Implications of Young Child Malnutrition on Health and Development: Prioritize Nutrition Interventions in the First 1000 Days of Life
Implications of child undernutrition is not limited to adverse impact on physical growth but on optimum brain growth, mental health and cognitive development. The adverse effects of micronutrient deficiencies in mothers and children are serious with impact on morbidity, mortality, anemia, school performance, overall productivity and national development. Only in the last two decades, studies on the month-wise trend in the prevalence rate of child undernutrition in under five years has drawn attention to the fact that the stunting and underweight rate increases steadily up to 24 months, peaks at about two years of age and then stabilises. Efforts are therefore being directed to the significance of concentrating on implementation of child undernutrition preventive measure in the first 1000 days of life. As per the globally accepted conceptual framework of child malnutrition and the evidence available of effective interventions, emphasis is to ensure universal coverage of selected package of essential nutrition interventions (ENIs) and coupling these with nutrition sensitive interventions. Priority interventions in the first 1000 days comprise nutrition care package linked to antenatal care services, intensive efforts for universal adoption of appropriate infant and young child feeding practices and context specific nutrition sensitive measures .For effective implementation, special attention to mapping of the ’at risk’ households having a member falling in the 1000 days window needs special attention. The contacts of health workers with antenatal care and routine child immunization services need to be effectively used for promoting appropriate maternal nutrition care and breastfeeding and complementary feeding practices in the first 1000 days of life. Along with universal coverage of ‘at risk’ households with ENIs, it is imperative to ensure that the context specific nutrition sensitive interventions are simultaneously addressed, as reflected in the design of India’s National Nutrition Mission/Poshan2.0.
Introduction
Undernutrition reduces chances of survival and adversely affects ability of young children to grow optimally, both physically and mentally. Persistently high level of stunting, wasting and underweight in children in India remains a serious concern. Malnutrition has serious implications throughout the life cycle, adversely affecting health, education, productivity and economy of a country. Design of a nutrition programme therefore needs to prioritize selected package of interventions and reach the right target group at right time to prevent malnutrition and facilitate optimum development. The chapter presents implications of malnutrition on overall development and the rationale of designing programme that focus on the first 1000 days of life with selected doable interventions that could make a difference.
Malnutrition and Development
Malnutrition, comprising undernutrition, overweight/ obesity and micronutrient deficiencies, have serious consequences on child morbidity, mortality and development [1]. Maternal-Child malnutrition is the leading risk factor for disease burden. Globally, maternal and child undernutrition is estimated to be the underlying cause of nearly half of under-five child deaths [2, 3]. In India, 68% of under-five deaths are associated with undernutrition [4]. Undernutrition in children is estimated to reduce a nation’s economic advancement by at least 8% due to its impact on young child mortality, increasing incidence of morbidity, direct productivity losses, poor cognition and reduced schooling [5]. Based on analysis of demographic and health survey data of a number of countries, an association between height and cognitive development gradient has been reported [6]. Undernutrition impairs brain development and cognitive abilities during the early days with implications on delayed school enrolment, high school drop-out rate as well as poor performance in school and lower learning outcomes [7]. A multi-country study analysis reveals that for every 10% increase in the prevalence rate of stunting, the proportion of children reaching the final grade of school dropped by almost 8% [8]. Undernutrition in early childhood therefore adversely influences school concentration, learning at school, livelihood actions and productivity through the life cycle leading to intergenerational cycles of poverty and malnutrition. WHO estimates that reduced school attendance of stunted children results in reduced earning capacities equal to an average 22% loss of yearly income in adulthood [9]. The implications at the macro level are grave—annual losses of around 10% of Gross Domestic Product (GDP). Poor nutrition of pregnant women adversely affects growth of foetus and contributes to intrauterine growth retardation (IUGR) and low birth weight (LBW) and this in turn increases the occurrence of a wide range of metabolic disorders and chronic diseases when adults [10, 11]. It is postulated that a mechanism for survival results in the adaptation of IUGR foetus or offspring to in vitro or extra- uterine environments with evolutionary advantages for survival, resulting in inappropriate programme offspring with adverse consequences in adulthood [12]. Today, under nutrition in early childhood is recognised to be an important factor for increasing the chances of adult-onset chronic diseases such as diabetes, cardiovascular diseases, etc. with negative impact on work capacity, health expenditure and earnings.
Deficiencies of various micronutrients, often referred to as “hidden hunger,” have grave consequences on health, education and development. Nutritional anaemia is caused by deficiencies of one or all of the following micronutrients -iron, Folic acid and vitamin B12.The implications of iron deficiency and anaemia are serious across all age groups, but are of special concern during pregnancy and early childhood. Anaemia not only contributes to high morbidity and mortality but also reduces performance and productivity. It is estimated that a population increase in maternal haemoglobin by 1g /dl could reduce the risk of maternal mortality by approximately 25% [13]. Maternal iron deficiency anaemia prior to and early pregnancy places mothers at increased risk of significant decrements in foetal growth, preterm birth or low birth weight babies [14, 15]. Incidence of LBW doubles with Hb <8 g/ dl [16]. Moreover iron deficiency in perinatal and neonatal stages adversely impacts cognitive outcome. Iron deficiency in foetal stage for an extended period is reported to adversely affect brain development with a high chance of the damage being irreversible [17]. In children, anaemia results in poor attention span and concentration at work, resulting in lowered school performance. Deficiencies of other micronutrients such as vitamin A and zinc have serious impact on the immunity, survival and growth of children. Folic acid and iodine deficiencies also adversely influence the brain and cognitive development of foetus and young children. Folic acid deficiency in women in reproductive age is known to be a contributory cause of neural tube defects [17, 18]. Iodine deficiency during pregnancy can cause dysfunction of the thyroid gland and may impair neurological development in foetus, brain damage and lowering of intelligence quotient (IQ) in school children by about 11 IQ points [19].
Undernutrition in children on young child mortality, increased incidence of morbidity, direct productivity losses, poor cognition and reduced schooling is estimated to reduce a nation’s economic advancement by at least 8% [5]. As per WHO estimates, reduced school attendance of stunted children results in reduced earning capacities equal to an average 22% loss of yearly income in adulthood [9]. The implications at the macro level are grave—annual losses of around 10% of Gross Domestic Product (GDP).
Young Child and Maternal Malnutrition: The Current Situation in India
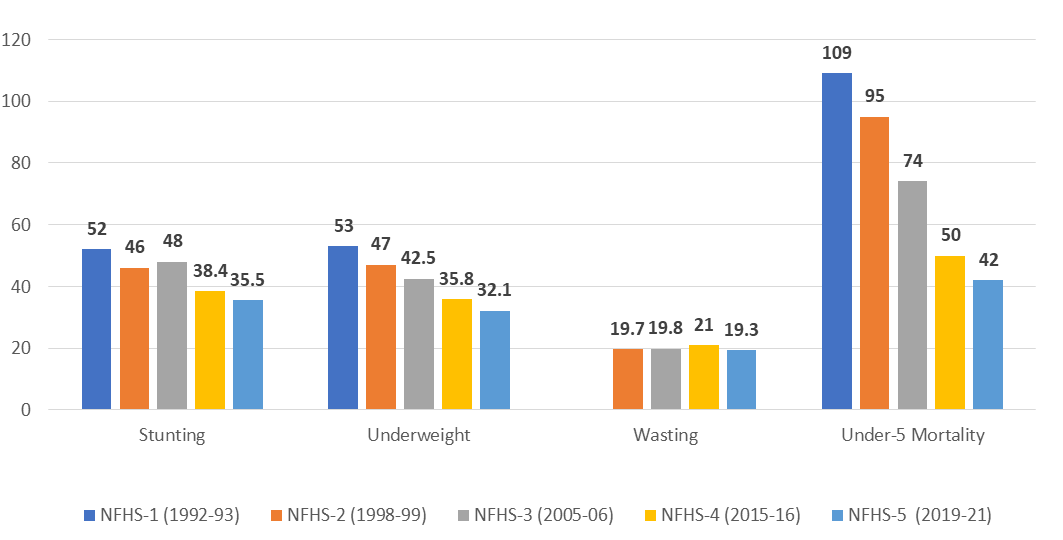
Figure 1 indicates the trends in undernutrition and mortality in under-five children as per the National Health and Family Surveys (NFHS) surveys conducted between
1992 and 2019-21 [20, 21, 22, 23, 24]. The nutritional status of young children under five years have shown a consistent decline in the stunting and underweight rates but the situation continues to remain grave. As per 2019-21 survey report, over 35 % children in India are stunted while 32.1% are underweight. Under five child wasting rates in fact is noted to have remained consistent with a fifth of under five years’ children in the wasted category. There is a wide difference noted in the situation of undernutrition rate amongst the Indian states [NFHS 5]. Some children suffer from more than one form of malnutrition such as wasting and stunting or stunting and overweight with or without anaemia or other micronutrient deficiencies [25].
First 1000 Days of Life: Window of Opportunity
In 2001, for the first time in India, the month-wise trend of prevalence rate of underweight in under two years children was reported from the State Government of Uttar Pradesh on the basis of a survey undertaken for the state government by the Institute of Applied Statistics and Development Studies (IASDS) with UNICEF support [26, 27]. The findings drew attention to the fact that there is a substantial increase in the percentage of underweight children with an increase in age in the first two years of life and then the prevalence rate plateaus [26, 27]. The study concluded, “There is a need to accord highest priority to care and feeding (breastfeeding and complementary feeding) below one year. Intervention measures, if delayed beyond this critical period of infancy, maybe too late for effective prevention of malnutrition in children” [28]. This led to the piloting of a project designed to focus on under two years children, with a special emphasis on care during pregnancy and the first 12 months of life [29]. At the same time, in 2001, Shrimpton, et al [30], presented the global evidence that undernutrition in children increases steadily in the first 24 months of life as depicted in Fig 2. The global finding was based on the analysis of 39 country data of children 0-59 months relative to the National Centre for Health Statistics (NCHS) reference. Later, using the WHO 2006 Growth standards [31], the global -analysis reconfirmed that the prevalence rate of stunting and underweight increases steadily up to 24 months, peaks at about two years of age and then stabilises. Most growth retardation that occurred by the age of two years was also reported to be largely irreversible [32]. It was also recognised that the first 1000 days of life, from the onset of conception to 24 months of age, is extremely critical since it is not only a period of rapid linear physical growth but also is characterized by rapid and dynamic brain development [33]. Additionally, young children who are stunted or underweight have lower immunity and have a higher chance of falling ill and entering a cycle of under nutrition-infection.
![Figure 2: The global finding was based on the analysis of 39 country data of children 0-59 months relative to the National Centre for Health Statistics (NCHS) reference. Later, using the WHO 2006 Growth standards [31], the global -analysis reconfirmed that the prevalence rate of stunting and underweight increases steadily up to 24 months, peaks at about two years of age and then stabilises. Most growth retardation that occurred by the age of two years was also reported to be largely irreversible [32]. It was also recognised that the first 1000 days of life, from the onset of conception to 24 months of age, is extremely critical since it is not only a period of rapid linear physical growth but also is characterized by rapid and dynamic brain development [33]. Additionally, young children who are stunted or underweight have lower immunity and have a higher chance of falling ill and entering a cycle of under nutrition-infection.](/fulltextimages/10112/fig_2.png)
In 2005-6, India’s National Family Health Survey 3 (NFHS 3) data for the first time confirmed that nationally between 0-24 months of age, the prevalence rate of both underweight and stunting increased with age. The rate of underweight being almost 30% at 6 months and increasing to 32.7% at 9-11 months, 46.9% at 12 -17 months, followed by a sharp increase to almost 58% by 23 months [22]. The rate of childhood stunting showed a much sharper increase between 9 and 24 months. These survey findings also indicated that almost a third of children were born with low birth weight and this led to high percentage of children being underweight, stunted and wasted in the first 1-2 months of life itself. The significance of under two years or first 1000 days life, 270 days of pregnancy and 730 days of 0-24 months, was evident. This undernutrition trend was supported by the World Bank 2005 report on the analysis of findings of the earlier National Family Health Survey 2, 1998- 99 [1, 21]. The report stated “Most growth retardation occurs by the age of two, in part because around 30% of Indian children are born with low birth weight” [1]. It was noted that these children with LBW continued to grow poorly, with a substantial growth faltering and a poor “catch up” growth with a higher chance of remaining stunted at 24 months [14]. In fact, stunting or poor growth occurring during this period of under two years was reported to have implications on the growth pattern during adolescence with a greater chance of growing up to be stunted adults. Available evidence from India indicates that children who are stunted at the age of two fail to reach their optimal height during adolescence [34], the second and last growth spurt stage of life, and this sets up an intergenerational cycle of undernutrition in women.
Analysis of NFHS 4 data in 2015-16, reconfirmed an increase in the percentage of stunted or underweight from birth to first 24 months [23] (Figure 3). In the first month, one in 5 children was stunted or underweight while almost 2 out of 5 children were noted to be wasted. The findings emphasized that by the age of two years most growth retardation takes place and that the “trajectory of length growth after birth seems to be largely set-in uterus” [35]. The significance of maternal nutrition care is therefore evident. This is further supported by studies that indicate an association between prevalence of low BMI in mothers with the rate of low birth weight [36]. Maternal nutrition situation in India in 2019-21, as compared to NFHS 4, shows a reduction in undernourished women with low BMI of 18.5 (18.7 % in 2019-21 as compared to 22.9 % in 2015-16) and an increase in rate of overweight /obese women with BMI 25 and above (24% in 2019-21 against 20.6 in 2015- 16). Both undernutrition and overweight during pregnancy are detrimental to foetal growth and new-born health and nutritional status [37]. Mothers must enter pregnancy healthy with appropriate health and nutrition care during adolescence and in the preconception stage in order to break the intergenerational cycle of malnutrition.
![Figure 3: Trend (percentage prevalence rate) with age of stunting, underweight and wasting in children 0-59 months [23].](/fulltextimages/10112/fig_3.png)
An analysis on the prevalence rate of child stunting or underweight in India, with reference to the four wealth quintiles, also reveals that the trend of increase in the occurrence of undernutrition with increase in age is similar across all the wealth quintiles [22]. However, a difference regarding the rate of undernutrition at the starting points is noted. Length at birth as well as a percentage prevalence rate of stunting in under-five children is noted to be worse off in the most economically disadvantaged population compared to the other three quintile groups. The data also highlights the fact even in the highest wealth quintile groups, almost a fifth of the children are stunted at birth. For prevention of stunting, the findings reveal that attention needs to be directed to address the problem of undernutrition not only in children under two years from the poor socio-economic group, but even in those from high socio-economic group.
These findings confirm that the first 1000 days of life, from minus 9 months to 24 months comprising 270 days of pregnancy and 730 days of the first two years of life, is the “window of opportunity” for preventing linear growth retardation or growth faltering in early childhood in low- and middle-income nations, including India [30]. The significance of taking appropriate evidence- based interventions in the first 1000 days is further supported from a recent global a longitudinal data analysis of growth data from South Asia and Africa. In South Asia, one in three children (31%) who had experienced stunting by 2 years of age were noted to have been stunted at birth or within the first week of birth while a similar percentage (32%) were stunted between 8 days and 6 months of age and in 38 % the onset of stunting was between 6 to 24 months [38, 39]. The findings of the study in the two regions with the highest burden of stunting reconfirmed that “about half of the global burden of stunting in early childhood originates during the 500 days between conception and 6 months of age” [39]. The significance of paying particular attention to the period of rapid fetal growth and 0-24 months, i.e.the first 1000 days of life is evident. Besides this critical period of the first 1000 days of life, for breaking the intergeneration cycle of malnutrition, nutrition care during adolescence, particularly for girls aged 10 to 19 years, also deserves special attention [40].
Besides underweight, stunting and wasting in preschool children, the problem of micronutrient deficiencies are common in children 0-19 years [25]. It is also reported that maternal anemia is a determinant of anemia in children aged 6-59 months [39]. As per the last national survey of NFHS 5 survey of 2019-21, the prevalence rate of anaemia is reported to be highest in under five children with 67.1% preschool children being anaemic compared to 59.1% in adolescents, 57% women in the reproductive age and 52.2% in pregnant women [24].
Focus Interventions in the First 1000 Days of Life: The Way Forward
Malnutrition in children results from multiple, complex and interactive causes as presented in the various conceptual framework models [3, 41, 42]. It is imperative to focus simultaneously on essential direct nutrition interventions and nutrition sensitive interventions with special attention to ‘at risk’ households having a member in the first 1000 days of life i.e. with a pregnant or nursing woman or a child under two years [43]. With such a targeted approach, the task of frontline workers is more focused, manageable and effective for ensuring at least 90 % coverage with evidence based selected essential nutrition interventions (ENIs) and in reaching out for other sectoral inputs for addressing the underlying factors of child malnutrition or nutrition sensitive factors that operate at household and community levels. The latter comprise factors such as household food insecurity, inadequate care of women and children combined with poor birth planning including conception at an early age, short intervals between births and a large family size as well as poor sanitation services, domestic violence, unhealthy environment with lack of ready access to safe drinking water and environmental sanitation. Regarding improving ENIs coverage in the first 1000 days, it is imperative to ensure timely inputs are given for appropriate maternal, neonatal and infant care with special attention to establishing appropriate feeding practices during this period. In India, 70% pregnant women register for pregnancy in the first trimester and 58.1% attend at least 4 ANC services [24]. ANC provides minimum four contacts with health services to 6 out of 10 pregnant women. This is an opportunity that must be seized for maternal nutrition care. Linking maternal nutrition care with ANC is essential. Such a package of ANC linked maternal nutrition care needs to include systematic interventions for promoting consumption of adequate and diversified diet (from at least 5 food groups) and daily use of iodized salt, counselling on weight gain based on BMI recorded in the first trimester, monitoring weight gain, testing of haemoglobin levels, provision and compliance of iron-folic acid (IFA) tablets as per the dosage recommended for prevention and for the treatment of mild or moderate anaemia, timely referral of severely anaemic cases, provision of calcium supplements etc [39, 44]. With the launch of Anaemia Mukt Bharat (literal meaning ‘Anaemia Free India’) in 2018, there is a higher focus in India on the prevention and management of anemia during pregnancy [45]. However, the other ENI measures of maternal nutrition care continue to be mostly absent [46, 47]. Moreover, in addition to ENIs, it is important to also simultaneously address the nutrition sensitive factors that are context specific and applicable to ‘at risk’ households. The latter could range from actions for improving access to diversified affordable food items to interventions for influencing socio-economic situation, water-sanitation services etc. The measures for accessing diversified nutritious diets are complex. The study undertaken in 2019 in low-middle- and high -income countries reveal that the most common limiting factors for women is cost (79%) followed by pressure on their time (62%) and difficulty in finding nutritious diets (30 %) [39, 48].
Besides maternal nutrition, appropriate breastfeeding of new-borns and infants in the first 6 months need special care. Percentage of infants being breastfed within an hour of birth or early initiation of breastfeeding (EIBF) has remained almost stagnant in India--around four in 10 newborns. This is despite the fact that mothers undergoing institutional delivery has increased remarkably from 78.9 % in 2015-16 to 88.6 % in 2019-21 [23, 24]. In order to accelerate EIBF rate, the first doable action that needs attention by the health system is closing the vast gap in the percentage of mothers practising EIBF (41.8%) and those reporting institutional delivery (88.6%). Between 0-6 months, mothers are advised to practice exclusive breastfeeding (EBF). There is an increase in the percentage of mothers reporting EBF-63.7 % in 2019-21 as compared to 54.9 % in 2015-16 [23, 24]. An optimum secretion of breastmilk is often not achieved due to mothers lacking the required breastfeeding skills. Such a situation adversely affects the confidence of mothers and builds in the perception that milk ‘formed’ is insufficient resulting in discontinuation of EBF. A shift in focus from mere promotion of EBF to providing support to nursing mothers for ‘effective’ EBF is imperative. Use of appropriate ‘cross cradle hold’ technique and also practicing the technique of emptying one breast fully before shifting to the next has been reported to make a positive difference in optimum breastfeed transfer to infants and in making a positive difference in the daily weight gain to as high as average 30 grams/day in infants by 3 months of age, even in the case of LBWs [49]. Routine child immunization offers suitable contacts with a reported coverage of 76.4% [24]. Besides ANC, immunisation contact opportunities could also be used effectively by health workers to check and provide inputs for appropriate positioning of infants and use of feeding techniques by mothers while breastfeeding.
Between 6-24 months, the primary challenge is appropriate complementary feeding (CF). Minimum adequacy of complementary feed (a combined measure of frequency and diet diversity) is much lower in India compared to other developing countries [50]. Even though policies and guidelines for Infant and Young Child Feeding (IYCF) practices were issued over a decade back and a number of government health programmes were launched, focus on promoting CF practices remain weak and a persistent challenge. Counselling, on combining continued breastfeeding with appropriate introduction of semisolid from 6 months onwards, is not included in the tasks of the health system. These inputs are not viewed as responsibilities of health workers and can be attributed, to a great extent, to the fact that in India, the Primary Health Care system is accountable for reducing child mortality but not child undernutrition. Moreover, improvement in CF practices is complex and hindered by the fact that for the establishment of appropriate of CF practices, besides providing inputs for influencing mothers’ knowledge, measures are required to be taken to address “child food poverty” -- a state where young children are not fed the bare minimum number of food groups they need in early childhood [51]. Addressing the issue of food poverty situation is therefore multifacted since it implies addressing nutrition sensitive issues such as improving socio-economic status of family and availability of diversified food at affordable prices, discouraging large family size, improving education status and empowering women. These issues for improving CF practices are being addressed to some extent by the National Nutrition Mission or POSHAN Abhiyaan/Poshan2.0 launched since 2018, spearheaded by the Integrated Child Development System (ICDS) under the Ministry of Women and Child. For improving access to diversified diet, the Poshan2.0 programme design provides support for establishment of kitchen gardens for homestead food production. provision of free supplementary nutrition in the form of ‘Take Home Ration’ to young children 7-36 months combined with efforts for intensifying promotion of appropriate selection of food items and feeding practices by execution of a well- planned social mobilisation communication strategy. Additionally, the programme design includes measures for providing context specific various relevant nutrition sensitive services by converging inputs in the identified “at risk” households in the first 1000 days of life [52]. Rolling out of the programme design is hindered to a large extent by the poor convergence of ICDS with primary health care system and this needs to be systematically studied and rectified [53].
A reduction in the prevalence rate of stunting in young children needs to recognised as an investment for overall national development [52]. Enhancing the investment in nutrition intervention measures is crucial since global assessment reveals that for every US dollar invested in scaling up nutrition actions, $16 is realized in return [54]. A cost-effective nutrition intervention programme design, needs to focus on prioritising interventions in the first 1000 days of life and optimally using the contact opportunities provided at the time of delivery of maternal-child health services [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53].
References
-
Gragnolati M, Shekar M, Das Gupta M, Bredenkamp C, Lee YK (2005) India’s undernourished children: a call for reform and action. The World Bank.
-
Bhutta ZA, Das JK, Rizvi A, Gaffey FM, Walker N, et al. (2013) Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost?. Lancet 382(9890): 452-477.
-
Black RE, Victora CG, Walker SP, Bhutta AZ, Christian P, et al. (2013) Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 382(9890): 427-451.
-
India State-Level Disease Burden Initiative Malnutrition Collaborators (2019) The burden of child and maternal malnutrition and trends in its indicators in the states of India: the Global Burden of Disease Study 1990–2017. The Lancet Child & Adolescent Health 3(12): 855-870.
-
Gillespie S, Haddad L, Mannar V, Menon P, Nisbett N, et al. (2013) The politics of reducing malnutrition: building commitment and accelerating progress. Lancet 382(9891):552-569.
-
Ministry of Finance (2016) Mother and Child, Chapter 5, Ministry of Finance, Government of India pp 84-95.
-
Victora CG, Adair L, Fall C, Hallal PC, Martorell R, et al. (2008) Maternal and Child Undernutrition: consequences for adult health and human capital. Lancet 371(9609): 340-357.
-
Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, et al. (2007) Developmental potential in the first 5 years for children in developing countries. The lancet 369(9555): 60-70.
-
(2016) WHO recommendations on antenatal care for a positive pregnancy experience. World Health Organization.
-
Abu-Saad K, Fraser D (2010) Maternal nutrition and birth outcomes. Epidemiologic reviews 32(1): 5-25.
-
Kajantie E, Osmond C, Barker DJ, Forsén T, Phillips DIW, et al. (2005) Size at birth as a predictor of mortality in adulthood: a follow-up of 350 000 person-years. Int J of epidemiol 34(3): 655-663.
-
Wu G, Imhoff‐Kunsch B, Girard AW (2012) Biological mechanisms for nutritional regulation of maternal health and fetal development. Paediatric and perinatal epidemiology 26(1): 4-26.
-
(2004) Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. World Health Organization.
-
Allen LH (2000) Anemia and iron deficiency: effects on pregnancy outcome. Am J clin nutr 71(5): 1280S-1284S.
-
Scholl TO (2005) Iron status during pregnancy: setting the stage for mother and infant. The Am J clin nutr 81(5): 1218S-1222S.
-
World Health Organization (2004) Nutrition Foundation of India, Silver Jubilee Functions, Release of the book “Twenty Five Years: 1980-2005”, New Delhi, India.
-
Cheatham CL (2019) Nutritional Factors in Fetal and Infant Brain Development. Ann Nutr Metab 75(1): 20-32.
-
Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, et al. (2010) Updated national birth prevalence estimates for selected birth defects in the United States, 2004–2006. Birth Defects Research Part A Clin Mol Terat 88(12): 1008-1016.
-
Greene LS, Stanbury JB (1994) A retrospective view of iodine deficiency, brain development and behavior from studies in Ecuador. The damaged brain of iodine deficiency. New York: Cognizant Communication, pp: 173-85.
-
National Family Health Survey (NFHS) 1-1992-93. Ministry of Health & Family Welfare, Government of India.
-
National Family Health Survey (NFHS) 2-1998-99. Ministry of Health & Family Welfare, Government of India.
-
National Family Health Survey (NFHS) 3-2005-06. Ministry of Health & Family Welfare, Government of India.
-
National Family Health Survey (NFHS) 4-2015-16. Ministry of Health & Family Welfare, Government of India.
-
National Family Health Survey (NFHS) 5-2019-21. Ministry of Health & Family Welfare, Government of India.
-
(CNNS) 2019 Ministry of Health and Family Welfare (MoHFW), Government of India, UNICEF and Population Council. Comprehensive National Nutrition Survey.
-
(IASDS) 1999 Nutritional status of women and children in Uttar Pradesh, Institute of Applied Statistics and Development Studies.
-
Vir SC (2006) Mission Poshan: Project to redesign state wide programme strategy for addressing malnutrition in under three in Uttar Pradesh.
-
Vir SC, Nigam AK (2001) Nutritional status of children in Uttar Pradesh. NFI Bulletin, pp: 22:4-6.
-
(2006) Symposium on ‘Nutrition in Late Infancy and Early Childhood (6-24 months),’ Nutrition Foundation of India, New Delhi, India.
-
Shrimpton R, Victora CG, de Onis M, Lima RC, Blössner M, et al. (2001) Worldwide timing of growth faltering: implications for nutritional interventions. Pediatrics 107(5): E75.
-
WHO (2006) WHO child growth standards. Acta Paediatr 95: 1-03.
-
(2004) United Nations System Standing Committee on Nutrition. Fifth Report on the World Nutrition Situation for Improved Development Outcomes.
-
Gilmore JH, Knickmeyer RC, Gao W (2018) Imaging structural and functional brain development in early childhood. Nature Reviews Neuroscience 19: 123-137.
-
Rao S (2012) Maternal and Child Undernutrition in India and Implications for Public Health Policies. Paper presented to Public Health Foundation of India for India Health Report.
-
Shrimpton R (2012) Global policy and programme guidance on maternal nutrition: what exists, the mechanisms for providing it, and how to improve them?. Paediatric and Perinatal Epidemiology 26: 315-325.
-
Mason JB, Saldanha LS, Ramakrishnan U (2012) Opportunities for improving maternal nutrition and birth outcomes: synthesis of country experiences. Food and Nutrition Bulletin 33(S2): S104-S137.
-
Armitage JA, Khan IY, Taylor PD (2004) Developmental programming of the metabolic syndrome by maternal nutritional imbalance: how strong is the evidence from experimental models in mammals? The Journal of physiology 561(Pt2): 355-377.
-
Benjamin-Chung J, Mertens A, Colford JM (2020) Early childhood linear growth failure in low- and middle- income countries. medRxiv.
-
UNICEF (2023) Undernourished and Overlooked, UNICEF NY.
-
Bhatia N, Vir SC (2021) Nutrition care of adolescents: crucial for optimum, growth, development and intergenerational health. In: Vir SC (Ed.), Public Health Nutrition in Developing Countries, 2nd Edition, Woodhead Publishers, India, pp: 649-716.
-
Stewart CP, Iannotti L, Dewey KG (2013) Contextualising complementary feeding in a broader framework for stunting prevention. Maternal & child nutrition 9(S2): 27-45.
-
Vir SC (2021) Undernutrition in children: significance, current situation, determinants, programme principles and intervention package. In: Vir SC (Ed.), Public Health Nutrition in Developing Countries, 2nd Edition, Woodhead Publishers, India, pp: 143-222.
-
Dalal RM, Agnihotri SB (2021) Nutrition Care in the First Year of Life: Significance, Key Experiences and Emerging Lessons in Preventing Growth Faltering and Promoting “Catch Up” Growth. In: Vir SC, (Ed.), Public Health Nutrition in Developing Countries 2nd edition, Woodhead Publishers, India, pp: 499-562.
-
World Health Organization (2016) WHO recommendations on antenatal care for a positive pregnancy experience.
-
MoHFW (2018) Anaemia Mukt Bharat-Operational Guidelines for Intensified National Iron Plus Initiative (i-NIPI) for Programme Managers. Ministry of Health and Family Welfare, Government of India.
-
Sanghvi T, Nguyen PH, Tharaney M, Gosh S, Escobar- Alegria J, et al. (2021) Gaps in implementation and uptake of maternal nutrition interventions in antenatal care services in Bangladesh ,Burkina Faso. Ethiopia and India. Maternal and Child Nutrition 18(2): 1-17.
-
Alive & Thrive, IPE Global, IFPRI (2020) Integrating Maternal Nutrition Into the Government ANC platform: Programmatic Learnings and Recommendations, Alive & Thrive, New Delhi, India.
-
Schmied V, Fleming C, Lala G (2020) Food and Nutrition: Mothers’ Perceptions and Experiences. The State of the World’s Children 2019 Companion Report. Western Sydney University and UNICEF, Sydney, Australia.
-
United Nations Children’s Fund (UNICEF) Fed to Fail? The Crisis of Children’s Diets in Early Life. 2021 Child Nutrition Report. UNICEF, New York, USA.
-
Ministry of Women and Child Development (2022) Saksham Anganwadi and Poshan 2.0. A strategic Intervention to Address malnutrition Concerns. No 11/4/2021-CD-1(e-95706) Ministry of Women and Child Development MoWCD.
-
UNICEF (2022) Child Food Poverty. A nutrition Crisis in Early Childhood, UNICEF, New York, USA.
-
Vir SC, Ranjan A (2021) Investing in Nutrition: Central to Sustainable Development. In: Vir SC (Ed.), Public Health Nutrition in Developing Countries, 2nd (Edn.), Woodhead Publishers, India, pp: 1-39.
-
Vir SC, Suri S (2022) The role of maternal nutrition in reducing childhood stunting. ORF Occasional Paper, pp: 355.
-
(2016) International Food Policy Research Institute. Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines