An In-Vitro Cone-Beam Computed Tomographic Evaluation of Root Canal Anatomy of Permanent Mandibular Incisor Teeth in an Indian Population
The current study aimed to investigate the root canal anatomy and possible variations in permanent mandibular incisor teeth (central and lateral) of an Indian subpopulation, using three-dimensional cone-beam computed tomography (CBCT) imaging in vitro. Material and Methods: A total of 200 freshly extracted permanent mandibular incisors (100 central incisors and 100 lateral incisors) were collected from dental hospitals and private clinics in Mumbai and Navi Mumbai cities from the state of Maharashtra. Teeth with fully formed apices, no calcifications, no previous endodontic treatment, absence of root fracture, absence of internal/external resorption were included in the study. The collected samples were exposed to CBCT scanning and the root canal anatomy with variations (if any) was tabulated according to Vertucci’s classification for each sample. Results: Of the 200 teeth analyzed the most common root canal configuration was Type I (55.5%), followed by Type III (24.14%), Type II (12.08%), and Type IV (3%). Also, of the 111 Type I canals, 60.37% (67 off 111) presented round, while 39.63% (44 of 111) presented non-round canals in the coronal and the middle thirds. At the apical third of the canals 81.08% (90 of 111) exhibited round, whereas 18.91% (21 of 111) exhibited non-round cross-section.</p> <p>Conclusion: With high prevalence of presence of a multiple canals in single rooted mandibular incisor for the studied population, the operator should be extremely cautious while carrying out the root canal treatment of these teeth.
Introduction
The main goal of an endodontic treatment is the correct diagnosis, optimal mechanical instrumentation and chemical disinfection, followed by three-dimensional fluid tight seal of the entire root canal system [1]. Failure of treatment is not uncommon despite rigid adherence to all basic treatment protocols. One of the major reasons for this is inability of the operator to identify the root canal anatomy and locate the extra canals if any [2]. The mandibular permanent incisors are succedenous teeth located adjacent to the midline in the lower arch. Known to be the smallest adult human teeth; they are also flat and narrow in the labio-lingual dimension. They are almost always single rooted but the internal root canal anatomy is prone to exhibit complex variations. As these teeth are usually radiographed only in one plane, they appear single canaled and more accessible than they really are. Adding to the difficulty while treating these teeth, the narrow crown offers restricted area of access to the root canals. There are various studies reported in literature on root canal anatomies of these teeth in different populations with rare exploration in Indian population [1, 3]. A number of destructive and non-destructive methodologies have been described in the literature including decalcification, radiography, vertical and cross- sectional cutting, histological evaluation, stereomicroscopy analysis, surgical microscopy, plastic casts, scanning electronic microscopy, cone beam computed tomography (CBCT) and micro-computed tomography (mCT) [4, 5, 6]. Traditional radiography although commonly used, portrays a 2-dimentional image of a 3-dimentional structure, which results in compression of vital anatomical information about the root canal anatomy [6]. Besides this most of the time the conventional antero-posterior radiographs does not reveal the mesio-distal anatomy of the tooth. For this reason CBCT has been evaluated as an accurate diagnostic tool to define the number of root canals in vitro [7, 8]. As the root canal anatomy of permanent mandibular incisor teeth of an Indian population has not been explored extensively, this study was devised to evaluate the number of root canals, and the possible variations seen in the root canal morphologies in the permanent mandibular incisors of an Indian population.
Materials and Methods
Sample Selection
A total of 200 freshly extracted permanent mandibular incisors (central incisors and lateral incisors) were collected from dental colleges and clinics in the city of Mumbai. The teeth were washed with water and stored in saline with thymol solution until the sample collection was complete. Each tooth extracted was accompanied by case history record defining the ethnicity of the patient. The inclusion criteria were; permanent mandibular central and lateral incisors, fully developed single or multiple roots, and teeth extracted of patients with an Indian origin by birth. Teeth with fracture, broken during extraction, endodontic treatment/intervention, root caries, calcification, and resorption (internal/external) were excluded from the current study. Following completion of collection of samples, they were cleaned of calculus and soft tissue debris using an ultrasonic scaler (Woodpecker Dte-D5, China) at a power setting of 03 with continuous water spray.
CBCT Acquisition
The 200 samples (n=100 central incisors, and n=100 lateral incisors) were mounted on to wax for CBCT scanning. CBCT images were obtained using ProMax 3D Mid (Planmeca OY, Helsinki, Finland). The scans were obtained at the following parameters: 90kV and 8mA with isotropic resolution set at 0.1mm, with 8.9 seconds scanning time and slice thickness of 0.1mm. The scans obtained were analyzed cross-sectionally, and longitudinally and the canals were visualized using Romexis version 2.9 (Planmeca OY, Helsinki, Finland) and classified keeping Vertucci’s classification as reference [7].
- Root Canal Configuration
- Results
- The occurrence of the different canal configurations for the 200 permanent mandibular incisors (100 central and
- 100 lateral) is presented in (Table 1).
- Number of Roots
- All the samples evaluated (100 central incisors, and
- 100 lateral incisors) exhibited single roots.
- Root canal types according to Vertucci’s classification
- Central Incisor (n=100)
- Lateral Incisor (n=100)
- Type I
- 57
- 54
- Type II
- 12
- 15
- Type III
- 24
- 27
- Type IV
- 4
- 2
- Type V
- -
- -
- Type VI
- -
- -
- Type VII
- -
- -
- Type VIII
- -
- -
- Others
- 3
- 2
Table 1: Classification of root canal systems according to Vertucci as seen and evaluated in 200 permanent mandibular
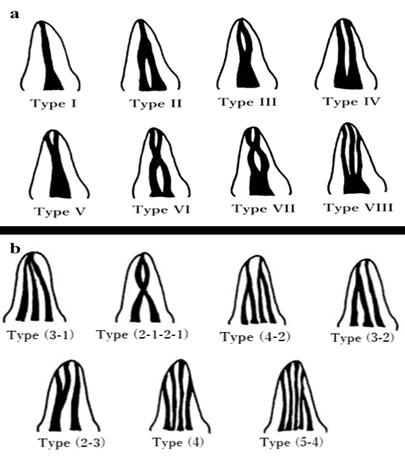
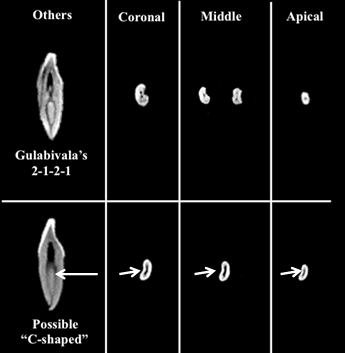
Figure 3: Representative image of other root canal variations seen in permanent mandibular central and lateral incisors evaluated in current study according to Gulabivala’s classification and possibly a “C-shaped” as the longitudinal section resembles 2 canals and the cross- section images at coronal, middle and apical third resemble a c shaped with a developmental groove as seen with teeth exhibiting this root canal anatomy (white arrows).
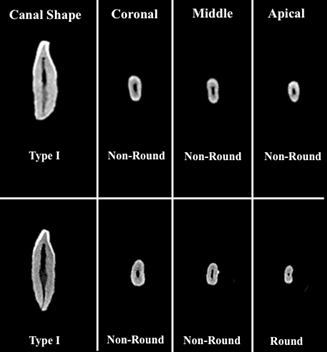
Prevalence of Canal Shape in Single Canaled Samples
Of the 111 single canaled permanent mandibular incisors, 60.37% (67 off 111) exhibited round and 39.63% (44 of 111) exhibited a non-round canal cross-section in coronal and the middle thirds (Figure 4). For the apical third, 81.08% (90 of 111) were associated with round and 18.91% (21 of 111) with non-round cross-section.
Discussion
It is assumed that mandibular incisors are associated with a single root and a single canal. However literature shows that complicated configurations are present, and that canal configurations vary with respect to ethnicity and race [9, 10]. A number of techniques are used to study the internal anatomy of the teeth, most conventional being radiographic and clearing & staining and radiography [11]. Although clinically conventional periapical radiographs present as a valuable diagnostic tool, they cannot be relied on completely because of inherent limitations like; distortion and superimposition of bony and dental structures [11]. Although the canal staining and clearing technique is considered the gold standard method of studying root canal anatomy, it has a number of demerits like the tooth morphology can get distorted in the clearing process as the tooth structures are weakened during demineralization process [12, 13]. The weakened tooth thereafter could be distorted during the dying process of the specimen and, small structures like accessory canals or isthmuses could be distorted or missed. Another problem with this technique is limited dye penetration. Root canal blockage resulting from narrowing and calcification below the grain size of dye solution hinders the infiltration of the dye solution [12, 13]. The use of cone beam computed tomography (CBCT) has proved to serve as a boon in endodontics. CBCT scans are able to differentiate between many types of structures and airspaces including bone, teeth, airway, paranasal sinuses, and sometimes soft tissue while avoiding diagnostic limitations inherent in 2-D images like superimposition of structures, non uniform magnification, distortion and no depth information. Patel et al., have reported CBCT to be as precise as the conventional techniques of clearing and staining in the determination of root canal anatomy [14, 15]. The high accuracy, comparatively less exposure time and radiation dose added to the ability to have a 3 dimensional reconstruction and visualization have made CBCT the investigation of choice in modern dentistry [16, 3]. In the current study, the root canal anatomy of mandibular incisor teeth was evaluated using three- dimensional cone beam computed tomography in vitro. Every specimen was analyzed in multiple sections and all three dimensions to accurately assess the internal anatomy of the root canal systems. Of the samples evaluated, 57% of mandibular central insisors and 54% of mandibular lateral incisors presented with a single canal. Of the 100 mandibular central incisors, 12% showed type II, 24% showed type III and 4% showed type IV canal system according to Vertucci’s classification. However, 46% of permanent mandibular lateral incisors showed the presence of multiple canals of which 15% showed Type II, 27% showed Type III and 2% showed Type IV canal system (according to Vertucci’s classification). The results of the current investigation show that almost half (43% central and 46% lateral) of the specimen collected from an Indian population showed a second canal with the bifurcation most commonly being in the middle third of the root. The failure to identify this complex anatomy due to lack of anatomic knowledge or lack of skill to negotiate these canal systems account for majority of endodontic failures of mandibular incisors [17, 18]. These results were in accordance to the results of the study conducted by Sikri and Sikri that showed the presence of single canal (Vertucci’s Type I) in 58.33% permanent mandibular central incisors and 59.78% of mandibular lateral incisors. Vertucci’s Type II canal anatomy was seen in 12.5% mandibular central incisors, Type III in 4.16% and Type IV in 4.16%. While 4.3% mandibular lateral incisors showed Vertucci’s Type II, 3.26% showed Type III and 6.52% showed Type IV canal configurations [1]. Boruah and Bhuvan showed that in the mandibular incisors of North Eastern Indian population, possess a slightly higher percentage (63.75%) of Type I canal system. One third of the teeth (36%) exhibited two canal system and of the teeth with two canals, Type III configuration was most common followed by Type II and Type V [3]. Jaju, Sushma P.; Jaju, Prashant P.; Garcha, Vikram conducted A retrospective study of 130 Indian patients who underwent a CBCT scan for implants and assessed variation in the root canal anatomy in the mandibular incisors [19]. They found that Vertucci type I and type III configurations were more prevalent in both mandibular central and lateral incisors [19]. 81.37% of teeth had a single canal and 28.43% of teeth had two canals, Type 1 Vertucci configuration was found to be the most prevalent one, and type 4 the least prevalent in the study conducted by Kamtane & Ghodke on the mandibular incisors of Indian sub population of Pune [20]. The study conducted by Benjamin and Dawson in 1974 also showed similar statistics of root canal systems in permanent mandibular central incisors [21]. However, for the Chinese population Type I root canal morphology is more common according to the studies by You-nong & Bao-li and Qing-ping & Xing [22, 10]. The frequency of multiple canals was 5.0% for central incisors and 14.7% for lateral incisors in the study conducted by Yang ZhengyanluKeke Wang Fei li Yueheng Zhou Zhi in the permanent mandibular anterior teeth in Chinese population [23]. All of these studies reported a much higher prevalence of a single canal in the specimen. These differences in findings can be attributed to the different methods of conducting the studies and more to the anatomic differences in the teeth of people of different geographic regions and ethnicities. A comparison of the current study to the previous reported studies on the root canal morphology of mandibular anterior teeth in various populations is presented in Table 2.
Number
No Investigato
Teeth studied
rs Year Region
of samples Benjamin &
Mandibular
1 Dawson
1974 Unknown 364
central incisor (21) Mandibular
2 Kartal&Yani
koglu (9) 1992 Turkish 100
central incisor Mandibular
96 central incisors Radiogra
3 Sikri&Sikri
(2) 1994 Indian
Mandibular
92 lateral incisors Mandibular
You- nong&Bao-li
1995 Chinese 108
central incisors
4 (22) Canal classification according to Vertucci’s
types (%) Nature of
Study
I II III IV V VI VIIVIII OTHE
MULTI-
RS
ROOT
Radiogra
phy (In-
58.640.1 0 1.3 0 0 0 0 0 41.4
vitro) Staining & clearing 55 16 20 4 3 0 0 0 2 45
107 Mandibular 71.00.09 18.6 0 5.61 0 0 0 8.41 28.97
lateral incisors Mandibular
5 Caliskan et
al (26) 1995 Turkish 100
lateral incisors Mandibular
6 Miyashita et
al (4) 1997 Japanese 85
central incisors Mandibular
200 central incisors Staining & clearing
7 Sert et al
(27) 2004 Turkish
Mandibular
201 lateral incisors Mandibular
100 central incisors Staining & clearing
8 Vertucci (7) 2005 American
Mandibular
100 lateral incisors Al- Qudah&Aw awdeh (28)
Mandibular
Staining & clearing 87.6 9.3 0 1.4 1.7 0 0 0 0 12.4
Staining & clearing 73.810.9 6.7 5.1 3.6 0 0 0 0 26.2
Radiogra
| 18 | Kamtane&G hodke (20) | 2015 | Indian | 52 | Mandibular central incisors | CBCT(In- vivo) | 64.7 1 | 23.53 | 8.82 | 2.9 4 | 0 | 0 | 0 | 0 | 0 | 0 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 50 | Mandibular lateral incisors | |||||||||||||||
| 19 | Dhaimade et al | Curren t Study | Indian | 100 | Mandibular central incisors | CBCT (In- vitro) | 57 | 12 | 24 | 4 | 0 | 0 | 0 | 0 | 3 | 0 |
| 100 | Mandibular lateral incisors | 54 | 15 | 27 | 2 | 0 | 0 | 0 | 0 | 2 | 0 |
Table 2: Percentage of root canal anatomies of permanent mandibular incisor teeth of various populations using different methods
Table 2: Percentage of root canal anatomies of permanent mandibular incisor teeth of various populations using different methods of evaluation by numerous authors compared to the current study. Clinical methods like dental operating microscope, loops, and dyes can be used to identify the 2nd canal. Optimizing the access preparation by extending the traditional lingual access toward the cingulum overcomes the challenge of locating the second canal in mandibular incisors. Exposing a labial or incisal approach has also become more acceptable with the advent of highly aesthetic restorative materials in dentistry [21, 25, 26].
Conclusion
A comprehensive understanding about the normal root canal anatomy and all possible variations is necessary for the success of any endodontic procedure. Almost, 50% of permanent mandibular incisors (Central and Lateral) in the studied Indian population showed the presence of more than one canal. The clinicians should give due consideration to such population based studies, make more efforts, use 3D radiography whenever possible and indicated, modify the traditional access cavity extending it towards the cingulumetc to reduce the changes of missing the extra canal and prevent subsequent failure of the root canal treatment. Although some studies have been conducted on the root canal anatomy of mandibular incisors, further research is always helpful to better understand root-canal anatomy, thus increasing the success rate of endodontic treatment.
References
-
Sikri VK, Sikri P (1994) Root canal morphology of mandibular incisors. Endod 6: 9-13.
-
Estrela C, Bueno MR, Couto GS, Rabelo LE, Alencar AH, et al. (2015) Study of Root Canal Anatomy in Human Permanent Teeth in A Subpopulation of Brazil's Center Region Using Cone-Beam Computed Tomography-Part 1. Braz Dent J 26(5): 530-536.
-
Boruah LC, Bhuyan AC (2011) Morphologic characteristics of root canal of mandibular incisors in North-East Indian population: An in vitro study. J Conserv Dent 14(4): 346-350.
-
Miyashita M, Kasahara E, Yasuda E, Yamamoto A, Sekizawa T (1997) Root canal system of the mandibular incisor. J Endod 23(8): 479-484.
-
Matherne RP, Angelopoulos C, Kulild JC, Tira D (2008) Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod 34(1): 87-89.
-
Mukhaimer R, Jarbawi M (2013) Radiographic study of the root canal system of mandibular incisors in Palestinian population. Open J Stomatol 15: 452-456.
-
Vertucci FJ (1984) Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 58(5): 589-599.
-
Aminsobhani M, Sadegh M, Meraji N, Razmi H, Kharazifard MJ (2013) Evaluation of the root and canal morphology of mandibular permanent anterior teeth in an Iranian population by cone-beam computed tomography. J Dent 10(4): 358-366.
-
Kartal N, Yanıkoğlu FÇ (1992) Root canal morphology of mandibular incisors. J Endod 18(11): 562-564.
-
Qing-ping Z, Xing C (212) The relationship between the number of root canal & age in mandibular anterior teeth. Poster presented at: The 7th Annual Meeting of Chinese Geriatric Dentistry: Beijing, People’s Republic of China, pp: 53-54.
-
Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG (2007) Endodontic applications of cone-beam volumetric tomography. J Endod 33(9): 1121-1132.
-
Weng XL, Yu SB, Zhao SL, Wang HG, Mu T, et al. (2009) Root canal morphology of permanent maxillary teeth in the Han nationality in Chinese Guanzhong area: a new modified root canal staining technique. J Endod 35(5): 651-656.
-
Chang SW, Lee JK, Lee Y, Kum KY (2013) In-depth morphological study of mesiobuccal root canal systems in maxillary first molars: review. Restor Dent Endod 38(1): 2-10.
-
Patel S, Dawood A, Ford TP, Whaites E (2007) The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J 40(10): 818-830.
-
Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA (1998) A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol 8(9): 1558-1564.
-
Patel S, Horner K (2009) The use of cone beam computed tomography in endodontics. Int Endod J 42(9): 755-756.
-
Janik JM (1984) Access cavity preparation. Dental Clinics of North America 28: 809-818.
-
Logani A, Singh A, Singla M, Shah N (2009) Labial access opening in mandibular anterior teeth: An alternative approach to success. Quintessence Int 40(7): 597-602.
-
Jaju SP, Jaju PP, Garcha V (2003) Root canal assessment of mandibular incisors in an Indian population using cone beam CT. Endodontic Practice Today 7(2): 105-111.
-
Kamtane S, Ghodke M (2016) Morphology of Mandibular Incisors: A Study on CBCT. Pol J Radiol. 81: 15-16.
-
Benjamin KA, Dowson J (1974) Incidence of two root canals in human mandibular incisor teeth. Oral Surg Oral Med Oral Pathol 38(1): 122-126.
-
You-nong W, Bao-li Y (1995) Morphology research of 1976 permanent root canal. J Pract Stomatol 11: 98- 101.
-
Zhengyan Y, Keke L, Fei W, Yueheng L, Zhi Z (2016) Cone-beam computed tomography study of the root and canal morphology of mandibular permanent anterior teeth in a Chongqing population. Ther Clin Risk Manag 12: 19-25.
-
Ingle J, Bakland L (2002) Endodontics. 5th Edition, BC Decker, Hamilton.
-
Clements RE, Gilboe DB (1991) Labial endodontic access opening for mandibular incisors: Endodontic and restorative considerations. J Can Dent Assoc 57(7): 587-589.
-
Calişkan MK, Pehlivan Y, Sepetçioğlu F, Türkün M, Tuncer SS (1995) Root canal morphology of human permanent teeth in a Turkish population. J Endod 21(4): 200-204.
-
Sert S, Aslanalp V, Tanalp J (2004) Investigation of the root canal configurations of mandibular permanent teeth in the Turkish population. Int Endod J 37(7): 494-499.
-
Al-Qudah AA, Awawdeh LA (2006) Root canal morphology of mandibular incisors in a Jordanian population. Int Endod J 39(11): 873-877.
-
Shu-fen S, Lin-xia L, Dan Z (2009) Incidence of mandibular incisors with twice canals in Jilin province. Poster presented at: The 3rd Symposium of Chinese of Conservative Dentistry & Endodontic Clinical Technique: Chongqing, People’s Republic of China, 90.
-
Ying Z, Yingtao D, Xiaoyan W, Wang ZH, Li G, et al. (2014) Cone-beam computed tomography analysis of root canal configuration of 4674 mandibular anterior teeth. J Peking Univ Health Sci 46(1): 95-99.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage