Pulmonary Infarction in Pulmonary Embolism
We present a case of 45-year-old woman who developed pulmonary infarction in pulmonary embolism, in a postoperative context. We review all imaging characteristics of this pathology, whose recognition is sometimes difficult due to wide spectrum of findings it can take.
Introduction
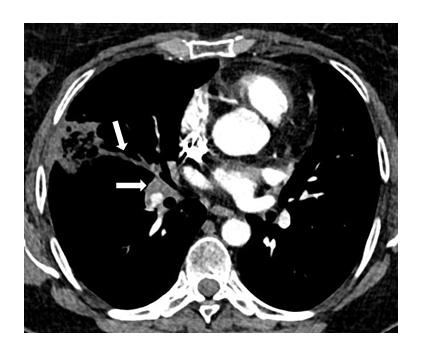
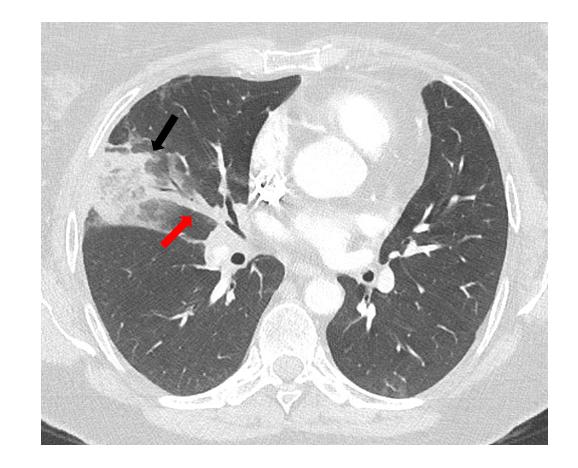
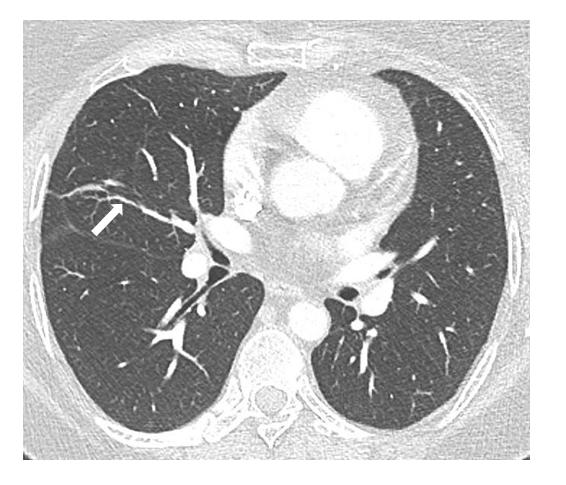
A 45-year-old woman presented to the emergency room for progressive stress dyspnea and respiratory- dependent chest pain for three weeks, in the postoperative period of hysterectomy for oncologic purpose. Clinical examination revealed that mild tachycardia (104 bpm), decrease of pulse oximetry at 93% and right basal hypoventilation. Biochemical examination included elevation of CRP to 161 mg/L and D-dimer to 2720 ng/mL, without leukocytosis. Thoracic CT angiography demonstrated multiple segmental acute pulmonary embolisms (Figure 1) with peripheral round pulmonary consolidation bordered by ground glass (halo sign) in the middle lobe and pulmonary infarction (PI) (Figure 2) [1]. Cardiopulmonary support and anticoagulation permitted fast recovery of the patient. Control CTs performed as part of oncological monitoring at 1, 6 and 12 months revealed progressive resolution of infarction with residual linear scar (Figure 3).
Discussion
Pulmonary infarction (PI) is usually caused by pulmonary embolism (PE), it concerns a minority of the patients affected (10 – 30%) [2].
Predisposing factors for PI are higher height, smaller BMI, active smoking and age higher than 40 years old. There is no correlation between PI and malignant disease, chronic bronchitis, cardiac congestion, quantified clot burden score and severity of symptoms. The pathogenesis of pulmonary infarction is controversial and only a few studies were dealing this subject. Multiple etiopathogenic factors seem to be involved like the location of the clot, the speed at which occlusion develops, the ability of bronchial circulation to compensate and possibly the role of elevated pulmonary venous pressure. The coagulative ischemic necrosis can result in complete or incomplete PI, with respectively either fibrotic scar (as in our case) or resolving opacity in few days with “Melting Ice Cube Sign”.
The clinical presentation includes dyspnea, cough, pleuritic or substernal chest pain, haemoptysis, fever, diaphoresis and signs of DVT like leg swelling or pain. The cardiopulmonary examination can reveal tachypnea, tachycardia with or without gallop rhythm, crackles, cyanosis, hypoxemia or pleural rub. Most of these signs are non-specific.
HRCT signs of pulmonary infarction are various and the study by Revel et al illustrates well the difficulty to affirm PI when analysing CT alone without clinical context [3]. Described signs consist of subpleural wedge-shaped consolidation with convex borders in area of low attenuation. Consolidation can have truncated apex (Hampton hump sign) or present central lucencies with bubbly consolidation and thickened vessel leading to the apex of the opacity (vascular sign). The consolidation may also be surrounded by focal ground glass opacities (halo sign) secondary to adjacent alveolar haemorrhage or vice versa (reversed halo sign). Slight continuous FDG uptake along the border of subpleural consolidation with photopenic center can be demonstrated on TEP-CT (rim sign) [4, 5, 6].
Conclusion
PI diagnosis may be challenging, especially because HRCT signs have variable specificity but low sensitivity, they are thereby useful to know.
Competing Interests: The authors have no competing interests to declare.
References
-
Revel MP, Triki R, Chatellier G, Couchon S, Haddad N, et al. (2007) Is it possible to recognize pulmonary infarction on multisection CT images? Radiology 244(3) : 875-882.
-
He H, Stein MW, Zalta B, Haramati LB (2006) Pulmonary Infarction: spectrum of findings on multidetector helical CT. J Thorac Imaging 21(1): 1-7.
-
Bray TJP, Mortensen KH, Gopalan D (2014) Multimodality imaging of pulmonary infarction. Eur J Radiol 83(12): 2240-2254.
-
Soussan M, Rust E, Pop G, Morère JF, Brillet PY, et al. (2012) The rim sign: FDG-PET/CT pattern of pulmonary infarction. Insights Imaging 3(6): 629- 633.
-
Kirchner J et al. (2015) PI following PE: a comparative study on clinical conditions and CT findings to identify predisposing factors. ROFO 187: 440-444.
-
Miniati M, Bottai M, Ciccotosto C, Roberto L, Monti S (2015) Predictors of pulmonary infarction. Medicine 94(41): 1488.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage