Spontaneous Retroperitoneal Hematoma: A Case Report
Spontaneous retroperitoneal hematoma is a rare condition caused by extravasations of blood into the retroperitoneal space with no history of external trauma or previous vascular procedures. Its clinical presentation can be insidious, evolving for a few days, or sudden, depending on the amount of bleeding. The classic triad of presentation, called Lenk’s triad, characterized by abdominal pain, palpable mass and hypovolemic shock. Diagnosis is made by imaging studies such as computed tomography (CT) or ultrasound. Treatment can be surgical or conservative depending on the hemodynamic status of the patient. In the case, the patient presented a sudden low back pain on the left, with a slow decrease in hematocrit, however, no signs of significant hemodynamic changes during hospitalization and the diagnosis was demonstrated by means of abdominal CT that showed the presence massive retroperitoneal hematoma left encompassing the left adrenal and perirenal fascia. There was no report of previous external trauma, but the patient had a regular use of acetylsalicylic acid (ASA) 100 mg daily. The CT scan did not show any other changes that could have caused the bleeding. The treatment was conservative, and the patient was discharged after 11 days of hospitalization. The diagnosis was spontaneous retroperitoneal hematoma due to spontaneous arterial injury by minimal effort or aggravated by the use of ASA.
Introduction
Spontaneous retroperitoneal hematoma is a rare pathology characterized by extravasations of blood in the retroperitoneal space with no history of external trauma or associated prior vascular procedures. As a clinical manifestation, the presence of abdominal pain, anemia, palpable abdominal mass and hemodynamic instability are highlighted, being more common hypotension and hypovolemic shock. Its etiology is varied, and may include more commonly renal pathologies, such as malignant or benign tumors, inflammatory processes and vascular alterations. In the reported clinical case, no other pathology was found, and the hematoma was associated with the use of ASA.
Clinical Case
A 64-year-old Caucasian male was admitted to the Emergency Department with left lumbar pain, of sudden onset in the morning, of strong intensity and type "tearing". At the physical examination, he was expressed himself clearly, with important pain's facies, hydrated, acyanotic, anicteric, tachypneic, denied alterations of the intestinal habit, hematuria and / or local trauma. Abdomen: globose, depressible, and painful to superficial and deep palpation in the left flank, tympanic.
Previous pathological history: Prostate cancer, radical prostatectomy in 2010, infraumbilical incisional hernioplasty in 2012; systemic arterial hypertension in daily use of metoprolol 50 mg, losartan potassium 100 mg, sinvastatina 40 mg, hydrochlorothiazide 50 mg, ASA 100 mg and daflon® 500 mg.
Laboratory tests were performed, which showed: hematocrit 39.8%; hemoglobin 13.6 mg / dl; leukometry 12,000 without left shift, platelet count 275,000, TAP 68%; PTT 33 s; INR 1.3; urea 38 mg / dl; creatinine 1.3 mg / dL; glucose 147mg / dl; TGO 33U / l; TGP 29U / l; alkaline phosphatase 50 U / l, Gama GT 32U/l, amylase 53mg / dl, sodium 136 Meq/l; total bilirubin 0.9mg / dl; direct bilirubin 0.2mg / dl, indirect bilirubin 0.7mg / dl.
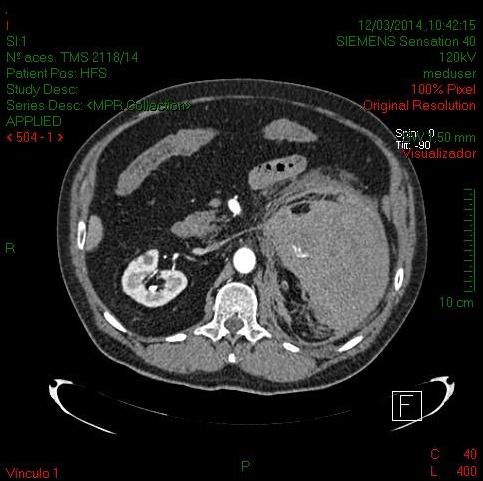
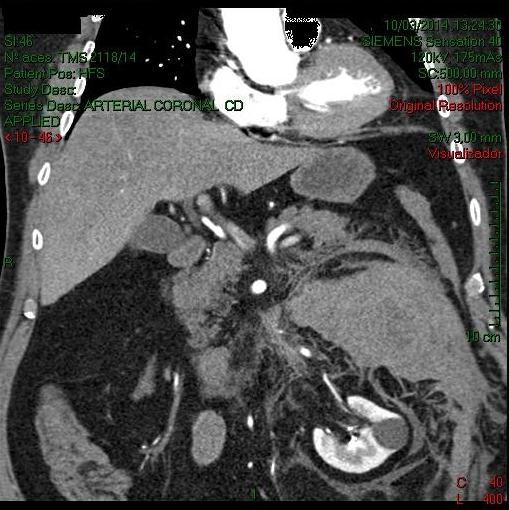

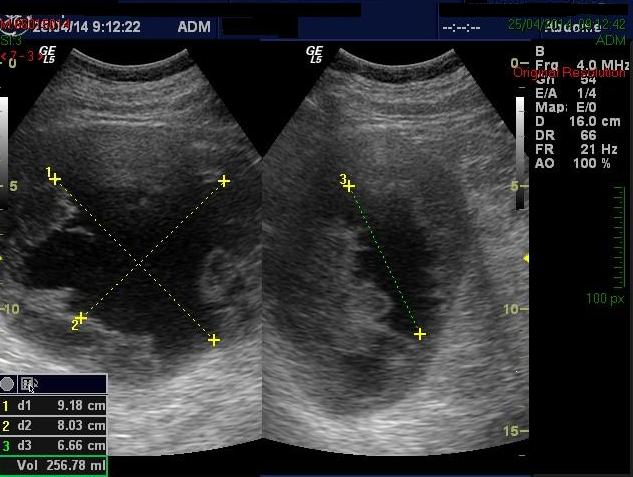
Enhanced CT of the abdomen and pelvis showed a massive left retroperitoneal hematoma encompassing the left adrenal and the perirenal fascia on this side. The lesion measured 9.0 x 11.0 x 19.0cm, and it pushed the left kidney down (Figures 1&2). An abdominal ultrasonography was performed, showing a heterogeneous collection, displacing the left kidney down, and adjacent to the head of the pancreas, measuring 16.7 x 10.3 x 12.6 cm, with an estimated volume of 1,127cc Small pleural effusion on the left Figure 3.
He evolved well with improvement of the pain and the laboratory and imaging exams, remaining hemodynamically stable. The option for a conservative treatment with suspension of the anti-platelet aggregation and follow-up by serial ultrasonographic examination was used Figure 4. The diagnostic hypothesis was spontaneous retroperitoneal hematoma due to spontaneous arterial injury or minimal effort aggravated by the use of ASA. He was discharged from hospital after 11 days of hospitalization, with orientation, regular analgesia, rest and return to control the collection resorption through ultrasonographic examination.
Patient was referred to the intensive unit for assisted observation and monitoring. At the moment of admission there was no indication of surgical intervention due to hemodynamic stability. The blood pressure was 86X62mmHg, heart rate was 77, requiring increased of the venous hydration. It evolved with fall of hematocrit and platelets, but remained hemodynamically stable.
Hemoglobin 9.2 mg / dl; hematocrit 27.1%; PTT 34.3 s; TAP 73%; INR 1.23; platelet count 184,000. The control CT performed on the third day of hospitalization showed no significant evolutionary modification in the in the collection's volume.
Discussion
Spontaneous retroperitoneal hematoma is a relatively rare entity, characterized by the formation of a blood collection in the retroperitoneal space of non-traumatic etiology, and may be associated with varied pathologies of any retroperitoneal structure, more frequently at the renal level, like malignant tumors followed by benign tumors; vascular and inflammatory alterations were the most prevalent [1].
Hereditary or acquired blood dyscrasias may also be cause of the retroperitoneal hematoma, when no pre- existing pathology is seen in viscera of that region. Among the hematological causes are thrombocytopenic purpura, leukemia, myeloma, hemophilia, polycythemia and therapeutic anticoagulation.
Treatment with oral anticoagulants is the most frequent cause among blood dyscrasias and the incidence of retroperitoneal hematoma in these cases may vary from 0 to 0.6% [2]. There is no evidence that acetylsalicylic acid is the source of the hematoma, but its continued use may aggravate previous bleeding. Other associated clinical factors, such as arterial hypertension, arteriosclerosis and arterial vascular malformations may predispose to bleeding [3].
Studies show that renal tumors are the most frequent causes with an incidence of about 57 to 63%, followed by vascular alterations with 18 to 26%, and inflammatory conditions with about 11% of cases [4, 5]. Among the renal tumors, the majority is of benign origin, being angiomyolipoma responsible for 15% of the cases. Of malignant tumors, renal adenocarcinoma is the most frequent, with an incidence of 0.3 to 1.3% [4, 5]. Other frequent causes of retroperitoneum spontaneous bleeding of renal origin include renal infarction, pyelonephritis, tuberculosis, cortical abscesses, vasculitis, arteriovenous fistulas, vascular malformations, rupture of cysts, lithotripsy, among others. Among the causes of extrarenal origin are: retroperitoneal tumors (liposarcoma, fibrous histiocytoma, schwannomas and gangliomas), rupture of aortoiliac aneurysm, aneurysm and microaneurysm of visceral arteries, spontaneous rupture of the iliac vein, adrenal masses, adenomas, cysts), spontaneous bleeding of the psoas muscle and ectopic pregnancy [1].
The clinical presentation of the retroperitoneal hematoma depends on the intensity and duration of the bleeding, which may have an insidious onset, evolving for a few days, or sudden onset. There is no pathognomonic signal, but abdominal and / or lumbar pain is the main symptoms. The classic triad of presentation, called Lenk’s triad, is characterized by abdominal pain, palpable mass and hypovolemic shock, being present in about 30% of the cases [4]. About 60% of the cases may present with a femoro crural neuropathy [3, 6]. We may also find hematuria, fever, nausea and vomiting and signs of peritoneal irritation, but these signs and symptoms are less frequent.
The diagnosis is made by imaging exams, such as abdomino-pelvic CT or abdominal ultrasonography. Computed tomography is the method of choice because, in addition to detecting the image with high values of attenuation compatible with bleeding, and determining its extent, it can also detect the cause of bleeding, such as the presence of tumors or vascular lesions. Abdomino-pelvic CT has 100% sensitivity for the detection of retroperitoneal bleeding and the ultrasound has a sensitivity of up to 76.4% for the diagnosis [7]. Selective arteriography may be indicated for investigation of vascular pathologies, but in acute cases its sensitivity is low because it only detects active bleeding if the flow is greater than 1 ml / minute [1].
The treatment will depend on the hemodynamic condition of the patient. In cases of hemodynamic instability where blood and volume replacement and correction of coagulopathy cannot stabilize the patient, or when the cause of the bleeding is detected, surgical intervention is indicated for drainage of the hematoma and correction of the cause [7, 8]. Surgery when indicated should be as conservative as possible [5, 8]. In cases where the patient has hemodynamic stability and the origin of the bleeding is not detected, a conservative treatment can be chosen, with periodic monitoring of the hematoma size by imaging tests [1, 7, 8]. The most recommended therapy is conservative treatment with analgesia and correction of coagulation disorders [6, 8].
In this case, the patient had no history of recent trauma and / or surgical procedures, with only regular use of ASA and systemic arterial hypertension as predisposing factors. The diagnosis was made after a CT scan that showed the hematoma and excluded other obvious causes for bleeding. The treatment was conservative, with volume replacement and oral anticoagulation suspension. The patient progressed well, and after 11 days of hospitalization, he was discharged from hospital and returned for medical monitoring at the outpatient clinic.
Conclusion
Spontaneous retroperitoneal hematoma is a rare pathology for being a bleeding into the retroperitoneal space without prior history of external trauma or neurovascular surgical procedures. Its etiology can be varied, being more frequently from injury of renal origin. The clinical featuring presents with abdominal pain, palpable abdominal mass and hypovolemia. The diagnosis is made through imaging methods such as abdomino- pelvic CT or abdominal ultrasonography. Treatment may be conservative or surgical depending on the patient's hemodynamic status and findings of associated pathologies on imaging examinations. The important thing after hospital discharge is to maintain a periodic control through computed tomography examinations due to the frequent association of retroperitoneal hematoma with small tumors.
References
-
Pérez MA, Quinteiro SC, Del Rio JAC, Suaréz LC, Insua JV, et al. (1998) Hematoma retroperitoneal espontâneo como causa de dolor abdominal y shock hemorrágico. Angiologia 50(2): 95-98.
-
Figueirol VC, Salgueiro MA, Leme MBP, ACBC-RJII, TCBC-RJIII (2005) Hematoma retroperitoneal espontâneo: Relato de Caso. Rev Col Bras Cir 32(1): 52-53.
-
Alvarez CZ, Cerda CC, Jadue AT, Rojas FR, Abelleira MP, et al. (2007) Hematoma retroperitoneal espontáneo: Caso clínico. Rev méd Chile 135(8): 1044-1047.
-
Gimeno VA, Bosquet MS, Ramírez MB, Trassierra MV, Arlandis SG, et al. (2007) Hemorragia retroperitoneal espontánea: nuestra experiencia en los últimos 10 años. Actas Urol Esp 31(5): 521-527.
-
Sancho GP (2016) Hemorragia retroperitoneal espontânea. Rev Méd Costa Rica Centroamérica 73(618): 131-134.
-
Gómez RT, Milla AC, Cadenas F, Fernández JB, Vázquez MC (2003) Hematoma retroperitoneal espontáneo inducido por enoxiparina a dosis terapêuticas. An Med Interna 20(7): 386-387.
-
Sierra-Díaz E, Belmonte-Hernández MV, Villanueva- Pérez MA, García-Gutiérrez M (2015) Hemorragia retroperitoneal espontánea no traumática: efecto del diagnóstico preciso y oportuno. Cirugía y Cirujanos 83(3): 206-210.
-
Bianchi D, Bernabei E, De Majo A, Athanasopoulou E, Venditti D, et al. (2015) Spontaneous Retroperitoneal Hemorrhage: a Case Report and an Overview of the Literature. La Prensa Med Argent 101: 5.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage