Investigating Infection Prevention and Control Practices among Healthcare Workers in Kasese District, Uganda: Factors and Implications for Ebola Preparedness
The World Health Organization (WHO) African region often faces numerous public health emergencies, with a significant proportion caused by infectious diseases. Ebola virus disease (EVD) is a high-consequence pathogen of particular concern due to its high mortality rate and potential for global transmission. The study aimed to investigate infection prevention and control (IPC) practices with factors associated with the practice among health care workers (HCWs) in Kasese district, Uganda. The study design was cross-sectional, utilizing both qualitative and quantitative methods. The study population consisted of HCWs working in six selected Health Centre III facilities in sub-counties bordering the Democratic Republic of Congo (DRC). A sample of 106 HCWs was purposively selected and data collection involved structured questionnaires, and then data analysis was done using descriptive statistics and logistic regression. The study reveals that a majority of HCWs were female (55.7%), worked in outpatient departments (49.1%), had 6-10 years of service (43.4%), held certificates as their highest education level (48.1%), and were predominantly nurses (53.8%). IPC practices were found to be low, with 72.6% of participants exhibiting inappropriate IPC practices. Individual factors influencing low IPC practices included the duration of IPC training, knowledge, attitude towards IPC, and education level, all statistically significant (P < 0.05). Similarly, health facility factors such as the accessibility of IPC guidelines and personal protective equipment (PPE), availability of sanitizer/soap, and proper and continuous IPC raining/continuing medical education (CME) were associated with low IPC practice (P < 0.05). In conclusion, the study highlights a low level of IPC practice among HCWs in Health Centre Threes in Kasese District, with both individual and health facility factors contributing to this issue. Recommendations include training HCWs in IPC and organizing regular cascade training, providing IPC knowledge as part of their daily duties, ensuring confidence in managing Ebola during outbreaks, maintaining IPC strategies implemented during EVD outbreaks, and supplying IPC materials to healthcare facilities. These efforts, coupled with increased staffing, can significantly enhance protection and performance in public healthcare services.
Introduction
Ebola virus disease (EVD) is a relatively uncommon but highly deadly viral illness affecting both humans and nonhuman primates. Discovered near the Ebola River in the Democratic Republic of Congo (DRC) in 1976, it has triggered outbreaks across Africa, including Sudan (1976), Gabon (1994 and 1996), Zaire (1995), and Uganda (2000-2001). The 2014-2015 West African outbreak and the 2018 DRC outbreak have underscored its global threat [1].
Globally, EVD has infected 34,796 individuals with a cumulative case fatality rate of 58.1%, all within Africa, particularly in Central, Western, and Eastern regions Shang WJ, et al. [1] Uganda, in East Africa, has grappled with multiple EVD outbreaks since 2000. The most recent outbreak occurred in Mubende and Kasanda districts in 2022, the fifth in Uganda. This outbreak of Ebola Sudan Disease prompted the Ministry of Health (MoH) to declare it in September 2023, following a month of unconfirmed deaths. It resulted in 164 cases (142 confirmed, 22 probable), 55 confirmed deaths, and 87 recoveries WHO [2]. The proximity of the DRC outbreak’s epicenter to Uganda’s border raised concerns due to cross-border movements. Consequently, Uganda’s MoH initiated preparedness activities encompassing coordination mechanisms, community surveillance, health worker training, and infection prevention control campaigns [3, 4].
Twenty high-risk districts in Uganda were designated for intensified EVD preparedness. The Rwenzori region’s health workers underwent extensive training, vaccination, and facility enhancement. Despite the recent Ebola Sudan Virus outbreak, continuous preparedness activities remain pivotal due to border risks [4, 5]. Under Pillar 1 of the response, Uganda’s MoH provided support for infection prevention and control in health facilities, risk communication, social mobilization, and surveillance by communities and health facilities [5, 6].
Despite knowledge about the importance of infection prevention and control (IPC), past studies in Uganda have revealed unprepared healthcare workers and non- adherence to universal IPC precautions. Effective IPC in high-risk districts, including Kasese, is critical to thwart potential outbreaks and protect healthcare workers and the community. IPC measures, if rigorously implemented, can halt virus spread [7].
Uganda’s successful management of previous EVD cases highlights the healthcare system’s determination and resilience, particularly in IPC. However, there is limited information on the factors affecting IPC practices, especially regarding EVD. This study aimed at determining the level of preparedness and explore factors influencing IPC practices among healthcare workers in Health Center IIIs (HC IIIs) in Kasese district, Western Uganda.
Materials and Methods
The Study Location
This study took place in Uganda’s Kasese district, located in the western region with coordinates spanning 00° 12’S to 00° 26’N latitude and 29° 42’E to 30° 18’E longitude. The district covers 3389.8 sq km, comprising 2911.3 sq km of dry land, 409.7 sq. km of open water, and 68.8 sq. km of swamps. It shares borders with Bundibugyo, Kabarole, Kamwenge, Rubirizi, and the Democratic Republic of Congo. Administratively, it’s divided into 4 counties, 1 municipality, 25 sub-counties, and 9 town councils. In 2019/20, the population was 777,000, with 51.7% females and 48.3% males, a density of 183 persons per sq km, and 75.5% residing in rural areas and 24.4% in urban areas. There are 140,697 households.
Study Design and Setting
It was a multicenter cross-sectional study that applied both descriptive and analytical approaches and the study setting was Kasese District in six Health Centre IIIs; Katwe, Musyenene, Kitholhu, Kalambi, Nyabugando, and Kasanga that where nearest to Eastern DRC.
Study Population (Participants)
The study population was Health Care Workers (HCWs) defined as any personnel with specific training requirements working within a health facility such as medical doctors, pharmacists, clinical officers, nurses, laboratory technicians, midwives and nursing assistants were recruited into the study through random selection within each health care facility.
Sample Size and Sampling Technique
The study included 106 participants, and two sampling methods were employed: health Centre III facilities were purposively selected on the basis of their vicinity to the DRC boarder in the DRC-bordering sub-counties, and simple random sampling of healthcare workers within each facility was conducted, ensuring representation from all sections where feasible.
Data Collection Technique
Data collection for this study utilized a preparedness observation checklist, adapted from the WHO’s IPC measures checklist, and a semi-structured questionnaire to assess IPC measures, practices, and related factors among healthcare workers in health facilities.
Ethical Consideration and Quality Control
Ethical approvals were obtained from Uganda Martyr’s University Ethics committee, and administrative clearance was secured from relevant authorities. Informed consent was obtained from individual health workers, and rigorous measures were taken for pretesting, quality control, and research assistant training.
Data Analysis
Data analysis employed SPSS Version 20, employing stepwise logistic regression to identify IPC predictors. Variables significant during bivariate analysis (p-value ≤0.1) were introduced into the multivariate regression model to calculate adjusted odds ratios (AOR) with a 95% confidence interval, considering factors with P-values < 0.05 as predictors. The measurement of the level of IPC practice was conducted using four parameters: Practice of hand washing during all five key moments of hand hygiene, Use of appropriate PPE whenever on duty, Practices of all the components of waste management in the duty station, Practices of environmental cleaning at the duty station. Participants who practiced all four IPC areas were scored 4 and considered as practicing appropriate IPC. Participants who scored less than 4 were considered to have had inappropriate IPC practice, indicating a low level of IPC practice.
Results
Demographic Characteristics of the HCWs
Table 1 presents demographic data of 106 respondents (100% response rate). Most were female (55.7%), aged 31- 35 years (27.4%), and had education up to a certificate level (48.1%). Professionally, 53.8% were Nurse-Enrolled Nurses/ Nursing Officers/Assistant Nursing Officers, 13.2% were Health laboratory personnel, 4.7% Public Health Personnel, and 1.9% pharmacy professionals. Experience-wise, 43.4% had 6-10 years, 18.9% had 11-15 years, and 13.2% had 26+ years. Geographically, 44.3% were from Mpondwe subcounty, and for health facilities, 25.5% were from Kasanga H/C III.
| Sub counties | Frequency | Percentage (%) |
| Katwe | 16 | 15.10% |
| Kalambi | 13 | 12.30% |
| Nyakiyumbu | 15 | 14.20% |
| Mpondwe | 47 | 44.30% |
| Kitholhu | 15 | 14.20% |
| Health Facilities | ||
|---|---|---|
| Katwe H/C III | 16 | 14.90% |
| Kalambi H/C III | 13 | 12.30% |
| Musyenene H/C III | 15 | 14.20% |
| Nyabugando H/C III | 20 | 18.90% |
| Kitholhu H/C III | 15 | 14.20% |
| Kasanga H/C III | 27 | 25.50% |
| Sex | ||
| Male | 47 | 44.30% |
| Female | 59 | 55.70% |
| Department of Work | ||
| Out Patient Department | 52 | 49.10% |
| Maternity Ward | 19 | 17.90% |
| Medical Ward | 12 | 11.30% |
| Laboratory | 11 | 10.40% |
| Antenatal Care Clinic | 6 | 5.70% |
| Others | 6 | 5.70% |
| Years in Service | ||
| 1-5 | 12 | 11.30% |
| 6-10 | 46 | 43.40% |
| 11-15 | 20 | 18.90% |
| 16-20 | 12 | 11.30% |
| 21-25 | 2 | 1.90% |
| 26+ | 14 | 13.20% |
| Highest Education Level | ||
| Degree | 6 | 5.70% |
| Diploma | 41 | 38.70% |
| Certificate | 51 | 48.10% |
| Ordinary Level of Secondary | 8 | 7.50% |
| Professional Status | ||
| Clinician | 14 | 13.20% |
| Nurse | 57 | 53.80% |
| Health Laboratory Personnel | 14 | 13.20% |
| Pharmacist | 2 | 1.90% |
| Public Health Personnel | 5 | 4.70% |
| Others | 14 | 13.20% |
| Age in years | ||
| 18-25 | 18 | 17.00% |
| 26-30 | 16 | 15.10% |
| 31-35 | 29 | 27.40% |
| 36-40 | 11 | 10.40% |
| 41-45 | 14 | 13.20% |
| 46+ | 18 | 17.00% |
Table 1: Demographic Characteristics of the Respondents (n=106).
Source: Primary field data 2023. Table 1: Demographic Characteristics of the Respondents (n=106).
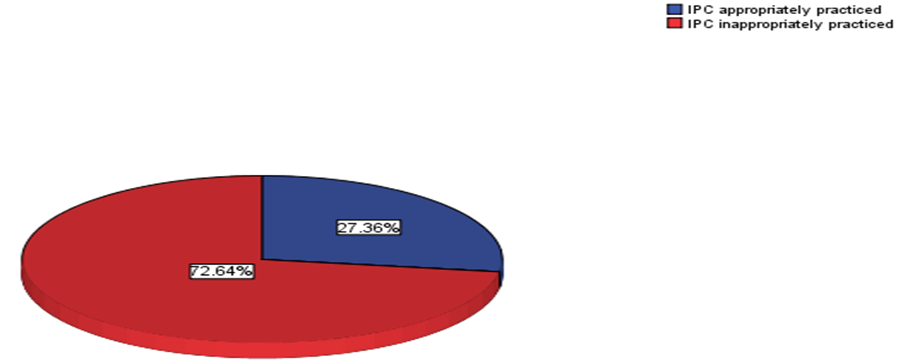
Source: Primary field data 2023. Figure 1: Level of Infection Prevention and control (IPC) in health center Threes in kasese District (n=106).
The Figure1 shows the level of IPC Practice in Health Centre Threes in Kasese District with majority of the health workers and health facilities having inappropriate IPC practices 77 (72.6%) and appropriate IPC was at 29 (27.4%).
Individual Health Workers Factors Associated with IPC Practices
Table 2 illustrates associations between IPC training, knowledge, attitude, education level, and IPC practices among healthcare workers. Regarding the duration of the last IPC training, there was significant association (Ch2 test: 8.934, AOR 0.078, p=0.007). Those trained within <1 year had 15.1% practicing appropriate IPC, while those trained
1-2 years ago had 5.7%. For those trained >2 years ago or not at all, the percentages were 1.9% and 0.9%, respectively. Knowledge about IPC also had a significant impact (Ch2 Test: 6.512, AOR 0.110, p=0.001). Adequate knowledge resulted in 24.5% practicing appropriately, compared to 2.8% for those with inadequate knowledge. Attitude was strongly associated with IPC practices (Ch2 test: 11.685, AOR 0.148, p<0.001). Those with a good attitude had 27.4% practicing appropriately, while those with a bad attitude had none. Education level showed significance as well (Ch2 test: 8.910, AOR 0.072, p=0.003), with varying levels of appropriate IPC practices among degree holders (2.8%), diploma holders (15.1%), certificate holders (9.4%), and those with ordinary secondary education (none).
| Individual Factors | IPC Level | Bivariate | Multivariate | |||
|---|---|---|---|---|---|---|
| Appropriate | Inappropriate | Ch2 Test | P-COR | AOR | P Value | |
| Duration of last IPC Training | 8.934 | 0. 090 | 0.08 | 0.007 | ||
| <1 year | 16 (15.1%) | 18 (17.0%) | ||||
| 1-2 years | 6 (5.7%) | 28 (26.4%) | ||||
| >2 years | 2 (1.9%) | 12 (11.3%) | ||||
| Never Trained | 1 (0.9%) | 23 (21.7%) | ||||
| Knowledge on IPC | 6.512 | 0.121 | 0.11 | 0.001 | ||
| Inadequate | 3 (2.8%) | 50 (47.2%) | ||||
| Adequate | 26 (24.5%) | 27 (25.5%) | ||||
| Attitude towards IPC | 11.685 | 0.159 | 0.15 | <0.001 | ||
| Bad | 0 | 53 (50.0%) | ||||
| Good | 29 (27.4%) | 24 (22.6%) | ||||
| Education Level | 8.91 | 0.081 | 0.07 | 0.003 | ||
| Degree | 3 (2.8%) | 3 (2.8%) | ||||
| Diploma | 16 (15.1%) | 25 (23.6%) | ||||
| Certificate | 10 (9.4%) | 41 (38.8%) | ||||
| Ordinary level | 0 | 8 (7.5%) |
Table 2: Showing Individual Health Workers Factors Associated with IPC Practices (n=106).
Source: Primary field data 2023. Table 2: Showing Individual Health Workers Factors Associated with IPC Practices (n=106).
Health Facility Factors Associated with IPC Practices
Table 3 below outlines the associations between various factors and IPC practices among healthcare workers. The availability of IPC guidelines in facilities was associated with IPC practices but did not reach statistical significance (Ch2 test: 5.056, AOR 0.25, p=0.060). Access to IPC guidelines was significantly related to IPC practices (Ch2 test: 9.583, AOR 0.84, p=0.002). Facilities with Hand Washing Facilities at Work Stations saw better IPC practices, while those without such facilities showed no appropriate IPC. Access to PPEs whenever needed significantly influenced IPC practices (Ch2 test: 7.825, AOR 0.67, p=0.004), with accessible PPEs leading to appropriate IPC practices. Availability of sanitizer/soap also significantly affected IPC practices (Ch2 test: 5.148, AOR 0.41, p=0.022), with facilities having these items demonstrating better IPC. Proper and continuous IPC training/CMEs in facilities were significantly associated with IPC practices (Ch2 test: 10.209, AOR 0.85, p=0.001), with facilities offering such training seeing more appropriate IPC practices.
| Health Facility Factors | IPC Level | Bivariate | Multivariate | ||||
|---|---|---|---|---|---|---|---|
| Appropriate | Inappropriate | Ch2 Test | P-COR | AOR | P Value | ||
| Availability of IPC Guidelines in Facilities | Yes | 28 (26.4%) | 60 (56.6%) | 5.056 | 0.34 | 0.3 | 0.06 |
| No | 0 | 8 (7.5%) | |||||
| Not Sure | 1 (0.9%) | 8 (7.5%) | |||||
| Accessibility of IPC Guidelines in Facilities | Yes | 28 (26.4%) | 52 (49.1%) | 9.583 | 0.93 | 0.8 | 0.002 |
| No | 1 (0.9%) | 25 (23.6%) | |||||
| Availability of Hand Washing Facilities at Work Station | Yes | 29 (27.4%) | 68 (64.2%) | 3.704 | 0.36 | 0.3 | 0.053 |
| No | 0 | 9 (8.4%) | |||||
| Accessibility of PPEs Whenever Needed | Yes | 27 (25.5%) | 51 (48.1%) | 7.825 | 0.76 | 0.7 | 0.004 |
| No | 2 (1.9%) | 26 (24.5%) | |||||
| Availability of Sanitizer | Yes | 27 (25.5%) | 56 (52.8%) | 5.148 | 0.5 | 0.4 | 0.022 |
| /Soap in Facilities. | No | 2 (1.9%) | 21 (19.8%) | ||||
| Proper and Continuous IPC Training/ CMEs done in Facilities. | Yes | 21 (19.8%) | 29 (27.4%) | 10.209 | 0.94 | 0.9 | 0.001 |
| No | 8 (7.5%) | 48 (45.3%) |
Table 3: Showing Health Facility Factors Associated with IPC Practices (n=106).
Source: Primary field data 2023. Table 3: Showing Health Facility Factors Associated with IPC Practices (n=106).
Discussion
Level of IPC Practice
This study found a low level of IPC practice among healthcare workers, with 72.6% practicing inappropriately, while 27.4% practiced appropriately. Those with low IPC practice failed to adhere to hand hygiene during key moments, didn’t use proper PPE, neglected waste management components, and didn’t perform environmental cleaning at their duty stations. These findings align with prior research, including a systematic review of 22 Ebola outbreaks, indicating consistently low IPC adherence in healthcare settings. Similar studies in Liberia, Sierra Leone during the Ebola outbreak, Guinea, and Nigeria also reported low IPC practices among healthcare workers, emphasizing the need for improved IPC training and implementation in healthcare facilities [8, 9, 10, 11, 12].
Practice for EVD among Health Workers in HC IIIs in Kasese District
Individual health worker factors have been identified as significant contributors to the implementation of effective Infection Prevention and Control (IPC) practices for Ebola Virus Disease (EVD) among health workers.
The duration of last IPC Training was associated with level of IPC practice among the health care workers with the Ch2 test of 8.934, AOR= 0.78 and p= 0.007. For instance, this study revealed that training/ mentorship in IPC was done, however, majority of the health workers had last received training more than two years ago and new staff who had served for not more than two years had never been trained on IPC. Although participants expressed a desire to be perceived as experienced practitioners, they did not consistently adhere to infection prevention and control (IPC) policies and procedures. Therefore, regular trainings about IPC are very significant, to equip and update health workers with the necessary knowledge on how to continually practice IPC in their health facilities. The above findings concur with WHO [13] that knowing IPC guidelines among the HCWs is fundamental for effective IPC practice and this should be through regular trainings. In the same way Saqlain, et al. say that, the Ministry of Health should provide a comprehensive IPC training program, targeting all HCWs, to promote all precautionary and preventive measures of pandemic outbreaks. And Mensah et al. affirm that the inclusion of training programs on IPC, in addition to other employee occupational health strategies, can help decrease the risk of infections amongst HCWs.
The study also found out that the knowledge on IPC was associated with level of IPC practice among the health care workers with the Ch2 Test 6.512, AOR 1.48 and p=0.001. The health care workers who had adequate knowledge on IPC only 26 (24.5%) practiced appropriate IP with those that had Inadequate knowledge on IPC; 3 (2.8%) of them practiced appropriate IPC and 50 (47.2%) practiced inappropriate IPC. This findings suggest that having knowledge on IPC
was associated and fundamental for effective IPC practice which was in line with the report and studies from WHO and another IPC study Geberemariyam B, et al. [14] and another IPC study and knowledge about infection risk and behavior’s influenced IPC Level [15]. However, this finding was not in line with the 2 studies that say good knowledge does not necessarily predict good IPC practice [16]. For example, HCWs were found to demonstrate poor compliance with hand hygiene practices despite well-established guidelines for the prevention of HAIs [17].
Attitude towards IPC was associated with the level of IPC practice among the health care workers with the Ch2 test of 11.685, AOR= 1.48 and p< 0.001 with those that had a positive attitude 29 (27.4%) had a appropriate IPC and 24 (22.6%) had inappropriate IPC, and those that had bad negative attitude towards IPC none of them had appropriate IPC and 53 (50.0%) had inappropriate IPC of the total study sample. This study findings were inline with the study that was conducted in Benin City in Nigeria that highlighted that attitude was a significant factor associated with adherence to preventive practices towards EVD among health care workers Onowhakpor AO, et al. [18] and was also in line with the study in healthcare facilities of West Arsi District, Southeast Ethiopia: a facility-based cross-sectional study that showed that positive attitude towards infection prevention practices were two times more likely to have good infection prevention practices compared to those with negative attitude towards infection prevention practices [19]. This was not in line with the studies that were done in Bahir Dar City of Amhara Region, Ethiopia that found that Attitude can be predicted by age. HCWs aged 20-25 were almost three times more likely to have positive attitude than HCW aged more than forty years towards infection prevention practices [20].
Education level of the participants was associated with the level of IPC practices among the HCWs with the Ch2 test of 8.910, AOR= 0.71 and p= 0.003 with those that had degrees 3 (2.8%) had inappropriate IPC, Diploma holders 25 (23.6%) had inappropriate IPC, Certificate Holders 41 (38.8%) had inappropriate IPC, and those that had Ordinary secondary level none of them had appropriate IPC practice. These was in line with the study that was done in Debre Markos referral hospital, Northwest Ethiopia that showed that healthcare workers with high level of education were more likely to practice infection prevention activities. It was also in line with the study that was done in the Palestinian hospitals that showed that healthcare workers with higher educational level had acquired essential information, including infection prevention course [21].
Addressing individual health worker factors is crucial for promoting and sustaining effective IPC practices for EVD among health workers. Training programs may focus on enhancing knowledge, attitudes, and self-efficacy, while providing ongoing support and reinforcement. Organizational support in terms of resource availability, motivation, and recognition can further strengthen adherence to IPC practices. By addressing these individual factors, healthcare systems can improve the overall safety and quality of care provided during EVD outbreaks.
Health Facility Factors Associated with Infection Prevention and Control Practice for EVD in HC IIIs in Kasese District
Health facility factors play a critical role in determining the effectiveness of Infection Prevention and Control (IPC) practices for Ebola Virus Disease (EVD) within health facilities. For instance;
Availability of IPC guidelines in the facilities was associated with level of IPC practice among the health care workers but was not statistically significant in this study with the Ch2 test of 5.056, AOR= 0.25 and p= 0.060. the health facilities that had IPC guidelines in their facilities 60 (56.6%) had inappropriate IPC practice and those who did not have IPC guideline in their facilities none of them had appropriate IPC practice and those that were not sure if their health facilities had IPC guidelines 1 (0.9%) had appropriate IPC practice and this study finding was in line with the study that was conducted in Government Healthcare Facilities in Addis Ababa, Ethiopia that indicated existence of guidelines alone is not sufficient to ensuring appropriate IPC practice among the health care workers this was not in line with the report from WHO that showed that availability of technical IPC guidelines consistent with the available evidence is essential to provide vigorous outline to support the performance of good practices in safe guarding health workers against epidemics and they provide standards for IPC implementation at a health facility [22].
Accessibility of IPC Guidelines in Facilities was associated with level of IPC practice among the health care workers and was statistically significant with the Ch2 test of 9.583, AOR= 0.84 and p= 0.002. Those that did not have access to IPC guidelines 25 (23.6%) had inappropriate IPC of the total study sample these was in line with the study among Healthcare Workers in Governmental Healthcare Facilities in Addis Ababa, Ethiopia [14]. Importantly, the existence of guidelines alone is not sufficient to ensure their adoption and implementation science principles and findings clearly indicate that local adaptation is a prerequisite for successful guideline adoption.
Availability of Hand Washing Facilities at Work Station was also associated with the level of IPC practice in that those facilities that had Hand Washing Facilities at Work
Station 29 (27.4%) practiced appropriate IPC and 68 (64.2%) practiced inappropriate IPC and those that had no hand washing facilities at their stations none practiced appropriate IPC of the total study sample. These was in line with the study in Ethiopia were Healthcare workers working in healthcare facilities with continuous water supply in their department were 1.6 times more likely to have good infection prevention practices compared to HCWs working in healthcare facilities without continuous water supply in their department Sahiledengle B, et al. [19] and was also in line with study systematic review that found out that access to water and other infrastructures directly impact the IPC practice [23]. These was also in line with study among health care workers of private and public hospitals of Bahir Dar city administration, Ethiopia were reliable and uninterrupted provision of good-quality alcohol-based hand rub (ABHR) or supplies of clean water with adequate number of functioning sinks ensured appropriate IPC in the health Facilities [24]. It was also in line with the 2020 global WASH report that revealed that one in three facilities do not have adequate hand hygiene stations at the point of care and hand hygiene compliance was only around 9% during care of critically ill patients in low income countries [25].
Accessibility of PPEs Whenever Needed was associated with the level of IPC practice and it was statistically significant with the Ch2 test of 7.825, AOR= 0.67 and p= 0.004. Health facilities were PPEs were accessible to the staff 27 (25.5%) practiced appropriate IPC and 51 (48.1%) practiced inappropriate IPC and those that did not have access to PPEs whenever they needed them, none of them practiced appropriate IPC of the total study sample this was inline with the study among HCWs in public health facilities of Mekele Special Zone, Northern Ethiopia were Health care workers working in health facilities having continuous supply of PPE are seven times more likely to practice infection prevention compared with those who don’t have continuous supply [26]. It was also in line with the study that was conducted in El Mansoura University Children’s Hospital in Egypt were the absence or insufficiency of basic protective equipment such as masks, gloves and goggles were barriers to compliance to IPC [27]. Availability and supply of infection prevention equipment increases the utilization of those supplies for the prevention of Hospital-acquired infections. Therefore, health workers who get supply of infection prevention equipment (as soap, mask, and infection prevention guideline) have higher odds of practicing infection prevention activities than those healthcare works who did not get infection prevention supplies.
Availability of Sanitizer/Soap in Facilities was associated with the level of IPC practice and it was statistically significant with the Ch2 test of 5.148, AOR= 0.41 and p= 0.022. The health facilities that had available sanitizer/soap for use in the work station 27 (25.5%) practiced appropriate IPC and 56 (52.8%) practiced inappropriate IPC and those facilities were sanitizer/soap was not readily available only 2 (1.9%) practiced appropriate IPC of the study sample. These was also in line with study among health care workers of private and public hospitals of Bahir Dar city administration, Ethiopia were reliable and uninterrupted provision of good- quality alcohol-based hand rub (ABHR) and soap ensured appropriate IPC in the health Facilities [24].
Proper and Continuous IPC Training/ CMEs done in Facilities was associate with the level of IPC practices among health care workers in the health facilities and it was statistically significant with the Ch2 test of 10.209, AOR= 0.85 and p= 0.001. The Health facilities that had Proper and Continuous IPC Training/ CMEs done 21 (19.8%) had appropriate IPC practice and 29 (27.4%) of them had inappropriate IPC practice. Among health facilities that did not have Proper and Continuous IPC Training/ CMEs done only 8 (7.5%) practiced appropriate IPC and 48 (45.3%) practiced inappropriate IPC of the study sample. These was in line with the study that was conducted in a Level Four District Hospital in Kenya where training on IPC improved the level of IPC practice among the health care workers.
Conclusion
This study highlights the low level of IPC practice among healthcare workers in Kasese District, with contributing factors at both the individual and health facility levels. The study underscores the importance of consistent IPC training, promoting a positive attitude toward IPC, and ensuring access to necessary resources and guidelines.
• Recommendations and lessons learned: Based on the findings, several recommendations are proposed.
• Comprehensive and regular IPC Training: The Ministry of Health and district health teams should provide regular IPC training and organize cascade trainings for healthcare workers to improve their knowledge and skills in IPC.
• Resource Provision: Adequate resources, including PPE, sanitizer, and soap, should be provided to healthcare facilities to ensure that healthcare workers can adhere to IPC measures.
• Hand Hygiene Promotion: Promote regular and thorough hand hygiene practices among healthcare workers through education and awareness campaigns.
• Environmental Cleaning: Implement regular cleaning and disinfection protocols for surfaces, medical equipment, and instruments within healthcare facilities.
• Waste Management: Ensure proper waste management practices, including segregation, handling, and disposal of infectious waste.
• Risk Assessment: Healthcare workers should assess the risk of Ebola exposure in their work settings and implement appropriate IPC measures accordingly. By addressing these recommendations, healthcare systems can significantly improve IPC practices among healthcare workers and enhance overall safety during infectious disease outbreaks like Ebola.
Acknowledgement
We would like to express our sincere gratitude to all the healthcare workers in Kasese District, Uganda, who participated in this study. Your cooperation and valuable insights were essential for the success of this research. We also extend our appreciation to the World Health Organization (WHO) and Ministry of Health Uganda for their ongoing efforts to address public health emergencies, including the Ebola virus disease. Additionally, we acknowledge Kasese District health office, for accepting us carry out the research in their health centres. We also acknowledge the support and guidance of our research team and the local healthcare authorities in Kasese District. Their contributions were instrumental in the completion of this study.
Funding
The research was funded by the authors themselves and no external individual or organization funded this research study.
Competing Interests
The authors do not have any conflict of interest in this research.
Ethics Approval
The research study was approved by Uganda Martyr’s University Research Ethics committee.
Data Availability Statement
All the relevant data in this study have been analyzed and reported in the article but data set can be availed on request.
Supplemental Material
Available on request
References
-
Shang WJ, Jing WZ, Liu J, Liu M (2023) Global Epidemic of Ebola Virus Disease and the Importation Risk into China: An Assessment Based on the Risk Matrix Method. Biomedical and Environmental Sciences 36(1): 86-93.
-
WHO (2022) Ebola outbreak 2022-Uganda.
-
Nakkazi E (2019) Death of Ugandan man tests country’s preparedness. The Lancet 393(10174): 863.
-
WHO (2018) Uganda steps up Ebola preparedness response in 22 high-risk districts.
-
MoH (2022) Uganda National Response Plan for ebola virus disease outbreak.
-
UNICEF (2022) Ebola Virus Disease Preparedness in Uganda.
-
WHO (2019) Confirmation of case of ebola virus disease in Uganda.
-
Lohr AM, Ingram M, Nuñez AV, Reinschmidt KM, Carvajal SC (2018) Community–clinical linkages with community health workers in the United States: A scoping review. Health promotion practice 19(3): 349-60.
-
Alhumaid S, Al Mutair A, Al Alawi Z, Alsuliman M, Ahmed GY, et al. (2021) Knowledge of infection prevention and control among healthcare workers and factors influencing compliance: a systematic review. Antimicrobial Resistance & Infection Control 10(1): 1-32.
-
Albano L, Matuozzo A, Marinelli P, Di Giuseppe G (2014) Knowledge, attitudes and behaviour of hospital health- care workers regarding influenza A/H1N1: a cross sectional survey. BMC infectious diseases 14: 1-7.
-
Akagbo SE, Nortey P, Ackumey MM (2017) Knowledge of standard precautions and barriers to compliance among healthcare workers in the Lower Manya Krobo District, Ghana. BMC research notes 10: 1-9.
-
Gichuhi AW, Kamau SM, Nyangena E, Otieno-Ayayo ZN (2015) Health Care Workers Adherence to Infection Prevention Practices and Control Measures: A Case of a Level Four District Hospital in Kenya. American Journal of Nursing Science 4: 39.
-
WHO (2018) Improving infection prevention and control at the health facility: Interim practical manual.
-
Geberemariyam B, Donka GM, Wordofa B (2018) Assessment of knowledge and practices of healthcare workers towards infection prevention and associated factors in healthcare facilities of West Arsi District, South east Ethiopia: a facility-based cross-sectional study. Arch Public Health 12(76): 69.
-
Albano L, Matuozzo A, Marinelli P, Di Giuseppe G (2014) Knowledge, attitudes and behaviour of hospital health- care workers regarding infuenza A/ H1N1: a cross sectional survey. BMC Infectious Diseases 14: 208.
-
Iliyasu G, Dayyab FM, Habib ZG, Tiamiyu AB, Abubakar S, et al. (2016) Knowledge and practices of infection control among healthcare workers in a Tertiary Referral Center in North-Western Nigeria. Ann Afr Med 15(1): 34-40.
-
Allegranzi B, Pittet D (2009) Role of hand hygiene in healthcare-associated infection prevention. J Hosp Infect 73(4): 305-315.
-
Onowhakpor AO, Adam VY, Sakpa OE, Ozokwelu LU (2018) Status of Ebola Virus Disease (EVD) preventive practices among Health care workers (HCWs) in Benin City: a year after disease containment in Nigeria. Pan African Medical Journal 30: 50.
-
Sahiledengle B, Gebresilassie A, Getahun T, Hiko D (2018) Infection Prevention Practices and Associated Factors among Healthcare Workers in Governmental Healthcare Facilities in Addis Ababa. Ethiop J Health Sci 28(2): 177-186.
-
Gulilat K, Tiruneh G (2014) Assessment of Knowledge, Attitude And Practice of Health Care Workers on Infection Prevention in Health Institution Bahir Dar City Administration. Science Journal of Public Health 2(5): 384-393.
-
Fashafsheh I AA, Eqtait F, Harazneh L (2015) Knowledge and Practice of Nursing Staff towards Infect Control Measures in the Palestinian Hospitals. J Educ and Practice.
-
(2015) GM Assessment of the knowledge and practices towards infection prevention and associated factors among healthcare providers of public health facilities in West Arsi, Oromia regional state, Ethiopia.
-
Allegranzi B, Tartari E, Pittet D (2021) Seconds save lives e clean your hands”: the 5 May 2021 World Health Organization Save lives: Clean Your Hands campaign. Journal of Hospital Infection 111: 1-3.
-
WHO (2020) Geneva, USA.
-
Gulilat K, Tiruneh G (2014) Assessment of Knowledge, Attitude And Practice of Health Care Workers on Infection Prevention in Health Institution Bahir Dar City Administration. Science journal of Public Health 2(5): 384-393.
-
Adly R, Amin F, Aziz MA (2015) Improving nurses’ compliance with standard precautions of infection control in pediatric critical care units. World Journal Nursing Science.
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal