Superior Semicircular Canal Dehiscence Commonly Ignored Diagnosis-A Case Report
Superior semicircular canal dehiscence (SSCD) is a condition caused by the absence of bone over one or both of the superior semicircular canals that leads to dysfunction of the vestibular end as result of formation of third window besides round and oval window resulting in altered fluid dynamics. We present a case of 48 year old man presenting with vertigo and aggravation of symptoms with noise. CT temporal bones revealed, bilateral SSCD which was detected in 5 mm interval coronal images. Thus in a middle age group individual presenting with vertigo a diagnosis of dehiscent superior semicircular canal should be considered.
Introduction
Superior Semicircular Canal Dehiscence (SSCD) is defined as an absence of bony covering of the membranous labyrinth of the superior semicircular canal [1]. In some patients, this finding is associated with a constellation of symptoms including autophony, aural fullness, sound and pressure-induced vertigo, tinnitus, and conductive hearing loss1. The prevalence of SSCD is unknown and varies depending on the detection modality utilized. While the classic presentation can be suspected on clinical and audiometric data, imaging plays an important role in the evaluation of these patients [1, 2]. Advances in CT now allow submillimeter high resolution images to demonstrate the bony defect, while multiplanar reformations can also aid in the radiological diagnosis [3].
Discussion
Superior semicircular canal dehiscence is described superior semicircular canal abnormality, where a clinical disequilibrium phenomenon is associated with the absence of its bony covering. Patients presents commonly with vertigo [2, 3], Tulio phenomenon is associated with SCCD where patients experience vertigo and nystagmus with loud noises [4]. In practical experience at our institution, the radiologic diagnosis of SSCD is made more commonly among middle and older age groups [5, 6]. There is a statistically significant increase in the prevalence of radiographic dehiscence as age increases and an increasing trend but no significant increase in prevalence of thinning with age [6]. No significant association between thinning and contralateral dehiscence or vice versa, suggesting that thinning occurs independently of dehiscence [5]. While there may be a congenital basis for some cases of SSCD, our data support the impression that SSCD is more commonly an acquired rather than a congenital/developmental condition [7, 8].
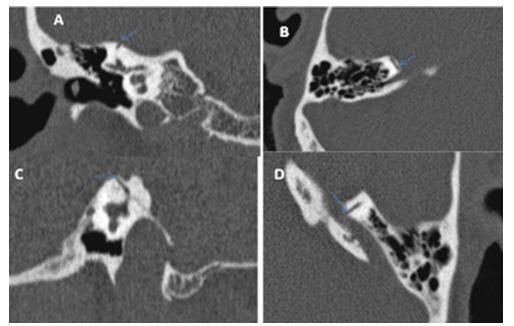
The key diagnostic features on CT imaging are a defect in the bony covering of the SSC, best seen in the coronal plane in thin slice temporal bone CT demonstrates and on Pöschl and Stenver reformatted images together with axial images improves the diagnostic efficacy [9, 10].
Differential Diagnosis that can be considered are thinning of arcuate eminance that is the bony covering of semi-circular canal may be seen due to ageing .Treatment is mainly Surgical Plugging or resurfacing the superior semicircular canal has been documented to resolve or improve the symptoms [9, 10].
Conclusion
The prevalence of SSCD as well as SSC thinning, being in same etiological spectrum and acquired conditions increases with age which is now a well established relationship. The association with CSOM and cholesteatoma was not found which is again important for the operating surgeon. HRCT imaging provide important tool in diagnosing the condition in clinically suspected individuals. Thus in a middle age group individual presenting with vertigo a diagnosis of dehiscent superior semicircular canal should be considered.
References
-
Minor LB, Solomon D, Zinreich JS, Zee DS (1998) Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg 124(3): 249-258.
-
Nadgir RN, Ozonoff A, Devaiah AK, Halderman AA, Sakai O (2011) Superior semicircular Canal Dehiscence: Congenital or acquired condition?. American Journal of Neuroradiology 32(5): 947-949.
-
Zhou G, Ohlms L, Liberman J, Amin M (2007) Superior semicircular canal dehiscence ina young child: implication of developmental defect. Int J Pediatr Otorhinolaryngol 71(12): 1925-1928.
-
Hirvonen TP, Weg N, Zinreich SJ, Minor LB (2003) High-resolution CT findings suggest a developmental abnormality underlying superior canal dehiscence syndrome. Acta Otolaryngol 123(4): 447-481.
-
Carey JP, Minor LB, Nager GT (2000) Dehiscence or thinning of bone overlying the superior semicircular canal in a temporal bone survey. Arch Otolaryngol Head Neck Surg 126(2): 137-147.
-
Williamson RA, Vrabec JT, Coker NJ, Sandlin M (2003) Coronal computed tomography prevalence of superior semicircular canal dehiscence. Otolaryngol Head Neck Surg 129(5): 481-489.
-
Masaki Y (2011) The prevalence of superior canal dehiscence syndrome as assessed by temporal bone computed tomography imaging. Acta Otolaryngol 131(3): 258-262.
-
Crovetto M, Whyte J, Rodriguez OM, Lecumberri I, Martinez C, et al. (2010) Anatomo-radiological study of the Superior Semicircular Canal Dehiscence Radiological considerations of Superior and Posterior Semicircular Canals. Eur J Radiol 76(2): 167-172.
-
Cloutier JF, Belair M, Saliba I (2008) Superior semicircular canal dehiscence: positive predictive value of high-resolution CT scanning. Eur Arch Otorhinolaryngol 265(12): 1455-1460.
-
Lee GS, Zhou G, Poe D, Kenna M, Amin M, et al. (2011) Clinical experience in diagnosis and management of superior semicircular canal dehiscence in children. Laryngoscope 121(10): 2256-2261.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage