Cholera-Free Zambia 2025: A Distant Dream or an Achievable Reality?
Cholera is a virulent infectious disease caused by the bacterium Vibrio cholerae, after ingesting contaminated food and/or water. Body weakness, muscle cramps coupled with acute watery diarrhoea and vomiting are some of the symptoms of cholera. Cholera is still a threat to public health due to its yearly occurrences. Lusaka, Zambia’s capital city is usually the epicentre of cholera outbreaks in the southern African nation. Inadequate solid waste management and sub-standard drainage systems are some of the major causes of cholera outbreaks. At the World Health Assembly held in 2018, Zambia made a bold decision to end cholera within its borders by 2025. Zambia’s progress suggests that a cholera-free future could be an achievable reality. However, sustaining these efforts beyond 2025 will be crucial to cementing gains and ensuring lasting impact. The purpose of this article is to review the progress made thus far, towards a cholera-free Zambia.
Abbreviations
DMMU: Disaster Management and Mitigation Unit; GTFCC: Global Task Force on Cholera Control; MCEP: Multisectoral Cholera Elimination Plan; PWAS: Public Welfare Assistance Scheme.
Introduction
Cholera is a virulent disease that is caused by the bacterium Vibrio cholerae, after ingesting contaminated food or water [1]. The infectious disease is still a major global concern, heavily bearing down on inhabitants of marginalized areas [2]. As of October 2024, a multi-country outbreak has affected seventeen (17) countries in the African Region, with the Democratic Republic of Congo [3], Ethiopia Perspective [4], and Zambia [5] reporting the highest number of cases. A cumulative number of cholera cases recorded from January 1 to September 29, 2024, was 127,283. The World Health Organization (WHO) has described these cases as acute crises [6].
Prolonged dry spells in some areas and extreme flooding in others have made accessing safe and clean water extremely challenging, leading to a surge in water-borne diseases like cholera [7]. As of February 11, 2024, Zambia reported 18,519 cholera cases and 652 deaths, with a case fatality rate (CFR) of 3.5%. Fortunately, new cases decreased by 47.2% to 938, and deaths dropped by 50% to 23 in week 06/2024 compared to the previous week. All 10 provinces were affected, with 70 districts reporting cases. The government activated its highest level of response, coordinated by the Disaster Management and Mitigation Unit (DMMU) under the Vice President’s office. The cholera outbreak severely impacted Lusaka District’s sub-districts, especially peri- urban areas, Luangwa district’s fishing areas [8], Chongwe district’s sewage compound, using well water.
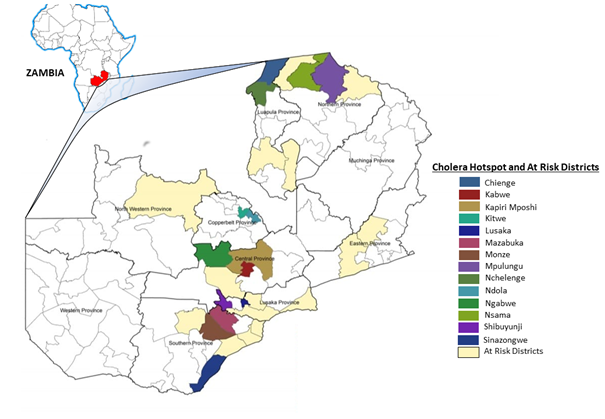
March 10, 2024, an update was given showing cumulative cases rising to 21,330, with 704 deaths and a CFR of 3.3%. New cases decreased by 5.1% to 562, and deaths dropped by 81.8% to two in week 10/2024. By June the same year, nine provinces reported cholera cases, with seven confirming outbreaks. Forty districts confirmed local transmission, with cumulative cases at 23,221 and 740 deaths (CFR 3,2%). That is significantly higher than the WHO-recommended threshold of less or equal to 1%. While Lusaka the Zambia’s major economic hub and densely populated province has seen a notable decrease in cholera cases [9], the eastern part of the country is experiencing an uptick. Chadiza, Chipata, Chipangali, Mambwe, and Lumezi are districts in the Eastern Province of Zambia (Figure 1) that have reported new cholera cases since 29th May 2024 [10].
Zambia’s Roadmap to Eradicate Cholera
In agreement with the mission of the Global Task Force on Cholera Control (GTFCC) to eradicate cholera in endemic regions by the year 2030. Zambia outlined a proactive stance in outlining an organized plan to end cholera within its borders by 2025. This step is backed by the agenda proposed at World Health Assembly held in 2018 that marked the 71st session of member states meeting together. The main objective of this strategic plan is to reduce deaths and ailments associated with cholera, ultimately having a cholera-free Zambia by 2025 [11]. Government ministries, donors and health partners put together collaborative efforts to form the multisectoral cholera elimination plan (MCEP), incorporating useful lessons learned from preceding cholera The MCEP stipulates three strategic axes to attain the goal of zero-laboratory confirmed cholera cases by 2025 (Figure 2). The short-term plan to this course involves the prevention of cholera, with focus on mass campaigns of oral cholera vaccines (OCVs) [13]. Whereas the long-term goal is the elimination of cholera, i.e., recording CFR below 0.5%. To meet the WHO-recommended rate. Formal solicitation of funds to enhance the provision of WaSH facilities in high-risk areas, improved surveillance on case management and local community engagement, are some additional strategies the plan has laid out.
outbreaks. Drawing on experiences and best practices while handling past gaps in the response to the public health threat [12].
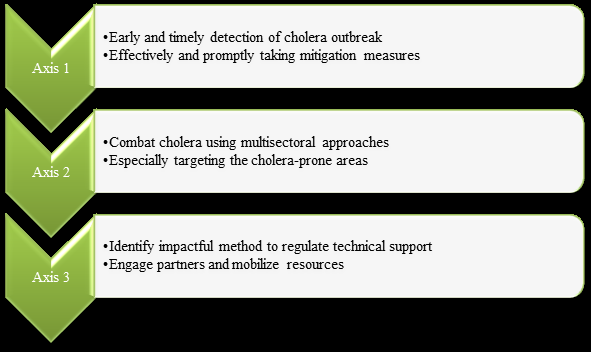
Zambia’s monitoring framework for cholera elimination is structured around the three strategic axes in (Figure 2). This timeline is designed to track progress from 2019 to
2025 [14], with annual evaluations to ensure that the country stays on course to eradicate cholera by 2025 (Table 1).
| Three axes roadmap | Output indicator | Baseline | 2019 | 2022 | 2025 |
|---|---|---|---|---|---|
| Axis 1 | CFR measure of the intensity of cholera outbreaks | 2017/2018 outbreak – CFR = 1.9% | 20% decline in CFR | 50% decline in CFR | CFR not exceeding 0.5% |
| Axis 2 | Eradicate cholera as a threat to public health safety in cholera hotspots | Cholera affecting twelve districts | Cholera to be eliminated in two districts | Cholera to be eliminated in six districts | All twelve districts eliminate cholera |
| Axis 3 | Create a fully funded cholera control plan in agreement with the global elimination roadmap | Lack of a resourceful multisectoral plan to eradicate cholera | Develop a control and apply for sustainable funding | Effectively implement the cholera elimination strategy | Fully establish and adhere to the cholera elimination plan |
| RESULTS: A cholera-free Zambia with a robust population | Decrease in deaths related to cholera | 2,821 reported cholera cases | 30% reduction of cholera cases | 60% reduction of cholera cases | Zero laboratory confirmed cholera cases |
Table 1: Zambia’s monitoring framework and outcome indicators.
To attain this goal, monitoring systems, including activity logs and registers, undergo regular and rigorous review and reporting. Furthermore, impactful studies provide critical insights in the assessment of the efficiency of the multisectoral cholera control plan. The comprehensive approach enables data-driven decision making, ultimately supporting Zambia’s quest to combat cholera [15].
Cholera Response Efforts
Health
An Oral Cholera Vaccine campaign was scheduled to take place in Chipata district from June 16-22, 2024. Additionally, organizations like the United Nations International Children’s Emergency Fund (UNICEF) and WHO are working closely with the government to provide critical supplies, services, and technical assistance to contain the cholera outbreak. This includes vaccination campaigns targeting 1.5 million people, including children, health workers, and those at high risk of infection [16]. Over 1.4 million cholera vaccine doses have been delivered to Zambia, with an additional 200,000 doses approved by the WHO International Coordinating Group on Vaccine Provision.
A comprehensive database has been set up, collecting historical data from all districts over the past 10 years [17]. This will enable targeted interventions and informed decision-making. A thorough review of cholera hotspots has been conducted to guide the roadmap to cholera elimination [7]. This strategic approach will help focus resources on areas with the highest risk of cholera outbreaks. The electronic Integrated Disease Surveillance and Response (eIDSR) system has been introduced in all districts to capture data on Acute Watery Diarrhoea (AWD). This will facilitate early detection and rapid response to potential outbreaks. All general hospitals in the 10 provinces have been capacitated to confirm cholera by culture. This enhanced laboratory capacity ensures accurate diagnosis and effective treatment. These efforts demonstrate Zambia’s commitment to controlling and eliminating cholera. By leveraging data, strengthening surveillance, and enhancing laboratory capacity, the country is well on its way to achieving its goal of cholera eradication by 2025 [18].
Nutrition
UNICEF’s efforts in Lusaka, Zambia, are yielding impressive results in the fight against malnutrition. Through active case finding in all seven sub districts, they have screened 380,288 children aged 6-59 months for wasting, which is roughly 95% of the estimated population in that age group [19]. This initiative has identified 167 severe acute malnutrition (SAM) cases in just one month and referred them for treatment [20]. The organization’s work in Zambia extends beyond Lusaka, addressing social and behavioural issues. Their efforts are crucial in improving the lives of children and communities, especially in settlements affected by drought and cholera.
Child Protection
In Lusaka district, 400 vulnerable households affected by cholera received one-time cash assistance of ZMW 1,200 ($45) through the Government Public Welfare Assistance Scheme (PWAS) to alleviate their cholera- related challenges. These households, along with many others impacted by cholera, also received psychosocial support services through the Lifeline Child Line helpline [19]. This support includes referrals to other protection services, made possible through the partnerships with Access to Health Zambia and the Department of Social Welfare [21]. In the Copper belt province, specifically in Chililabombwe, Kitwe and Ndola districts, home visits are underway by Community Welfare Assistants Committees (CWACs). These visits aim to identify and assess affected children and families, determining their eligibility for in- kind support services and protection services. These efforts demonstrate the ongoing commitment to supporting low resource households and individuals affected by cholera in Zambia. Education UNICEF has made significant strides in promoting water, sanitation, and hygiene (WaSH) in Zambian schools [22]. Recently, they provided essential WaSH items and educational materials to 182 schools in Ndola, Chililabombwe and Kitwe districts. This brings the total number of supported schools to 481, benefiting over 750,000 learners. The WaSH items provided include buckets for hand washing and dispensing drinking water, liquid soap for hand washing, chlorine comparator and chlorine for cleaning surfaces alongside posters with cholera prevention messages. Additionally, UNICEF is gearing up to support more schools in Zambia’s Kapiri-Mposhi, Livingstone and Sinazongwe districts with WaSH supplies, set to be distributed before the end of 2024. These measures will ensure that Zambian learners have access to safe and clean water and standard sanitation with adequate hygiene facilities, helping create a healthier learning environment for them [23].
Water, Sanitation and Hygiene
Zambia Red Cross partnered with UNICEF in the fight against cholera in Zambia. Together, the organizations established a program of chlorinating water at the point of collection, to treat it before consumption. This initiative reached 35,000 people in Chibolya area of Lusaka district [24]. Furthermore, household WaSH kits were distributed to 180,378 households across three provinces, namely: Lusaka mainly refugee camps, 10,378 kits, 40,000 kits were distributed in Central province and the Copper belt province got up to 130,000 kits. A total of 901,890 people benefited from these WaSH packages, cumulatively the cholera control strategies have reached 3,311,658 people across the country. To sustain this momentum, UNICEF procured 57,402 new household supplies to be shared among 285,000 people in the Copper belt province. Similarly, more provisions for cholera control and prevention have been secured to be distributed to 100 cholera treatment centres and health facilities. The capacity of Commercial Water Utilities and Ministry of Health staff has been strengthened by the introduction of training courses on water quality monitoring schemes [25]. Sixteen (16) staff members in Central province were trained and are now well versed in the handling and supply of clean water.
Risk Communication
Following the Cholera Rapid Qualitative Assessments and Intra Action Review Workshop in April 2024, UNICEF developed Information, Education, and Communication (IEC) materials in four foreign languages: French, Kinyarwanda, Kirundi and Kiswahili. These materials target refugees and asylum seekers in shops across Lusaka [26]. Besides foreign languages, UNICEF has also translated cholera IEC materials into sign language to cater to the deaf community, braille for visually impaired individuals. To amplify the message, UNICEF is broadcasting multimedia messages through community radio stations in all 10 provinces of Zambia and across 15 national TV stations. These messages reach over 10 million people nationwide with emphasis on early care seeking, water safety and hand washing.
Community Involvement
UNICEF in partnership with Zambia Interfaith Networking Group (ZINGO) and Support to Order People (STOP) continues to encourage Risk Communication and Community Engagement (RCCE) activities in Lusaka. These collaborations enable community members and congregants to participate in cholera RCCE activities, promoting a collective effort to combat the infectious disease [17].
Points to Consider
The MCEP lacks full operationalization due to inadequate partner support by some key stakeholders towards the institutionalization of the strategic plan. Additionally, little to no attention given to MCEP in certain pivotal ministries because of organizational priorities. Besides, a comprehensive advocacy and resource mobilization strategy have not yet been established. However, Zambia is working on developing the plan, though the national budget has insufficient monetary allocation to MCEP. Furthermore, the country does not have enough equipment, particularly in cholera-prone area, hence the delays in laboratory confirmation of cholera by culture due to long distances to reference laboratories. The community-based surveillance structures currently in place, do not meet the demands of the target population.
The re-emergence of cholera in Zambia is a pressing public health issue that necessitates immediate attention. If left unchecked, the consequences will be extreme, putting the health and well-being of people at serious risk. To attain a cholera-free Zambia by 2025, it is vital that vaccination coverage is improved especially in high-risk areas, and monitoring systems are strengthened, with prompt laboratory surveillance and early detection of this infectious disease. Effective control relies on implementing comprehensive measures, including enhanced data collection and analysis to quickly respond to outbreaks.
Conclusion
Overall, achieving a cholera-free Zambia by 2025 is indeed a challenging goal, yet it remains an achievable reality with the right combination of resources, community involvement, and government commitment. The nation's progress so far has demonstrated that focused public health campaigns, improved sanitation, and better water quality can significantly reduce cholera cases. However, sustained efforts are essential, including consistent funding, education on hygiene practices, and quick response to outbreaks. By prioritizing these areas and fostering strong partnerships, Zambia can turn the vision of a cholera-free future into a tangible outcome, improving the health and well-being of its citizens for generations to come.
Author’s Contributions
B.S. and E.E. share equal contribution to this article. • Funding Information This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. • Conflict of Interest The authors declare that they do not have any conflicts of interest.
References
-
Chowdhury F, Ross AG, Islam MT, McMillan NAJ, Qadri F (2022) Diagnosis, management, and future control of cholera. Clin Microbiol Rev 35(3): e00211-e00221.
-
Dorsainvil M (2021) Cholera: Still a Major Public Health Issue in Sub-Saharan Africa. J Health Care Poor Underserved 32(4): 1734-1741.
-
Charnley GEC, Kelman I, Gaythorpe KAM, Murray KA (2022) Accessing sub-national cholera epidemiological datfor Nigeria and the Democratic Republic of Congo during the seventh pandemic. BMC Infect Dis 22: 288.
-
Hussen M, Worku DY, Edosa M, Kebede M, Wossen M, et al. (2024) Ethiopia National Cholera Elimination Plan 2022–2028: experiences, challenges, and the way forward. Clin Infect Dis 79: S1-S7.
-
Kateule E, Nzila O, Ngosa W, Mfume F, Shimangwala C, et al. (2024) Multisectoral approach for the control of cholera outbreak-lessons and challenges from Lusaka district-Zambia, October 2023-February 2024. Pan Afr Med J 48: 19.
-
World Health Organization International (2024) Multi- country Outbreak of Cholera.
-
Mwaba J, Debes AK, Shea P, Mukonka V, Chewe O, et al. (2020) Identification of cholera hotspots in Zambia: A spatiotemporal analysis of cholera data from 2008 to 2017. Plos Negl Trop Dis 14(4): e0008227.
-
Murebwa CR, Mwanza R, Mwinuna C, Mweene NI, Mufunda J, et al. (2017) Occurrence of cholera in Lukanga fishing camp, Kapiri-Mposhi district, Zambia. Health Press Zambia Bull 1(1).
-
Mwaba J, Debes AK, Murt KN, Shea P, Simuyandi M, et al. (2021) Three transmission events of Vibrio cholerae O1 into Lusaka, Zambia. BMC Infect Dis 21: 570.
-
Thelma CC, Chitondo L, Phiri EV, Gilbert MM (2024) Understanding and addressing the cholera outbreak in Zambian communities. International Journal of Science and Research Archive 11(1): 526-534.
-
Muyebe ASJ (2014) the Politics of Cholera Epidemics in Zambia.
-
Mbewe N, Tembo J, Kasonde M, Mwangilwa K, Zulu PM, et al. (2024) Navigating the Cholera Elimination Roadmap in Zambia-a Scoping Review (2013-2023). MedRxiv.
-
Mukonka VM, Sialubanje C, Matapo BB, Chewe O, Ngomah AM, et al. (2023) Euvichol-plus vaccine campaign coverage during the 2017/2018 cholera outbreak in Lusaka district, Zambia: a cross-sectional descriptive study. BMJ Open 13(10): e070796.
-
Mutale LS, Winstead AV, Sakubita P, Kapaya F, Nyimbili S, et al. (2020) Risk and Protective Factors for Cholera Deaths during an Urban Outbreak-Lusaka, Zambia, 2017–2018. Am J Trop Med Hyg 102(3): 534-540.
-
Maity B, Saha B, Ghosh I, Chattopadhyay J (2023) Model- Based Estimation of Expected Time to Cholera Extinction in Lusaka, Zambia. Bull Math Biol 85(7): 55.
-
Ng′ombe H, Simuyandi M, Mwaba J, Luchen CC, Alabi P, et al. (2022) Immunogenicity and waning immunity from the oral cholera vaccine (ShancholTM) in adults residing in Lukanga Swamps of Zambia. PLoS One 17(1): e0262239.
-
Olu O, Babaniyi O, Songolo P, Matapo B, Chizema E, et al. (2013) Cholera epidemiology in Zambia from 2000 to 2010: implications for improving cholera prevention and control strategies in the country. East Afr Med J 90(10): 324-331.
-
Mwape K, Kwenda G, Kalonda A, Mwaba J, Ngulube J, et al. (2020) Characterisation of Vibrio cholerae isolates from the 2009, 2010 and 2016 cholera outbreaks in Lusaka province, Zambia. Pan Afr Med J 35: 32.
-
Ko M, Cherian T, Groves HT, Klemm EJ, Qazi S (2022) Application of the Child Health and Nutrition Research Initiative (CHNRI) methodology to prioritize research to enable the implementation of Ending Cholera: A global roadmap to 2030. PLoS One 17(5): e0264952.
-
Obasohan PE, Walters SJ, Jacques R, Khatab K (2020) Risk factors associated with malnutrition among children under-five years in sub-Saharan African countries: a scoping review. Int J Environ Res Public Health 17(23): 8782.
-
Walker RI (2005) Considerations for development of whole cell bacterial vaccines to prevent diarrheal diseases in children in developing countries. Vaccine 23(26): 3369-3385.
-
Gething PW, Ayling S, Mugabi J, Muximpua OD, Kagulura SS, et al. (2023) Cholera risk in Lusaka: A geospatial analysis to inform improved water and sanitation provision. PLOS Water 2: e0000163.
-
Ladan MT, Okukpon I, Maduekwe NC (2023) Realising Sustainable Access to Water and Sanitation in Africa: Role of Critical Institutions. SDGs in Africa and the Middle East Region pp: 1-24.
-
Libanda B, Rand E, Gyang GN, Sindano CT, Simwanza L, et al. (2024) Recent and future exposure of water, sanitation, and hygiene systems to climate-related hazards in Zambia. Journal of Water and Climate Change 15: 958-977.
-
Sikder M, Deshpande A, Hegde ST, Malembaka EB, Gallandat K, et al. (2023) Water, Sanitation, and Cholera in Sub-Saharan Africa. Environ Sci Technol 57(28): 10185-10192.
-
Yasmin T, Dhesi S, Kuznetsova I, Cooper R, Krause S, et al. (2023) A system approach to water, sanitation, and hygiene resilience and sustainability in refugee communities. Int J Water Resour Dev 39(5): 691-723.
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal