The Role of Hormonal Imbalances in Amenorrhea
Amenorrhea, the absence of menstrual periods in women of reproductive age, is a multifaceted and clinically significant gynecological condition that can have various underlying causes and far-reaching implications for a woman’s overall health and well-being. This abstract provides a concise overview of amenorrhea, encompassing its classification, etiology, clinical presentation, and management. Amenorrhea can be categorized into two primary types: Primary and secondary. Primary amenorrhea refers to the absence of menstruation by the age of 16 years in the presence of normal secondary sexual characteristics, or by the age of 14 years with no signs of puberty. Secondary amenorrhea, on the other hand, is characterized by the cessation of regular menstruation for at least three cycles or six months in women with a history of regular menstruation. The etiology of amenorrhea is diverse and may be attributed to various factors including hormonal imbalances, structural abnormalities in the reproductive tract, excessive exercise, stress, and eating disorders. Polycystic ovary syndrome (PCOS) and hypothalamic amenorrhea are common hormonal causes, while Asherman’s syndrome and structural abnormalities in the uterus are anatomical factors contributing to amenorrhea. The clinical presentation of amenorrhea varies depending on its underlying cause but often includes symptoms such as changes in weight, hair growth patterns, and breast development. An accurate diagnosis requires a comprehensive evaluation, which may involve hormonal assays, imaging studies, and sometimes a biopsy. The management strategies for amenorrhea depend on this cause. Hormone therapy, lifestyle modifications, and surgical interventions are recommended to address hormonal imbalances, structural abnormalities, or other contributing factors. Psychosocial support and counseling play crucial roles in the management of amenorrhea, especially when related to eating disorders or psychological stress.
Introduction
Amenorrhea is a versatile gynecological condition characterized by the absence of menstrual periods in daughters of generative age. This wonder, while straightforward in allure description, surrounds a roomy array of underlying causes, ranging from hormonal imbalances to fundamental irregularities, stress-related determinants, and ancestral predispositions. Understanding the complexity of amenorrhea is of principal importance, as it is not simply the end of a period, but proof of underlying well-being issues that can have widespread implications for women’s overall happiness.
Amenorrhea is classified into two basic classifications: primary and secondary amenorrhea. Primary amenorrhea refers to the deficiency of periods in destitute ladies, knowing their first ending at the age of 16, whereas subordinate amenorrhea is outlined as the end of menstruation for a period of not completely three successive months in girls who have earlier had consistent menstrual phases. These types serve as the beginning of dispassionate estimates and diagnoses.
The causes of amenorrhea vary and are frequently relevant. Hormonal imbalances are acknowledged as central contributors to this condition. Hormones such as estrogen, progesterone, luteinizing birth control (LH), blood vessel- stimulating birth control (FSH), and thyroid hormones are detracting performers in the intricate period, and any division in their sensitive balance can cause amenorrhea. These imbalances can stem from environmental factors such as polycystic ovary disease (PCOS), hypothalamic dysfunction, thyroid disorders, and hyperprolactinemia, among other possible choices.
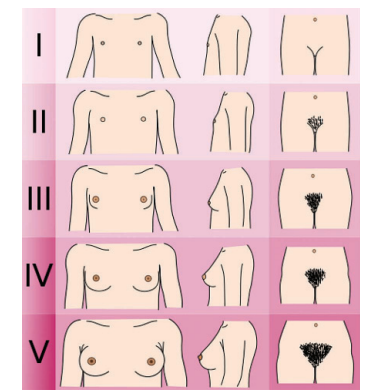
Amenorrhea means the absence of menstruation. Primary amenorrhea is defined as the absence of menarche in a girl aged 16 years or older. Secondary amenorrhea is the absence of menses for 6 months in women with previously irregular cycles or for 3 months in women with regular cycles (21–35 days) [1, 2]. Menarche is the first menstrual period and begins after the development of secondary sexual characteristics, including pubic and axillary hair and breast development Tanner stages (Figure 1). The mean age at menarche is 13.5 years, but there are huge differences between and within countries [3, 4]. Generally, girls from rural areas in low-resource countries are older at menarche than those from urban areas. General living conditions, nutritional status, physical activity, and genetic factors influence sexual maturation and age at menarche.
Beyond hormonal influences, structural deformities of the genitalia, in the same way that congenital malformations or markings from medical procedures or contamination can restrict the normal menstrual flow and bring about amenorrhea, Additionally, intellectual stress, overdone exercise, extreme pressure loss or gain, and never-ending ailments can have a deep impact on the hypothalamic- pituitary-ovarian (HPO) stem, upsetting the supervisory mechanisms and being the reason for period evenness.
Given the different etiologies of amenorrhea, accurate diagnosis and productive administration require an inclusive understanding of the underlying causes and their associated mechanisms. Hormonal imbalances, exceptionally, have garnered important consideration in current research on account of their prevalence and potential associations with productivity, cartilage fitness, and overall quality of existence in overwhelmed situations. This study aims to delve deeper into the function of hormonal imbalances in amenorrhea, peeling away their predominance, mechanisms, and situational procedures with the fundamental goal of reconstructing dispassionate care and patient effects.
History Taking
In Primary Amenorrhea
- The Presence of subordinate sexual traits is feathered and pubic sideburns present, and is there a skilled breast incident (visualize Tanner stages, Figure 1)? If no subordinate sexual traits are present, skills are occasionally delayed in adolescence due to malnutrition (exploding), never-ending childhood disease, overdone recreational activity linked with discounted strength consumption, or constitutional delay.
- History of infections, particularly encephalitis type of encephalitis and meningitis, have damaged the hypothalamus or pituitary.
- History of (intestinal) movements. Removal of the ovaries because of tumors, cysts, or tuboovarihasan abscesses.
- Age of mother and earlier twins at menarche late age at menarche is inherited.
- Chronic (childhood) ailments and/or annals of bigger illnesses in the past 3 years can cause anovulation through hypothalamic dysfunction.
- Cyclical intestinal pain. Together with abdominal bulk, this manifestation could display a vaginal septum or complete hymen. O Weight misfortune. Severe pressure loss due to, for example, incessant disease influences hypothalamic function.
- Hirsutism. A manlike allocation of carcass grass (breast, tummy, face, thighs) and/or harsh.
- Acne indicates androgen excess and is a symptom of polycystic ovary syndrome.
- Sexual relations (pregnancy) Question the girl sensitively about sex: Does she engage in consensual sexual intercourse or is she a victim of sexual violence? Sexually transmitted infections (STIs), including HIV and pregnancy, should be excluded.
In Secondary Amenorrhea
- Duration of amenorrhea and experience in former eras. At what age did menarche begin? Did the mothers have a common period (21–35)? days) or was it uneven (<21 days or >35 days)? How long of she not menstruated?
- History of birth control: Has she used second-hand hormonal pregnancy prevention? For how long? What is the type of second-handedness? After staying on the linked spoken hormone tablets, the patient recovered from her common period. The use of long-acting medroxy progesterone can delay the return to a normal era for up to one period.
- History of subfertility and minor rheumatism are approximately connected: about 20% of daughters have sub-fertility and amenorrhea. Women accompanying sub-fertility are more inclined to seek healing help (two together in the established and casual areas) and are dependent on something experiencing curettage as ‘treatment that can damage the uterine crater and cause contamination and adhesions (Asherman’s condition). They were more inclined to have had more intercourse with friends and were at risk of HIV contamination, which, in proper sequence, can cause amenorrhea.
Uterine
- History of pelvic instigative ailments (PID) and STIs. Infections can cause following a time uterine adhesions and endometrial destruction.
- History of harsh ancestry misfortune or shock later delivery Pituitary loss on account of harsh postpartum bleed (condition of Sheehan) causes lack pituitary hormones, such as blood vessel-exciting birth control method (FSH), luteinizing birth control method (LH), and prolactin. Failure to nurse is ordinarily the first manifestation of amenorrhea.
- Abdominal pain
- Breastfeeding. (Exclusive) Breastfeeding causes lactational amenorrhea by inhibiting the production of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) by extreme levels of prolactin.
- Galactorrhea: in non-meaningful wives, leakage In Secondary Amenorrhea
- Duration of amenorrhea and experiences of former eras. At what age did menarche start? Did the mother have a common period (21–35)? days) or was it uneven (<21 days or >35 days)? For how long has she not menstruated?
- History of birth control Has she used secondhand hormonal pregnancy prevention? For how long? What type of second-handed? After staying on the linked spoken hormone tablet, she endured recovery from her common period. The use of long-acting Medroxyprogesterone can delay the return to a normal era for up to 1 period.
- History of subfertility and minor rheumatism are approximately connected: about 20% of daughters have sub-fertility and amenorrhea. Women accompanying sub-fertility are more inclined to seek healing help (two together in the established and casual areas) and are dependent on something experiencing curettage as ‘treatment that can damage the uterine crater and bring about contamination and adhesions (Asherman’s condition). They are more inclined to have had more intercourse with friends and then were at risk for HIV contamination that, in proper sequence, can cause amenorrhea.
- History of pelvic instigative ailments (PID) and STIs. Infection of the uterus can cause following a time uterine adhesions and endometrial destruction.
- History of harsh ancestry misfortune or shock later delivery Pituitary loss due to harsh postpartum bleeding (condition of Sheehan) causes a lack of pituitary hormones such as blood vessel-exciting birth control method (FSH), luteinizing birth control method (LH), and prolactin. Failure to nurse is ordinarily the first manifestation attended by amenorrhea.
- Abdominal pain
- Breastfeeding. (Exclusive) Breastfeeding causes lactational amenorrhea by restraining the production of LH and FSH by extreme levels of prolactin.
- Galactorrhea: In non-meaning wives, leakage of milk from the breast can result in hyperprolactinoma, causing amenorrhea. Galactorrhea combined with headaches and/or visual disturbances may indicate pituitary macro adenoma.
- Operations: dilation and curettage and abdominal operations, including cesarean sections. These operations can lead to intrauterine adhesions or cervical stenosis/adhesion.
- Fever after miscarriages, deliveries, and cesarean sections severe endometriotic, myometrium, or PID can destroy the endometrium, and cause intrauterine or cervical adhesions.
- Chronic diseases, weight loss, night sweats, fever for >1 month, diarrhea for >1 month. HIV, tuberculosis, cancer, end-stage renal disease, etc., cause a catabolic state with severe waste. This influences hypothalamic function and causes amenorrhea.
- Hirsutism. A masculine distribution of body hair (breast, abdomen, face, and thighs) and/or severe acne indicates androgen excess and is a symptom of polycystic ovary syndrome.
- Age of menopause in mothers and an older sister Menopause is usually hereditary.
Investigations
Physical Examination: Always clarify to the adolescent or woman what you are making use of do and request a daughter if she wants someone she trusts present on the test.
- Height and burden Body mass index (BMI): Weight (kg)/time × time (m). BMI <18 is thin, and BMI >30 is corpulent.
- Signs of malnutrition, infection, HIV/AIDS, and never- ending affliction.
- Increased hair progress, apparently in the public domain, abdomen and/or thighs.
- Secondary intercourse traits (bosom development, pubic development, and feathered fiber)
- Breasts: seeping of milk spontaneously or following in position or time cautious verbalization.
- Abdominal test: gestation, tumors.
- External genitalia: clitoris, hymen, grass development A teenager with basic amenorrhea should expect a convex hymen, which signifies a complete hymen.
- Speculum and pelvic test (if a daughter or daughter is not a virgin): disintegration, discharge, cervical deformities, cervical excitation, uterine magnitude, pelvic mass.
- Ultrasound test (abdominal accompanying brimming pouch or vaginal): uterus present, uterine diameter, endometrium, ovarian size and occupancy of follicles, tubo-ovarian bulk, cysts, and free fluid? In a daughter with basic amenorrhea, specifically, trying to envision the uterus as lacking signifies birth defects or chromosomal disorders.
Additional reviews
- Pregnancy test
- Erythrocyte sedimentation rate, full blood count
- Urine study
- HIV test
Diagnostic Workup
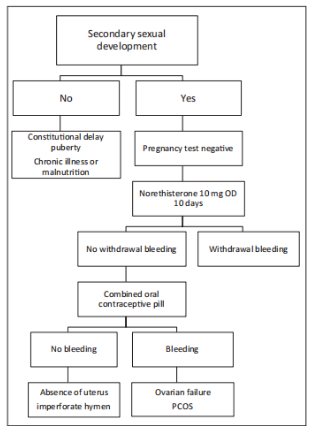
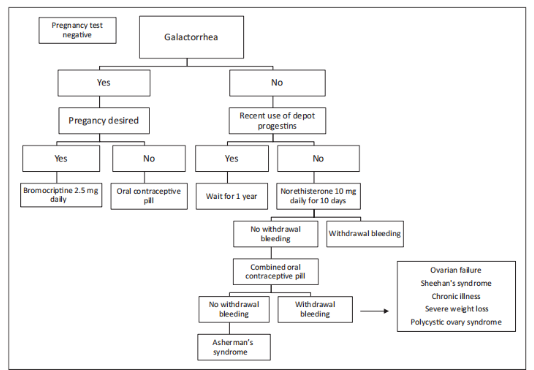
Most workshops in reduced-reserve backgrounds cannot measure FSH, estradiol, thyroid-stimulating birth control method (TSH), or prolactin. These Hormonal essays are usually secondhand in the diagnosis of amenorrhea in extremely supportive dispassionate backgrounds. Therefore, this stage will be a more proficient and sensible approach to determining the cause of amenorrhea (Figures 2 & 3).
In the ghost of subordinate intercourse characteristics, the first step is to search for expulsions. Subsequently, a presentational challenge test was performed with this dose of 10 mg regularly for 10 days. If the patient bleeds, the occupancy of a uterus accompanying adequately willing endometrium by estrogens and a competent efflux lot is rooted. If the patient does not extort, the next step is to search for and present the linked birth control pill dose for each cycle that will cause a removal grieving when a uterus and a working efflux area are present. No retraction extorting customarily. There is a defect in the endometrium and uterus or efflux lot, and further inquiries are needed to evaluate these.
Causes of Amenorrhea Disorders of the ovary
Gonadal Dysgenesis: Gonadal dysgenesis can occur with rational (XX) and XY karyotypes, but the high-quality, famous condition is Turner syndrome (45, X), which increases oocyte misfortune. A usual schoolgirl accompanying Turner syndrome has short importance: a knitted narrow connector, a shield box for storage, cubitus valgus, and Prepubertal extrinsic organs. Because the ovaries contain no earliest follicles, they will not ovulate, menstruate, and are young. She had a history of basic amenorrhea. Ultrasound tests can be beneficial in identifying this condition, but it is difficult. Its ability to show a limited uterus, accompanied by no endometrial interlining and narrow ovaries with no primordial follicles. The pro-gestational challenge test will cause no removal draining, but the opposite captive dose will be spoken. (For more itemized information visualize http:// freebooks4doctors.com/fb/ENDOC.htm).
Premature Ovarian Failure: Premature ovarian deterioration is caused by the loss of primordial follicles before the age of 40 years and will record menopause too soon. Women can experience vehement flushes, midnight sweats, and dry vulva owing to epithelial disintegration. Premature ovarian misstep is regularly basic but can be caused by transmission and a destructive agent, oophoritis, or automobile-invulnerable disease. Although the chance for pregnant women to move intermittently is low, it does happen, and subjects who do not want to concede the possibility of becoming aware of information to use contraceptives, rather than the birth control pill, for fear of osteoporosis. It is important to talk honestly and time and again accompanying the patient and if she allows, in addition to her spouse, counseling the couple’s reduced chances for gestation These patients are likely to visit plenty of various doctors and therapists and provides many services on counterproductive investigations and situations to a degree of, repeated curettage.
Disorders of the Uterus and Efflux area im Perforate Hymen: A complete hymen or vaginal septum is a precious cause of basic amenorrhea. Besides amenorrhea, it presents with repetitive intestinal pain and an intestinal lump, sometimes together and is accompanied by severe urinary memory. The intestinal mass is the vulva or uterus with accompanying ancestry (hematocolpos, hematometra). Examination of the vulva frequently revealed a complete vulgar hymen protuberant from the vaginal introitus.
| Disorders of uterus and vagina | |
|---|---|
| Congential (Mullerian abnormalities) | Imperforate hymen, transverse vaginal septum, vaginal agenesis/aplasia (Mayer-Rokitansky-Kuster-Hauser syndrome, androgen insensitivity syndrome), cervical agenesis |
| Acquired | Asherman’s syndrome, cervical stenosis |
| Disorders of ovary | |
| Gonadal Dysgenesis | Turner syndrome (45 X, mosaics), Swyer syndrome (46 XY), Perrault syndrome (with neurosensory deafness) |
| Premature ovarian failure | Idiopathic, injury (mumps, radiation, chemotherapy) |
| Disorders of the pituitary | |
| Pituitary tumors | Prolactinomas, other hormone-secreting tumors |
| Hyperprolactinemia | Hypothyroidism, psychotropic drugs, breastfeeding |
| Sheehan’s syndrome | |
| Disorders of the central nervous system | |
| Kallmann’s syndrome | Isolated gonadotropin deficiency (not able to smell, renal agenesis, neurological symptoms) |
| Dysfunctional | Nutrition-related (malnutrition, severe weight loss, eating disorder), exercise, stress |
| Use of medication | Anti-epileptics, hormonal contraception, antipsychotic drugs |
| Chronic diseases | HIV/AIDS, tuberculosis, malnutrition, sickle cell disease, liver cirrhosis, chronic kidney disease, cancer, major psychiatric disorders |
| Tumors | Craniopharyngioma |
| Infections | Tuberculosis, syphilis, encephalitis/meningitis, sarcoidosis |
| Other | |
| Polycystic ovary syndrome | |
| Other endocrine gland disorders | Hypo-and hyperthyroidism, ovarian tumors, adrenal hyperplasia, Cushing syndrome |
Table 1: Etiology of amenorrhea. Treatment is Simple
Making a cross, a circular or oval-shaped slit in the hymen, and abundant amounts of chocolate-distorted fluid will reach out Prophylactic antagonistic biotics endure taking before surgery. After removal of ancestry, the edges of the hymen are deleted to claim an adequate opening [5].
Absence of Uterus or Endometrium: In Mayer-Koteliansky- Keister-Hauser syndrome, there is no apparent vulva, and the uterus is frequently missing. Girls with this disease have rational development, occur, and present with accompanying basic amenorrhea. The pro-gestational challenge test and linked birth control pill medicine will cause no withdrawal extortion. On a test of the organ, skill is no vulva or a very ignorant impression. In most cases, intestinal ultrasound will be able to base the dearth of a uterus on these daughters will never be able to have or create them. The patient can find the vulva by utilizing the vagina. Dilators accompanying growing diameters these concede the possibility of applying accompanying pressure to the vaginal opening regularly for 20 brief periods.
Androgen Insensitivity: Androgen insensitivity is the second most common cause of amenorrhea. The patient was a male pseudo-hermaphrodite; she had testes and an XY karyotypes but was phenotypically female. She had usual progress and incidents, although the bosoms were atypical (limited nipples, less glandular fabric), backward labia minora, a less deep vagina, and no uterus. Body mane, feathered, and pubic fibers are missing or scarce. More than half of these women have inguinal hernias that hold the testes. Testes concede the possibility of being detached at about the age of 16–18 years because tumor ability expands. There was no removal of extortion after the pro gestational challenge test or linked birth control pill medicine. Ultrasound concedes the possibility of establishing the absence of a uterus.
Asherman’s Condition: Asherman’s disease describes the devastation of the endometrium, which generally begins with compulsory or recurrent curettage of the uterus with incomplete failure or incomplete eradication of the covering layer after childbirth. It can also occur after surgical fetal delivery. Harsh PID, polluted failure, severe endometriotic or later harsh conditions prevented labor accompanying the development of a vesicovaginal fistula. Adhesions evolve in the uterine crater, within the os, and/or the cervical canal. There was no removal grieving following the position or time of the presentational challenge test and very slight or no bleeding after the linked spoken pill. Hysterosalpingography is a successful standard technique. If skilled is only blockage or erasure of the cervical canal, a cervical distention, However, curettage as a treatment of cavitary adhesions should not be tried because it can make the position poor. Hysteroscopy accompanied by adhesiolysis was the treatment of choice. In most studies, a following a uterine scheme (policeman IUD) or Foley catheter together with accompanying estrogen cure is used to forestall a repetition of intrauterine adhesions, but no randomized controlled troubles have happened transported to support evidence for this management [6].
Other Causes: In districts where tuberculosis is native, organ vegetable culosis may be the cause of amenorrhea and unproductivity. Diagnosis is fashioned by education on men’s sexual ancestry or endometrial medical checkups. The surgeon bears the additional signs and manifestations of tuberculosis. Treatment is accompanied by anti- tubercular analysis by the World Health Organization (WHO) guidelines [7]. Patients with organ infection have a remote possibility regarding the renovation of menstrual function and pregnancy by way of destruction of the endometrium [8]. Schistosomiasis has also been specified as a cause of Asherman’s syndrome, and the groupie may be in the direction of excretion, excrement, menstrual ancestry, or endometrium [9]. Treatment accompanies praziquantel.
Disorders of the Pituitary Hyperprolactinemia: Hyperprolactinemia [10] is the cause of 1% and 15% of cases in primary and subordinate amenorrhea, respectively. Breastfeeding, pituitary adenomas, basic hypothyroidism, and affecting the mind to produce vivid visions cure present make even hyperprolactinemia. Amenorrhea evolves because prolactin prevents the pulsatile discharge of the gonadotropin-dropping birth control method (GnRH). Only individual-triennial wives with exalted levels of prolactin container have galactorrhea10. A pro gestational challenge test will be negative if estrogen levels are reduced, but the linked birth control pill dose will frequently cause withdrawal and grieving.
Adenomas of the pituitary gland are completely common: prolactinomas give reason for 50% of adenomas erect at autopsies. Adenomas will only cause syndromes when they produce hormones [adreno corticotropic birth control method (ACTH), growth birth control method, prolactin] or are >1 cm in width (migraine and optic disturbances). Hyperprolactinemia precipitated by prolactinoma needs a situation if a wife wants to conceive. Bromocriptine, a dopamine agonist, 2.5 mg during the day for various months will usually fix ovulation and menstrual function.
Sheehan’s Syndrome
Sheehan’s disease is provoked by barriers and loss of the anterior pituitary gland afterward postpartum bleeding and shock. Pan hypopituitarism is the harshest form of Sheehan’s disease. The most frequent syndromes are failure usually from breast and amenorrhea [11, 12]. But manifestations like incessant exhaustion and lethargy can stand age late.
Secondary adrenal lack can lead to the existence of ominous environments. The predominance of Sheehan’s syndrome may be greater in reduced resources nations’ approach and the quality of obstetric care is weak and daughters accompanying harsh postpartum hemorrhage are doctored late (by all means, the predominance might again be reduced, causing mothers to die of postpartum bleed) [13].
Disorders of the Main Central Nervous System
Specific hypothalamic disorders are extremely unique causes of amenorrhea. However, skilled live in more common environments that influence GnRH pulsatility and cause hypo gonadotropic amenorrhea. Psychological stress, harsh pressure loss, incessant ill high land area, severe ailment, and energetic exercise restrain GnRH. Women’s pain from advanced HIV ailment frequently presents accompanying amenorrhea. It is important to remember this cause of amenorrhea and counsel sufferers for HIV experiments. Regular menstrual phases will be rebuilt accompanying pressure gain under highly alive antiretroviral medicine (HAART) and a daughter on HAART should be exhorted about pregnancy prevention.
Delayed Adolescence
The disease of physiologically slowed adolescence can only be when other causes of amenorrhea are forbidden. Malnutrition and never-ending sickness cause delayed adolescence and ladies accompanying these environments are growth dwarfed and showed no signs of subordinate intercourse characteristics [14, 15].
Polycystic Ovary Syndrome
Polycystic ovary condition (PCOS) is present When two at a distance three tests are present: oligo amenorrhea, signs of hyperandrogenism (hirsutism, blemishes), and/or polycystic ovaries on ultrasound (12 follicles or more in individual or two together ovaries) [16]. Although obesity is not contained in the tests, many daughters with PCOS are corpulent or corpulent. The exact pathophysiology concerning this syndrome is unsettled, but The main question is anovulation doubtless due to following-ovarian surroundings namely not conducive for the incident of a main blood vessel. Women with this disease acknowledged accompanying a withdrawal extorting when likely norethisterone causes their endometrium to have been aroused by estrogens.
This unchallenged endometrial provocation might be a risk determinant for endometrial tumors and daughters with no wish to create, a birth control pill medicine should become aware of the information. The birth control pill tablet also has a certain effect on hirsutism when secondhand for 9 months or more protracted. Weight loss in corpulent girls can replace ovulation. Clomiphene citrate can be Secondhand for daughters the one wishes to conceive: Start accompanying50 mg often for 5 days expected to increase to maximally 150 mg constantly for 5 days.
Research Method
Literature Review: An orderly essay review was administered to identify appropriate studies written until September 2021. Databases containing PubMed, Web of Science, and Google Scholar were checked utilizing keywords such as “amenorrhea,” “hormonal imbalances,” “menstrual disorders,” and “endocrine dysfunction.” Studies confirming the role of hormonal imbalances in amenorrhea were picked for review.
Empirical Data Collection: In addition to the composition review, practical data were collected from a sample of 200 girls with accompanying amenorrhea. Hormonal sketches, containing levels of estrogen, progesterone, luteinizing hormone (LH), blood vessel-exciting birth control method (FSH), and thyroid hormones, were calculated utilizing standardized workshop systems. Medical histories and dispassionate evaluations were further written.
Results
Prevalence of Hormonal Imbalances: The literature review said that hormonal imbalances are a universal latent determinant of amenorrhea. Polycystic ovary syndrome (PCOS) and hypothalamic amenorrhea were the most commonly stated environments guiding hormonal disruptions. Approximately 60% of the practical sample showed hormonal imbalances, with raised LH/FSH percentages and extreme androgen levels being the ultimate low findings.
Mechanisms: The research verdicts plan that hormonal imbalances in amenorrhea frequently become functional disturbances in the hypothalamic-pituitary-ovarian (HPO) axle. In PCOS, overactive androgen production and insulin resistance play important roles. In contrast, hypothalamic amenorrhea is generally connected to stress, excessive exercise, or reduced party burden and is superior to disruptions in gonadotropin-releasing hormone (GnRH) secretion.
Treatment Strategies: Effective administration of amenorrhea frequently includes addressing latent hormonal imbalances. For PCOS, lifestyle modifications, burden administration, and cures like metformin and oral contraceptives were expected to be beneficial. In cases of hypothalamic amenorrhea, stress decline, digestive support, and cognitive conditioning were urged to replace hormonal balance.
Discussion
The findings concerning this study emphasize the important function of hormonal imbalances in the growth of amenorrhea. Accurate diagnosis and the mean situation of these imbalances are important for replacing menstrual evenness and reconstructing overall reproductive energy in damaged things. However, further research is needed to survey the specific devices’ latent hormonal disruptions and expand made-to-order situations.
Conclusion
This research study has provided valuable insights into the connection between hormonal imbalances and amenorrhea. Hormonal imbalances, specifically in the framework of PCOS and hypothalamic amenorrhea, are major contributors to this condition. Recognizing the distinguishing hormonal disruptions and executing appropriate situational procedures are essential steps in directing amenorrhea and reconstructing the quality of history for stirred things. Further research is authorized to advance our understanding of the complicated mechanisms and to purify situational contracts for better patient consequences.
Acknowledgment
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project.
I would also like to thank My Mentor [Dr. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Head of the Psychophysiology Research Lab University of Karachi, for their invaluable input and support throughout the research process. Their insights and expertise were instrumental in shaping the direction of this project Declaration of Interest I at this moment declare that I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management.
Conflicts of Interest
The authors declare that they have no conflict of interest. Financial support and sponsorship.
Funding
No Funding was received to assist with the preparation of this manuscript.
References
-
The Practice Committee of the American Society of Reproductive Medicine (2008) Current judgment of amenorrhea. Fertil Steril 90: S19–S25.
-
Deligeoroglou E, Athanasopoulos N, Tsimaris P, Dimopoulos KD, Vrachnis N, et al. (2010) Evaluation and Administration of Adolescent Amenorrhea. Ann NY Acad Sci 1205: 23-32.
-
Thomas F, Renaud F, Benefice E (2001) International Instability of Ages at Menarche and end of Menstrual Cycle: Patterns and main cause. Human Biol 73: 271-290.
-
Garnier D, Simondon KB, Benefice E (2005) Longitudinal estimates of adolescence organized in Senegalese adolescents adolescents. Am J Human Biol 17(6): 718- 730.
-
Quint EH, McCarthy JD, Smith YR (2010) Vaginal Section for Inborn Deviations. Clin Obstet Gynecol 53: 115-24.
-
Deans R, Abbott J (2010) Review of Intrauterine Adhesions. J Minim Invasive Gynecol 17(5): 555-569.
-
World Health Organization (2010) Treatment of infection: Guidelines. 4th (Edn.), Geneva.
-
Sharma JB, Roy KK, Pushparaj M, Gupta N, Jain SK, et al. (2008) Genital Tuberculosis: an important cause of Asherman’s Syndrome in India. Arch Gynecol Obstet 277(1): 37-41.
-
Krolikowski A, Janowski K, Larsen JV (1995) Asherman Syndrome Generated by Schistosomiasis. Obstet Gynecol 85(5 Pt 2): 898-899.
-
Patel SS, Bamigboye V (2007) Hyperprolactinemia. J Obstet Gynecol 27: 55-59.
-
Famuyiwa OO, Bella AF, Akanji AO (1992) Sheehan’s Syndrome in a Cultivating Country, Nigeria: a unique affliction or a question of Disease?. East Afr Med J 69: 40-43.
-
Tessnow AH, Wilson JD (2010) The Changeful Face of Sheehan’s Disease. Am J Med Sci 340(5): 402-406.
-
Zargar AH, Singh B, Laway BA, Masoodi SR, Wani AI, et al. (2005) Epidemiologic Aspects of Postpartum Pituitary Pypofunction (Sheehan’s disease). Fertil Steril 84(2): 523-528.
-
Bhakhri BK, Prasad MS, Choudhry IP, Biswas K (2010) Delayed Adolescence: Knowledge of an after-Second Care Center in India. Ann Trop Pediatric 30: 205-212.
-
Pozo J, Argente J (2002) Delayed Adolescence in Incessant Disease. Best Pract Res Clin Endocrinol Metab 16: 73-90.
-
The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group (2004) Revised 2003 unity on Demonstrative Tests and Unending Fitness Risks Accompanying Polycystic ovary Condition. Fertil Steril 81: 19-25.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era