Isolated Craniofacial Skeletal Involvement in Primary Hyperparathyroidism: A Report of Three Cases
Osteosclerotic and osteolytic lesions isolated to the skull/facial bones have rarely been reported among patients with hyperparathyroidism. There have been anecdotal reports of discrete localised bony lesions in these patients. Such lesions present a radiological challenge and might be confused with metastatic lesions. Here, we report three cases of hyperparathyroidism with two presenting with isolated osteosclerotic lesions in the skull and one presenting with a jaw swelling. The aim of this case series is to familiarize the clinicians and the radiologists with such atypical presentations.
Srishti, Kumar I*, Verma A, Singh PK and Shukla RC
0542-2369024; Email: ishanjd@gmail.com
Adenoma
Introduction
Due to its distinctive clinical picture, Hyperparathyroidism was classically described as a syndrome of “stones, bones, abdominal groans, thrones and psychiatric overtone”. However, clinical and radiological manifestation of this entity is varied and can manifest as limited involvement of skeletal system and elevated blood calcium level. Due to increased early detection, the frank skeletal presentations of osteitits fibrosa cystica and pathological fractures are uncommon in modern medicine and variable degree of skeletal involvement is currently observed. Common Radiological features of primary hyperparathyroidism include diffuse osteopenia with superimposed bone resorption. The bony resorption in these cases can be (a) subperiosteal, showing lacelike irregularity of cortical margin particularly involving the radial aspect of middle phalx of Isolated Craniofacial Skeletal Involvement in Primary Hyperparathyroidism: A Report of Three Cases
2nd and 3rd fingers, (b) subchondral causing pseudo- widening of joint spaces, (c) subligamentous involving the inferior aspect of calcaneum, clavicle, greater trochanter, ischial tuberosity, anterior inferior iliac spine and (d) Cortical, due to osteoclastic activity within haversian canals [1, 2, 3, 4, 5]. Subperiosteal resorption is the most constant and most specific finding and is considered to be virtually pathognomonic of hyperprathyroidism. Usually, osteosclerotic changes manifest as patchy or diffuse increase in bone density in the spine, skull, and pelvis. While diffuse or patchy osteosclerosis has been described rarely among these patients, localised well-defined osteosclerotic lesions have anecdotally been reported [6]. Here we present rare presentations of primary hyperparathyroidism which may be confused with osteoblastic or osteolytic metastatic lesions and expose the patient to a battery of investigations in a vain effort to search for a primary malignancy.
Clin Radiol Imaging J
Case Reports
Case 1
A 30-year-old female presented with a history of headache, bony aches and progressive proximal muscular weakness since the last 2 years. Investigations revealed hypercalcaemia (12.3 mg/dl), hypophosphataemia (2.1 mg/dl) with raised ALP levels (985 U/litre). Renal parameters were within normal limit. Skull axial computerised tomography revealed multiple high density foci clearly demarcated from surrounding bone involving both the skull vault and skull base. Inner and outer cortex of bone was maintained (Figures 1A-B). Ultrasound (Figure 1C) of the neck revealed a well-defined hypoechoic lesion noted overlying the left lobe of thyroid showing characteristic rim of vascularity consistent with parathyroid adenoma. Serum intact parathyroid hormone was high (PTH: 981 pg/ml).
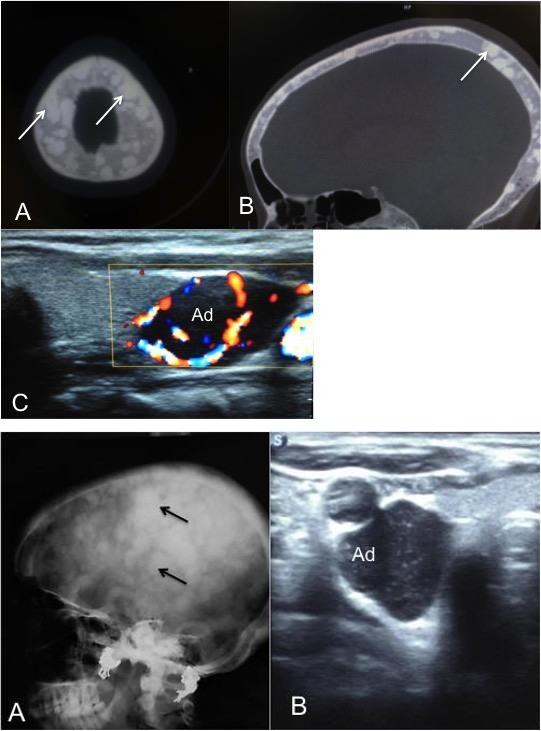
Figures 1(A-C): Axial CT showing multiple well marginated sclerotic foci (arrows) both the skull vault and skull base, Inner and outer cortex of bone was maintained (A-B), Ultrasound (C) of the neck revealed a well-defined hypoechoic lesion (ad) noted overlying the left lobe of thyroid showing characteristic rim of vascularity.
Case 2
The second patient was a 22 year old male who presented with the chief presenting complaints of headache, lower limb weakness and difficulty in walking.
Radiological skeletal survey revealed multiple well defined variable sized osteosclerotic foci involving skull bones superimposed on a homogenous ground glass background (Figure 2A).
Figures 2A,B: Lateral skull showing multiple well defined variable sized osteosclerotic foci (black arrows) involving skull bones superimposed on a homogenous ground glass background (A), Ultrasound reveals parathyroid adenoma (ad) overlying the left lobe of thyroid (B).
Rest of the skeletal survey was within normal limits. Ultrasound of the neck revealed a well-defined hypoechoic lesion overlying the left lobe of thyroid suggestive parathyroid adenoma (Figure 2B).
Case 3
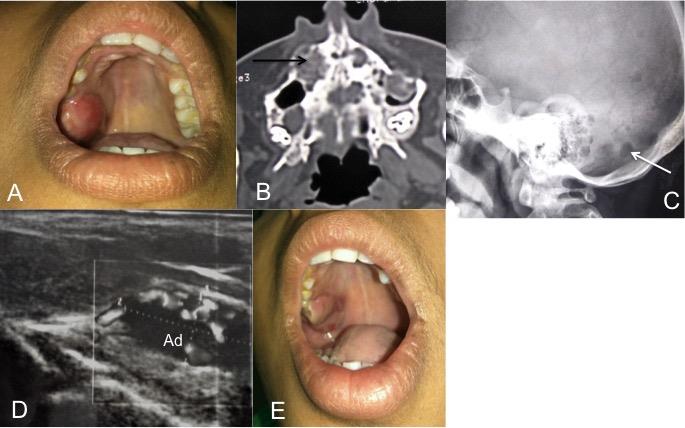
A 16 year old female presented with a swelling in the region of right upper alveolar margins for three months without complaints of pain or ulceration over the swelling (Figure 3A). General and systemic examinations were within normal limit. Biochemical investigations revealed revealed hypercalcaemia (12 mg/dl), hypophosphataemia (3.8 mg/dl) with raised ALP levels (786 U/litre). CT scan has done for further characterization of the lesion a lytic lesion involving the right maxillary bone with ground glass matrix (Figure 3B). Few well defined lytic lesions were also noted in the occipital bone as can be seen in the lateral skeletal radiograph of the patient (Figure 3C). Based on the above findings, cranio facial fibrous dysplasia, lesions of osteitis fibrosa cystica and osteolytic metastatic lesions were considered as the most probable differentials. USG neck done to rule out Osteitis fibrosa cystica revealed a parathyroid adenoma inferior to left thyroid lobe (Figure 3D). TheI-PTH levels were 1121 pg/dl. The subsequent removal of the parathyroid adenoma resulted in reduction in the size of the swelling (Figure 3E).
Discussion
The usual skeletal manifestation of hyperparathyroidism is diffuse osteopenia, subperiosteal, lamina dura, subchondral, subligamentous and intracortical bone erosion, acroosteolysis, salt-pepper skull, chondrocalcinosis and brown’s tumor. Osteosclerosis is rare in adults with primary hyperparathyroidism [7]. On the other hand, in secondary hyperparathyroidism associated with renal osteodystrophy, diffuse osteosclerosis and rugger Jersy spine is not uncommon [7]. Brown tumours may be noted as a central, slightly expansile and lightly septated distinct radiographic lucencies caused by localized replacement of bone by vascularized fibrous tissue which after undergoing necrosis and liquefaction becomes cystic. Brown tumors represent a reparative cellular process with localized accumulation of fibrosis tissue and giant cells. It can replace bone and even produce osseous expansion. Radiographically, these are osteolytic lesions with eccentric or cortical location with well-defined margins; most commonly occur in facial bones and jaws, pelvis, ribs, femurs and other long bones. Histopathologic findings consist of osteoclastic resorption with cavities filed with fibrous tissue, giant cells, hemosiderin deposits and macrophages [8]. These may heal byremineralization of the brown tumors with osteoblastic transformation due to reversal of the parathyroid hormone showing dense sclerotic appearance [9].
A roentgenogram showing focal osteosclerotic lesions is an uncommon feature of primary hyperparathyroidism as seen in the first two cases. Fujino Y, et al. published a report describing multiple osteosclerotic skull lesions in a 26-year patient suffering from primary hyperparathyroidism [10]. Boechat et al. reported two children with primary hyperperathyroidism, who presented with tibial osteosclerosis [11]. Chopra and his colleagues reported two female patients with osteosclerotic skull lesions [12]; one with primary hyperparathyroidism, and the other with vitamin D deficiency leading to secondary hyperparathyroidism. The exact mechanism and pathogenesis of osteosclerotic lesionsin primary hyperparahyroidism is still mysterious. However the sclerotic lesions might represent remineralized or healed brown tumours [7]. Some also consider the osteosclerotic foci a result of occasional and exaggerated response of osteoblasts to compensate for the bone loss induced by hyperparathyroidism [10, 13]. The lytic lesions noted in the third case are a common presentation of primary hyperparathyroidism and can commonly be confused with metastatic lesions [9, 14]. Alvin, et al. reported a case where a 61 year old male presented with generalized bone pain and multiple well- defined pure osteolytic lesions in the pelvic girdle, proximal femoral shafts and skull mimicking metastatic disease with pathologic analysis revealing brown tumor [15, 16].
The importance of accurate diagnosis in such cases cannot be overemphasized. The presence of multiple osteolytic lesions, some with well-defined or even sclerotic borders, while others showing expansive soft- tissue components, in a patient without known primary are highly suggestive of brown tumors. In conclusion, the present cases with multiple localised osteosclerotic or osteolytic foci in the calvarium are rare presentations of primary hyperparathyroidism and should always be considered in the differential when such lesions are encountered.
References
-
Chang CY, Rosenthal DI, Mitchell DM, Atsuhiko H, Susan VK, et al. (2016) Imaging Findings of Metabolic Bone Disease. Radio Graphics 36(6): 1871-1887.
-
Khan A, Bilezikian J (2000) Primary hyperparathyroidism: pathophysiology and impact on bone. CMAJ 163(2): 184-187.
-
Murphey MD, Sartoris DJ, Quale JL, Pathria MN, Martin NL (1993) Musculoskeletal manifestations of chronic renal insufficiency. Radio Graphics 13(2): 357-379.
-
Resnick D, Deftos LJ, Parthemore JG (1981) Renal osteodystrophy: magnification radiography of target sites of absorption. AJR Am J Roentgenol 136(4): 711- 714.
-
Resnick D, Niwayama G (1976) Subchondral resorption of bone in renal osteodystrophy. Radiology 118(2): 315-321.
-
S Chopra, S Manchanda, D Kothari, Kulshreshtha B (2012) Multiple osteosclerotic lesions of skull in two cases with co-existing hyperparathyroidism and vitamin D deficiency. JIACM 13(4): 349-351.
-
Genant HK, Baron JM, Straus FH, Paloyan E, Jowsey J (1975) Osteosclerosis in primary hyperparathyroidism. Am J Med 59(1): 104-113.
-
Jouan A, Zabraniecki L, Vincent V, Poix E, Fournie B (2008) An unusual presentation of primary hyperparathyroidism: severe hypercalcemia and multiple brown tumors. Joint Bone Spine 75(2): 209- 211.
-
Moran LM, Moeinvaziri M, Fernandez A, Sánchez R (2016) Multiple brown tumors mistaken for bone metastases. Computed tomography imaging findings. The Egyp J Radiol Nuclear Med 47(2): 537-541.
-
Fujino Y, Inaba M, Nakatsuka K, Kumeda Y, Imanishi Y, et al. (2003) Primary hyperparathyroidism with multiple osteosclerotic lesions of the calvarium. J Bone Miner Res 18(3): 410-412.
-
Boechat MI, Westra SJ, Van Dop C, Kaufman F, Gilsanz V, et al. (1996) Decreased cortical and increased cancellous bone in two children with primary hyperparathyroidism. Metabolism 45(1): 76-81.
-
Wolf HL, Denco JV (1958) Osteosclerosis in chronic renal disease. Amer J Med Sci 235: 33-42.
-
Ellis K, Hochstim RJ (1960) The skull in hyperparathyroid bone disease. Am J Roentgenol Radium Ther Nucl Med 83: 732-742.
-
Su AW, Chen CF, Huang CK, Chen PC, Chen WM, et al. (2010) Primary Hyperparathyroidism With Brown Tumor Mimicking Metastatic Bone Malignancy. J Chin Med Assoc 73(3): 177-180.
-
Eugenidis N, Olah AJ, Haas HG (1972) Osteosclerosis in hyperparathyroidism. Radiology 105(2): 265-275.
-
Templeton AW, Jaconette JR, Ormond RS (1962) Localized Osteosclerosis in Hyperparathyroidism. Radiology 78(6): 955-958.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage