Positive Affect Predicted Death Anxiety in Health Workers during the Covid-19 Pandemic
During Covid-19 pandemic, the research on health workers’ mental health grew significantly and it documented the coexistence of well-being, and trauma/negative affect, with a specific emphasis on death anxiety (DA). However, no studies focused on understanding the factors associated with death anxiety, and the protective role of well-being. The aim of this study is to examine the predictors of DA in a sample of 173 Italian health workers, assessed with indicators of psychological distress (anxiety, depression stress) and well-being (positive affect, positive mental health and post-traumatic growth). The regression model revealed that DA was predicted only by positive affect and gender. Female workers and those with lower levels of positive affect were the most vulnerable. This investigation provides new understanding on the features of DA in health workers, and it confirms the importance of maintaining and/or promoting the well-being of this population, particularly under stressful working conditions.
Introduction
The important role of positive psychology during the COVID-19 pandemic has been largely documented and reviewed in recent articles published in this Journal [1, 2]. In particular, various topics pertaining to the positive psychology research domain have been explored during the pandemic: from post- traumatic growth (PTG) to life satisfaction, hope and optimism, gratitude and resilience. The findings of these investigations all stressed out the buffering effect of these positive characteristics in dealing with lock down consequences and perceived stress due to the pandemic. Some authors documented the presence of positive emotions in the general population also during this difficult time [1, 3, 4, 5, 6]. Other investigations focused on health workers, who have been considered “heroes” across different Nations, especially during the first wave of pandemic [7, 8, 9].
On the other hand, other investigations assessed their mental health and found that these “heroes” manifested symptoms such as traumatic stress, depression, anxiety, psychological (and physical) exhaustion [9, 10]. Bassi, et al. [11] explored flourishing mental health in a group of Italian doctors and health workers during the first wave of pandemic and they found that only a small proportion of them manifested optimal well-being: those having higher levels of well-being were found to report lower post-traumatic stress symptoms.
Elgohary [10] investigated the prevalence of depression in healthcare workers during the pandemic and found that major depressive disorder was common, particularly in female workers. Moreover, in this population depression was predicted by fear of Covid-19 infection for themselves or their relatives, and fear of death with Covid-19.
In fact, during Covid-19 pandemic, the research topic of death anxiety and the fear of dying became particularly relevant in this population due to their close contact with Covid-19 positive patients. Death anxiety or fear of death has been defined as a mental condition which is activated when people feel endangered by death, or when confronted with intensive stressor, or life-threatening conditions [12]. This phenomenon was particularly reported during the first wave of pandemic when the Covid-19 vaccines were not available and face masks and other personal protective equipment were scarce. During that time health workers felt particularly vulnerable since they had to deal with an increased workload due to the massive contagion, and with an increased mortality rate among their assisted patients [13]. In line with other employees, their working performance during Covid-19 displayed different trends, considering the various challenges that the situation implied [14]. A study on female nurses documented that the risk of transmitting the infection to their household members, and the fear of death were among the factors that concerned nurses during the Covid-19 pandemic, significantly affecting their levels of depression, anxiety and stress [15].
In a study by Aguglia, et al. [16] the impact of the COVID-19 pandemic on the mental well-being of healthcare professionals was assessed, with a particular focus on the association between despair, death anxiety and post- traumatic symptoms. Based on mediation analysis, death anxiety has been identified as a possible mediator of the association between despair and post-traumatic stress symptoms. These findings support the hypothesis that healthcare workers with increasing despair may report clinically significant post-traumatic stress symptoms through increased death anxiety [16]. Similarly, Meher, at al. [12] explored death anxiety and subjective well-being in 240 Pakistani doctors during the Covid 19 pandemic and found that the association between death anxiety and subjective well-being was mediated through their sleep quality. Furthermore, death anxiety significantly and negatively predicted subjective well-being in those doctors.
Conversely, other authors Courtney EP, et al. [17, 18] explored death anxiety grounding on the perspective of the terror management theory, which posits that individuals activate specific psychological defensive mechanisms and try to construct and maintain meaning when faced with mortality awareness. Under this perspective, the pandemic of Covid -19 may have activated existential fears, that can lead either to psychological distress, or to personal growth, gratitude and existential well-being stemming from the awareness of one’s own mortality.
In order to explore the association between coronavirus anxieties, death anxiety, and individuals’ well-being in the general population, Cox, et al. [18] used structural equation modeling, and found that increased mortality concerns stemming from Covid-19 were associated with heightened benefit finding, which, in turn, was related to higher life satisfaction, meaning in life, self-esteem, resilience, and vitality.
Other authors confirmed the presence of post-traumatic growth and benefit finding during the pandemic. For example, Vazquez, et al. [19] found that beliefs about a good world, openness to the future and identification with humanity were associated with PTG; while suspiciousness, intolerance of uncertainty, anxiety about death were associated with psychological distress. In a sample of healthcare workers Kazantzakis, et al. [20] documented moderate (and interrelated) levels of post-traumatic stress symptoms and post-traumatic growth, particularly for the dimensions of life appreciation and personal strengths. Another investigation in Poland confirmed the correlation between psychological distress and PTG, which was found to be mediated by existential anxiety and subjective well-being [21].
In conclusions, all these studies confirmed the coexistence of well-being, positive psychological functioning and trauma/negative affect during the pandemic, with a specific emphasis on death anxiety/mortality awareness. However, to the best of our knowledge, no studies focused on understanding the determinants and the factors associated with death anxiety, particularly in health workers who were the most exposed to the risk of contagion.
Using a positive psychology approach, the aim of this investigation is to explore the features of death anxiety in a sample of Italian health workers, considering sociodemographic variables, negative indicators such as psychological distress (anxiety, depression, stress) and positive ones, such as positive emotions, post traumatic growth and positive mental health. Based on the aforementioned literature, we hypothesized that death anxiety in health workers might be predicted by both positive (PTG, positive affect) and negative indicators (psychological distress) with inverse and direct correlations, respectively.
Methods
Sample
This research is part of a larger, international study (Heal the Healers) that included various hospitals, clinics, nursing homes and healthcare centers across Europe. In the present research the data pertain to the Italian subsample.
Participants were recruited from several hospitals and nursing homes in Northern Italy. Researchers contacted their administrative officers/CEO, Directors. Local nurses, physicians and psychologists’ professional associations were also contacted. They received a letter with a description of the study aims, and a request for participation. After the institutions’ Ethical Board Commissions provided approval for the study and accepter their voluntarily participations, a web link with an online survey was sent and distributed among healthcare workers. Additional recruiting was conducted by consenting participants to distribute the web link to other colleagues in the healthcare settings. The online survey contained questions about sociodemographic characteristics, work conditions and information about Covid-19 infection. Healthcare workers could access the survey only after signing the informed consent form. Anonymity was preserved through assignment of an alpha numeric code. Median survey completion time was 25 mins. Data collection took place between January, 2021 and January 2022.
Assessment
Socio-demographic data collection included age, gender, marital status, and education. Work-related data were gathered on profession, job seniority, workplace, and direct contact with patients during the pandemic. Information was collected also regarding healthcare infection with Covid 19 virus (yes/no) and witnessing patients dying of Covid 19 in their workplace (yes/No).
Death anxiety was assessed with the 3-item subscale of the Illness Attitude Scale (IAS; [22]. These items are: “Are you afraid that you may die soon?”, “Does the thought of death scare you?” e “Are you afraid of news/triggers which reminds you of death?”. Participants had to answer according to a Likert scale ranging from 0 (not at all) to 4 (all the time). The total Death Anxiety score was calculated by summing up the 3 items’ single scores, with higher scores indicating higher Death anxiety. The Cronbach’ α for this sample is .781.
Positive functioning was assessed using the following questionnaires: Positive and Negative Affect Schedule [23] it measures two distinct and independent dimensions: positive affect (PA, 10 items) and negative affection (NA, 10 items) for a total of 20 items. The PA subscale reflects the degree to which a person feels enthusiastic, active and determined; the NA subscale refers to some general unpleasant states such as anger, guilt and fear. The subject has to evaluate the frequency of positive or negative emotions using a 5-point Likert scale. The Cronbach’ α for this sample is .794 for PA and .932 for NA Mental Health Continuum Short-Form [24], it consists of 14 items that measured the frequency of 3 well- being domains: 3 items for emotional well-being (EWB), 6 items for psychological well-being (PWB), and 5 items for social well-being (SWB) according to a Likert scale ranging from 0 ‘never ’ to 5 ‘everyday’. A total well-being score was calculated with a Cronbach’α value of .950 in this sample.
Post-Traumatic Growth Inventory [25]. PTGI measures the 5 dimensions of post-traumatic growth: a greater appreciation of life and a change in the sense of priorities, warmer and more intimate relationships with others, greater sense of personal strength, recognition of new possibilities or opportunities for one’s life, and spiritual development. The short version consists of 10 items and participants had to answer with a 6-level Likert scale, according to their degree of agreement with the content of the item. A total PTGI score was calculated by summing up each item’s score. The Cronbach’ α is .959 in this sample.
Psychological Distress was Assessed Using the Following Questionnaire: Depression Anxiety Stress Scales Short Version (DASS-21; [26] it consists of 21 items (7 items per subscale: depression, anxiety and stress). Participants were asked to score every item on a Likert scale from 0 (did not apply to me at all) to 3 (applied to me very much). Sum scores were computed by adding up the scores on the items per (sub)scale and multiplying them by a factor 2. Sum scores for the total DASS-total scale thus range between 0 and 120, and those for each of the subscales may range between 0 and 42. The Chronbach’α of the DASS-21 (total score) is .947 in this sample.
Statistical Analyses
Bivariate correlations and Descriptive statistics were used to describe the final sample of Italian Health workers (mean / frequencies). Skewness and kurtosis values were calculated and indicated that the data satisfied the normality assumption for all the measures used.
In order to evaluate the psychosocial correlates, of death anxiety a multivariate linear regression analysis (method enter) was performed. A three-step model was used, where socio demographic factors (age, gender, direct contact with patients during the pandemic (yes/no), infection with Covid 19 virus (yes/no) (step 1); indicators of psychological distress (DASS total score and PANAS Negative affect scale) (step 2); indicators of positive functioning (MHC total score, PTGI scale and PANAS Positive affect scale) (step 3) were entered to test if they significantly predicted death anxiety total score.
The partial eta-squared as a measure of effect size was calculated considering a value of 0.1 as a large effect, a value of 0.04 as a medium effect and a value of 0.01 as a small effect [27]. The significance level was set at p < .05. Analyses were performed with the Statistical Package for the Social Sciences (SPSS), version 28.
Results
A total of 173 HW completed the survey. After data cleaning 5 participants were excluded due to missing data (one or more questionnaires not answered). The final dataset included 168 responders: n=137 Female (81.5%); n=31 Males (18.5%). Their mean age was 43.68 years (SD=10.741; age range: 22-71 years).
Based on the Italian classification system of health professions, participants were physicians, nurses and midwives, nurses working in aging facilities, psychologists, social workers, professionals in technical (e.g., technicians in radiology, biomedical lab) and rehabilitation areas (e.g., physiotherapists), and healthcare assistants. They were divided into two categories based on their workplace: the category “frontline workers” included HW working directly in contact with hospitalized patients, or in nursing facilities, or with outpatients, but with a physical contact with them. 117 individuals (69.6%) belonged to this category: 94 were female (80.3%) and their mean age was 42.9 years (SD=11.56).
The category “second line workers” comprised HW working in healthcare facilities, but without a direct/in person daily contact with patients (technicians in radiology, biomedical lab, administrative staff, ect..). 51 individuals (30.4%) belonged to this category: 43 were female (84.3%) and their meal age was 45.48 years (SD= 8.37).
Table 1 illustrates the bivariate correlations between DA and the other selected variables. The only non-significant correlation is with the PTGI scale, which is significantly and directly correlated only to MHC.
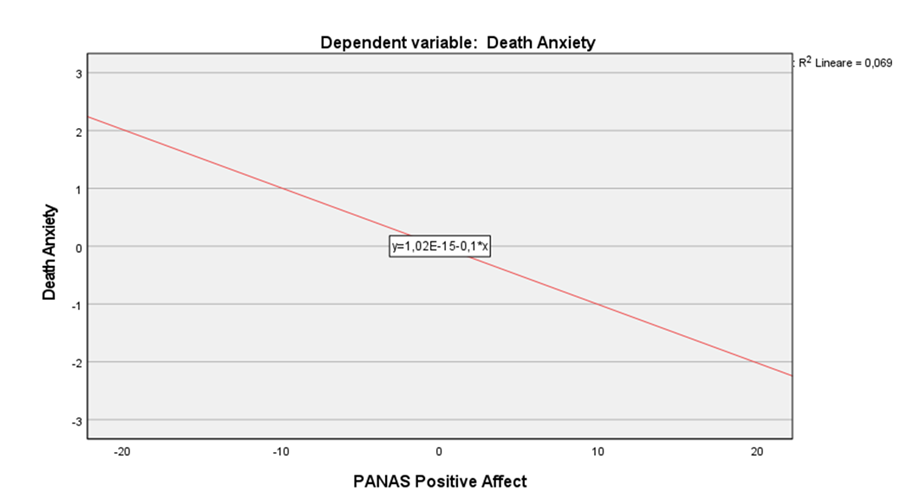
A three-step regression model was calculated to predict death anxiety (dependent variable). It revealed that variables included in the third model explained 87% of the variance (F 9,150 = 4,88, p < .001). Particularly, female gender and positive affect predicted death anxiety scores (β = 0.164, p < .05, β = −0.318, p < .001, respectively) (Table 2 & Figure 1).
| DA | PANAS NA | DASS | PANAS PA | MHC | PTGI | |
|---|---|---|---|---|---|---|
| DA | 1 | ,266** | ,306** | -,374** | -,252** | ,059 |
| PANAS NA | ,266** | 1 | ,738** | -,307** | -,400** | -,038 |
| DASS | ,306** | ,738** | 1 | -,416** | -,447** | -,056 |
| PANAS PA | -,374** | -,307** | -,416** | 1 | ,616** | ,129 |
| MHC | -,252** | -,400** | -,447** | ,616** | 1 | ,315** |
| PTGI | ,059 | -,038 | -,056 | ,129 | ,315** | 1 |
Table 1: Correlation matrix among variables in the sample of health workers (n=168).
PANAS -NA= PANAS Negative Affect Scale; PANAS -PA= PANAS Positive Affect Scale; MHC=Mental health Continuum; PTGI= Posttraumatic Growth Inventory DA= Death Anxiety **p<0.001. Table 1: Correlation matrix among variables in the sample of health workers (n=168).
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| β | p | β | p | β | p | |
| Age | -0.1 | 0 | -0 | 0.671 | -0.03 | 0.693 |
| Gender (0=M; 1=F) | 0.19 | 0 | 0.18 | 0.02 | 0.16 | 0.031 |
| Frontline workers | -0 | 1 | -0 | 0.593 | -0.08 | 0.284 |
| Covid-19 infection | 0.09 | 0 | 0.12 | 0.126 | 0.08 | 0.28 |
| PANAS- NA | 0.11 | 0.329 | 0.1 | 0.355 | ||
| DASS total score | 0.2 | 0.075 | 0.07 | 0.566 | ||
| PANAS -PA | -0.3 | 0.001 | ||||
| MHC | -0.03 | 0.773 | ||||
| PTGI | 0.04 | 0.674 | ||||
| R2 | 0.06 | 0.14 | 0.23 | |||
| R2 change | 0.06 | 0.08 | 0.09 | |||
| F value | 2.34 | 0 | 4.14 | <0.001 | 4.88 | <0.001 |
Table 2: Regression models predicting death anxiety in the total sample of health workers (N = 168).
PANAS -NA= PANAS Negative Affect Scale; DASS = Depression Anxiety Stress Scale; PANAS -PA= PANAS Positive Affect Scale; MHC=Mental health Continuum; PTGI= Posttraumatic Growth Inventory. Table 2: Regression models predicting death anxiety in the total sample of health workers (N = 168).
Discussion
The main aim of this investigation was to explore death anxiety and its associations with other indicators of psychological distress and positive functioning in sample of health workers. As previous research already has documented [28, 29, 30], death anxiety was associated with psychological distress, and inversely correlated to indicators of positive functioning also in our sample. The only notable exception is post-traumatic growth (PTG), which was not associated with death anxiety in our sample. This data disconfirms Cox, et al. [8] who documented that increased mortality concerns stemming from COVID-19 were associated with heightened benefit finding (a dimension similar to PTG), which, in turn, was related to other dimensions of positivity (i.e., life satisfaction, meaning in life, self-esteem). However, these findings refer to a general population, not to health professionals. In health professionals mortality awareness might be experienced more frequently and more commonly, also before the pandemic [29, 31]. Thus, as a consequence, it might not yield the “shattering of basic assumption in life” nature, as a necessary condition for PTG to appear, according to the model of PTGI [32]. This observation might provide an explanation to the lack of correlation between death anxiety and PTGI in our sample. However, also in the present research, PTG was associated to other indicators of well- being (i.e., MHC) (see correlation matrix).
Furthermore, the regression model found that death anxiety was not predicted by negative affect, or psychological distress, but by positive affect and -to a minor extent-by female gender. Gender differences in death anxiety have been largely documented by previous literature [33, 34] where females consistently reported higher scores than men. The gender influence on death anxiety was found to be mediated by other variables, such as emotional expressiveness, self-disclosure, social desirability [34], mastery, self-efficacy [35, 36] and (more recently) also by disgust [37]. Unfortunately, this body of research is still inconclusive in providing a definitive explanation for the differences between male and females in death anxiety. A prospective study documented that this gender difference appears particularly relevant in early adulthood (around 20ies) and later in midlife, when women around 50 year of age manifested a peak in death anxiety scores [38]. Considering that the mean age of our sample was 44 years and it was composed in prevalence by women, our findings might provide confirmation to Russac, et al. [38] work.
The novelty of our research, however, is that the most significant predictor of death anxiety was PA, and surprisingly, not NA, or psychological distress (measured with DASS) as other investigations have previously documented [39, 40, 41]. However, this data confirms the significant relationship between death anxiety and subjective well-being in health professionals [12]. Similarly, Meher, at al. [12] found an association between death anxiety and subjective well-being in health professionals during the Covid 19 pandemic, but it was mediated by their sleep quality (that was a direct source of doctors’ well-being) and by working in rural (vs urban) settings. Unfortunately, we did not assess these variables in our sample. Furthermore, death anxiety significantly and negatively predicted subjective well-being in Meher, et al. [12] article. Conversely, we were aimed at exploring the predictors of death anxiety, rather than health workers’ well- being and we have documented a robust, inverse association between positive affect and death anxiety. Surprisingly, our regression model did not find significant relationships with Covid-19 infection, nor frontline work, or with other indicators of positive functioning, either PTG or positive mental health (MHC scores). These findings, thus, are not in line with previous literature on health workers’ well-being during the pandemic [11, 12, 18, 29, 39]. Outside the specific peculiarities of this population, the association between positive affect, well-being and death anxiety have been scarcely investigated and future research is needed.
In any case, these findings highlight the buffering effect of positive emotions in dealing with stress, as already established by the broaden and built theory of positive emotions, and subsequent research data [4, 42, 43]. Also under an extremely stressful and risky working condition as the pandemic, health workers were less likely to worry about their own death if their reported to have experienced positive emotions. These emotions might have mitigated their levels of anxiety, or might have activated specific psychobiological correlates (i.e., the CTRA response) Cole SW, et al. [44, 45] not evaluated in the present investigation. Future research is needed, but the inverse correlations found in our regression model can be considered an indicator of the protective role of positive emotions for health workers’ death anxiety.
Strengths and Limitations
This study is limited by its preliminary nature, the self- selected, homogenous sample, and the use of self-reports as assessment methodology. This fact leaves the possibility of self-report bias to inflate some of the significant correlations and it limits the external validity of the findings. Furthermore, we have not used a specific scale for assessing Covid-19 anxiety or a specific questionnaire for death anxiety [33, 35], since they were not available in the Italian version at the time of the investigation.
Despite these limitations, this is also the first investigation during the Covid-19 pandemic that was specifically focused on health workers’ death anxiety and its correlates in terms of distress and positive functioning.
Conclusions
The pandemic has revealed the crucial role of health professionals in communities and societies around the world. Even if they have been considered “heroes” [7, 8], health workers manifested vulnerabilities as well, and, among them, the fear of being infected with Covid-19 virus and to die was the most recurrent one. Our investigation provides new understanding of its features in a sample of Italian health workers. Female workers and those with lower levels of positive affect were the most vulnerable in terms of death anxiety. Most importantly, this investigation provides confirmation to the importance of maintaining and/or promoting the well-being of this population, particularly during health crises or under stressful working conditions. For example, in previous research meditation was found to activate spirituality and a sense of self-transcendence that, in turn, were found to mitigate death anxiety [46, 47, 48, 49]. Also, meditation practices were found to activate the parasympathetic nervous system, which is directly connected to a pleasurable physical state [50, 51]. If future research would replicate the findings of this study, meditation or other positive interventions focused on the promotion of positive emotions [52] may become essential tools to foster health workers’ well-being and, consequently, to guarantee healthier communities.
Conflict of Interest
The authors have no conflict of interest to declare
Funding
This work was supported by the European Commission Erasmus+, Key Activity 3: FRIENDS - Project n° 592247-EPP- 1-2017-1-IT-EPPKA3-IPI-SOC-IN; and by the Maharishi
Foundation, Italy under a Grant for the project “Heal the Healers” to Prof. Chiara Ruini.
References
-
Allemand M, Olaru G, Hill PL (2021) Gratitude and future time perspective during the COVID-19 pandemic: Effects of age and virus worry. The Journal of Positive Psychology 17(6): 1-13.
-
Waters L, Cameron K, Nelson-Coffey SK, Crone DL, Kern ML, et al. (2021) Collective wellbeing and posttraumatic growth during COVID-19: How positive psychology can help families, schools, workplaces and marginalized communities. The Journal of Positive Psychology 17(6): 1-29.
-
Waters L, Algoe SB, Dutton J, Emmons R, Fredrickson BL, et al. (2022) Positive psychology in a pandemic: Buffering, bolstering, and building mental health. The Journal of Positive Psychology 17(3): 303-323.
-
Brouzos A, Vassilopoulos SP, Romosiou V, Stavrou V, Tassi C, et al.(2021). ‘Stay Safe-Feel Positive’ on the frontline: An online positive psychology intervention for police officers during the COVID-19 pandemic. The Journal of Positive Psychology pp: 1-11.
-
Hill PL, Klaiber P, Burrow AL, DeLongis A, Sin NL (2022) Great, purposeful expectations: Predicting daily purposefulness during the COVID-19 response. The Journal of Positive Psychology 17(1): 89-101.
-
Prinzing MM, Zhou J, West TN, Le Nguyen KD, Wells JL, et al. (2022) Staying ‘in sync’ with others during COVID-19: Perceived positivity resonance mediates cross-sectional and longitudinal links between trait resilience and mental health. The Journal of Positive Psychology 17(3): 440-455.
-
Brennan J (2020) Heroes in healthcare; what’s wrong with that. International Journal for Quality in Health Care 32(9): 567-568.
-
Cox CL (2020) ‘Healthcare Heroes’: Problems with media focus on heroism from healthcare workers during the COVID-19 pandemic. Journal of Medical Ethics 46(8): 510-513.
-
Mascayano F, Van der Ven E, Moro MF, Schilling S, Alarcón S, et al. (2022). The impact of the COVID-19 pandemic on the mental health of healthcare workers: Study protocol for the COVID-19 HEalth caRe wOrkErS (HEROES) study. Social Psychiatry and Psychiatric Epidemiology 57(3): 633-645.
-
Elgohary HM, Sehlo MG, Bassiony MM, Youssef UM, Elrafey DS, et al. (2021) Depression among health workers caring for patients with COVID-19 in Egypt. The Egyptian Journal of Neurology, Psychiatry and Neurosurgery 57(1): 139.
-
Bassi M, Negri L, Delle Fave A, Accardi R (2021) The relationship between post-traumatic stress and positive mental health symptoms among health workers during COVID-19 pandemic in Lombardy, Italy. Journal of Affective Disorders 280: 1-6.
-
Meher K, Mushtaq M, Fatima S (2022) Death Anxiety and WellBeing in Doctors During COVID-19: The Explanatory and Boosting Roles of Sleep Quality and Work Locality. OMEGA - Journal of Death and Dying.
-
Walton M, Murray E, Christian MD (2020) Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. European Heart Journal: Acute Cardiovascular Care 9(3): 241-247.
-
Sarfraz M (2023) Editorial Opinion: Employees’ Work Performance and Organization Success during COVID-19. Psychol Psychology Res Int J 8(2): 1-2.
-
Işık O, Tengilimoğlu D, Tosun N, Zekioğlu A, Tengilimoğlu O (2022) Evaluating the Factors (Stress, Anxiety and Depression) Affecting the Mental Health Condition of Nurses During the COVID-19 Pandemic. Evaluation and the Health Professions 45(1): 86-96.
-
Aguglia A, Amerio A, Costanza A, Parodi N, Copello F, Serafini G, Amore M (2021) Hopelessness and post- traumatic stress symptoms among healthcare workers during the covid-19 pandemic: Any role for mediating variables? International Journal of Environmental Research and Public Health 18(12).
-
Courtney EP, Goldenberg JL, Boyd P (2020) The contagion of mortality: A terror management health model for pandemics. British Journal of Social Psychology 59(3): 607-617.
-
Cox CR, Swets JA, Gully B, Xiao J, Yraguen M (2021) Death Concerns, Benefit-Finding, and Well-Being During the COVID-19 Pandemic. Frontiers in Psychology 12.
-
Vazquez C, Valiente C, García FE, Contreras A, Peinado V, et al. (2021) Post-Traumatic Growth and Stress-Related Responses During the COVID-19 Pandemic in a National Representative Sample: The Role of Positive Core Beliefs About the World and Others. Journal of Happiness Studies 22(7): 2915-2935.
-
Kalaitzaki A, Tamiolaki A, Tsouvelas G (2022) From secondary traumatic stress to vicarious posttraumatic growth amid COVID-19 lockdown in Greece: The role of health care workers’ coping strategies. Psychological Trauma: Theory, Research, Practice, and Policy 14(2): 273-280.
-
Tomaszek K, Muchacka-Cymerman A (2020) Thinking about My Existence during COVID-19, I Feel Anxiety and Awe-The Mediating Role of Existential Anxiety and Life Satisfaction on the Relationship between PTSD Symptoms and Post-Traumatic Growth. International Journal of Environmental Research and Public Health 17(19): 7062.
-
Kellner R, Abbott P, Winslow WW, Pathak D (1987) Fears, Beliefs, and Attitudes in DSM-III Hypochondriasis: The Journal of Nervous and Mental Disease 175(1): 20-25.
-
Watson D, Clark LA, Tellegen A (1988) Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of personality and social psychology 54(6): 1063-1070.
-
Keyes CLM (2002) The mental health continuum: From languishing to flourishing in life. Journal of health and social behavior 43(2): 207-222.
-
Tedeschi RG, Calhoun LG (1996) The Posttraumatic Growth Inventory: Measuring the positive legacy of trauma. J Trauma Stress 9(3): 455-471.
-
Lovibond SH, Lovibond PF (1995) Manual for the depression anxiety stress scales. Lovibond SH, Lovibond PF (Eds.), In: Manual for the depression anxiety stress scales 2nd (Edn.), Psychology Foundation of Australia.
-
Huberty CJ (2002) A History of Effect Size Indices. Educational and Psychological Measurement 62(2): 227-240.
-
Arpaci I, Karatas K, Baloglu M, Haktanir A (2022) COVID-19 Phobia in the United States: Validation of the COVID-19 Phobia Scale (C19P-SE). Death Studies 46(3): 553-559.
-
Asadi N, Esmaeilpour H, Salmani F, Salmani M (2021) The Relationship Between Death Anxiety and Alexithymia in Emergency Medical Technicians. OMEGA - Journal of Death and Dying 8(3).
-
Cozzolino PJ (2006) Death contemplation, growth, and defense: Converging evidence of dual-existential systems? Psychological Inquiry 17(4): 278-287.
-
Bianco S, Testoni I, Palmieri A, Solomon S, Hart J (2019) The Psychological Correlates of Decreased Death Anxiety After a Near-Death Experience: The Role of Self-Esteem, Mindfulness, and Death Representations. Journal of Humanistic Psychology pp: 002216781989210.
-
Tedeschi RG, Calhoun LG (1998) Posttraumatic Growth: Conceptual Issues. In: Calhoun LG, Tedeschi RG (Eds.), Positive Changes in the Aftermath of Crisis. Lawrence Erlbaum Associates, Inc. Publishers pp: 1-22.
-
Andrade EF, Pereira LJ, de Oliveira APL, Orlando DR, Alves DAG, et al. (2022) Perceived fear of COVID-19 infection according to sex, age and occupational risk using the Brazilian version of the Fear of COVID-19 Scale. Death Studies 46(3): 533-542.
-
Dattel AR, Neimeyer RA (1990) Sex differences in death anxiety: Testing the emotional expressiveness hypothesis. Death Studies 14(1): 1-11.
-
Caycho-Rodríguez T, Vilca LW, Cervigni M, Gallegos M, Martino P, et al. (2022) Fear of COVID-19 scale: Validity, reliability and factorial invariance in Argentina’s general population. Death Studies 46(3): 543-552.
-
Eshbaugh E, Henninger W (2013) Potential Mediators of the Relationship Between Gender and Death Anxiety. Individual Differences Research 11(1): 22-30.
-
Bassett JF (2017) Disgust Sensitivity Accounts for Some But Not All Gender Differences in Death Attitudes. OMEGA-Journal of Death and Dying 75(1): 26-46.
-
Russac RJ, Gatliff C, Reece M, Spottswood D (2007) Death Anxiety across the Adult Years: An Examination of Age and Gender Effects. Death Studies 31(6): 549-561.
-
Pradhan M, Chettri A, Maheshwari S (2022) Fear of death in the shadow of COVID-19: The mediating role of perceived stress in the relationship between neuroticism and death anxiety. Death Studies 46(5): 1106-1110.
-
Yıldırım M, Arslan G, Alkahtani AM (2022) Do fear of COVID-19 and religious coping predict depression, anxiety, and stress among the Arab population during health crisis?. Death Studies 46(9): 2070-2076.
-
Zahedi Bidgol Z, Tagharrobi Z, Sooki Z, Sharifi K (2020) Death Anxiety and Its Predictors Among Older Adults. Journal of Holistic Nursing and Midwifery pp: 101-110.
-
Fredrickson BL (2001) The role of positive emotions in positive psychology. The American psychologist 56(3): 218-226.
-
Galanakis M, Galanopoulou F, Stalikas A (2011) Do positive emotions help us cope with occupational stress. Europe’s Journal of Psychology 7(2): 221-240.
-
Cole SW, Levine ME, Arevalo JMG, Ma J, Weir DR, et al. (2015) Loneliness, eudaimonia, and the human conserved transcriptional response to adversity. Psychoneuroendocrinology 62: 11-17.
-
Fredrickson BL, Grewen KM, Algoe SB, Firestine AM, Arevalo JMG, et al. (2015) Psychological Well-Being and the Human Conserved Transcriptional Response to Adversity. PloS One 10(3): e0121839.
-
Bach JM, Guse T (2015) The effect of contemplation and meditation on ‘great compassion’ on the psychological well-being of adolescents. Journal of Positive Psychology 10(4): 359-369.
-
Koszycki D, Raab K, Aldosary F, Bradwejn J (2010) A multifaith spiritually based intervention for generalized anxiety disorder: A pilot randomized trial. Journal of Clinical Psychology 66(4): 430-441.
-
Park O, Lee YK, Younglee, Smith Stoner M (2016) The Effect of Insight Based Death Meditation on Death Anxiety and Qualify of Life. International Journal of Existential Psychology and Psychotherapy 6(1): 1-10.
-
Vaillant GE (2013) Psychiatry, religion, positive emotions and spirituality. Asian Journal of Psychiatry 6(6): 590- 594.
-
Hwang K, Kwon A, Hong C (2017) A Preliminary Study of New Positive Psychology Interventions: Neurofeedback- Aided Meditation Therapy and Modified Positive Psychotherapy. Current Psychology 36(3): 683-695.
-
Rickard NS, Vella Brodrick DA (2014) Changes in Well- Being: Complementing a Psychosocial Approach with Neurobiological Insights. Social Indicators Research 117: 437-457.
-
Van Agteren J, Iasiello M, Lo L, Bartholomaeus J, Kopsaftis Z, et al. (2021) A systematic review and meta-analysis of psychological interventions to improve mental wellbeing. Nature Human Behaviour 5(5): 631-652.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis