Public Aff 21(4): e2669.
-
Order-Government of National Capital Territory of Delhi.
-
HMIS-Government of India Ministry of Health and Family Welfare.
-
The World Bank-Population of India.
-
Treskova-Schwarzbach M, Haas L, Reda S (2021) Pre-existing health conditions and severe COVID-19 outcomes: an umbrella review approach and meta- analysis of global evidence. BMC Med 19: 212.
-
Kumar P (2022) What Impact Have SARS-CoV-2/Covid-19 Pandemic on Domestic Violence against Women in India across Different States and Union Territories from the Beginning of Lockdown Due To covid-19 pandemic in March 2020 till 20th September 2020?. J Cli Ped Chi Res 3(1): 78-83.
-
Kumar P(2022) What Impacts Have Geographical Locations On The Cases And Deaths From Covid-19/ SarsCov-2 Pandemic In 36 States And Union Territories Of India:-Observational Analysis In India. J Mari Scie Res Ocean 5(1): 01-07.
-
Kumar P (2022) Impact of COVID-19 pandemic on mortality count at the Emergency Ward of Hospitals in India: A Cross-sectional study from January 2019 to May 2021. pp: 13.
-
Yan J, Li Y, Zhou P (2022) Impact of COVID-19 pandemic on the epidemiology of STDs in China: based on the GM (1, 1) model. BMC Infect Dis 22(1): 519.
-
Kumar P (2022) what is the impact of covid-19 pandemic era on Pregnant Women sero-positivity for Syphilis among women attending antenatal care in India and number of babies diagnosed with Congenital Syphilis?. pp: 8.
-
Kumar P (2022) Impact of Covid-19 Pandemic era on Prevalence of Pregnant Women Sero-Positivity for Syphilis, Among Women Attending Antenatal Care in India and Babies Diagnosed with Congenital Syphilis-A Cross-Sectional Research Study. J Cli Ped Chi Res 3(1): 67-77.
-
Kumar P, Anupama A (2022) Incidence estimate of Cancer Cases in State/UT of India from 2018 to 2021. 7(6).
-
Kumar P, Farooqui HH (2021) What is the Impact of Covid-19 Pandemic on the RCH (Reproductive and Child Health) Programme in Rajasthan, because of nationwide lockdown. pp: 27.
-
Kumar P (2022) Impact of Covid-19 Induced Lockdown on The opd Patients Of Diabetes, Hypertension, Stroke (cva), Acute Heart Disease, Mental Illness, Epilepsy, Ophthalmic, Dental and Oncology In India- A Cross- Sectional Research Study.
-
Kumar P (2022) What is the impact of Covid-19 on the Antenatal Care Services Utilization in Public-Private- Rural-Urban Hospitals of India during the COVID-19 Pandemic Period of 2020-2021 compared to pre- pandemic era 2018-2019?. pp: 27.
-
Kumar P (2022) What is the impact of COVID-19 pandemic era 2020 on Jssk-Janani-Shishu Suraksha Karyakram (mother-child protection program) services utilization in India – A cross-sectional comparative research study?. pp: 21.
-
Kumar P Anupama A (2022) A Impact Of COVID-19 Pandemic Era 2020 on Rashtriya Bal Swasthya Karyakram (RBSK) - National Child Health Program in India-A Cross-Sectional Comparative Research Study
-
Mukherjee A, Parashar R (2020) Impact of the COVID-19 pandemic on the human resources for health in India and key policy areas to build a resilient health workforce. Gates open Res 15(4): 159.
-
Shadmi E, Chen Y, Dourado I, Faran-Perach I, Furler J, et al. (2020) Health equity and COVID-19: global perspectives. Int J Equity Health 19(1): 104.
-
Kumar P, Anupama A (2022) Analysis of NITI AAYOG (National Institution for Transforming India) Health Index Report on the Ranking of States and Union Territories: Round 2 (2015-2016/ 2017-2018)-V2.
-
Kumar P, Anupama A (2022) Analysis of NITI AAYOG (National Institution for Transforming India) Health Index Report on the Ranking of States and Union Territories: Round 1 (2014-2016)-V1.
-
Kumar P, Anupama A (2022) Establishment of Public Health Management Cadre in India and guidelines for implementation.
-
Kumar P, Anupama A (2022) What can be impact of civil authorities’ faulty mortality registration on COVID-19 mortality count in the state of Bihar, India- Evidence from NFHS (National Family Health Survey -5). Adn Envi Was Mana Rec 5(2): 174-178.
-
National Center For Disease Control - COVID -19 Outbreaks - Guidelines for Setting up Isolation Facility/ Ward.
-
Government of India Ministry of Home Affairs (Women Safety Division).
-
Kumar P, Anupama A (2022) what is the impact of the COVID-19 pandemic epoch on IPD (Inpatient Department) hospital admissions in India? - A 41months comparative, quantitative, deductive Cross-Sectional Research Study.
-
Kumar P, Anupama A (2022) What is the impact of the COVID-19 pandemic epoch on IPD (Inpatient Department) hospital admissions in India- A 41 months comparative, quantitative, deductive Cross-Sectional Research Study?.
-
Kumar P (2023) What is the impact of the COVID-19 on Inpatient Department (IPD) hospital admissions in India? - A 41months Cross-Sectional Study.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines