Case of a Liver Abscess Due to Fishbone-Diagnostic Challenge
Liver abscesses are relatively rare, especially these ones caused by foreign bodies that reached the liver by penetrating the gastrointestinal tract. We present a case of a 52- year old lady with a liver abscess which etiology was found after percutaneous abscess drainage. After the procedure, the patient was treated conservatively with a favorable outcome. Interventional radiology procedure is intended to help clear the etiology and the medical treatment of a liver abscess.
Introduction
The etiology of liver abscesses can be classified in a variety of ways. Understanding the source for a liver abscess is crucial because it aids in the determination of the type of treatment [1]. A foreign body in the liver is relatively rare and can be a diagnostic challenge. We present a case of a 52-year- old lady who presents only with upper abdominal pain and distension and finally diagnosed and treated for liver abscess due to fishbone.
Case Report
A 52-year old lady presents to the emergency department with mild to moderate upper abdominal pain and abdominal distension, without any positive symptoms of the acute surgical abdomen, no fever, vomiting, or nausea. She had no history of gastrointestinal diseases and her blood investigation was within normal. On further history, she reported having had dental issues and at that time, she had been started on spiramycin/metronidazole for the treatment of tooth abscess.
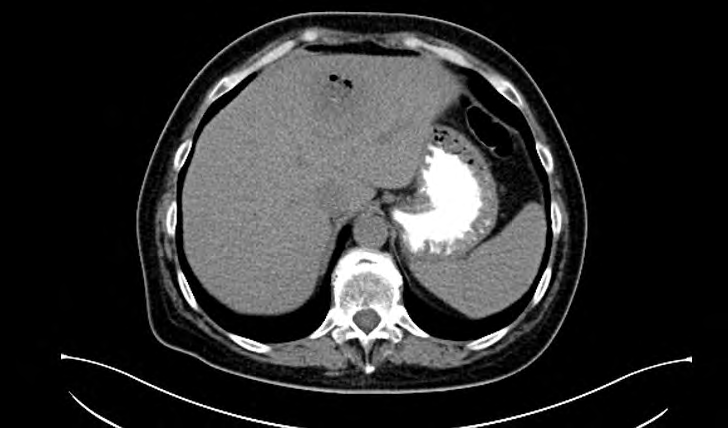
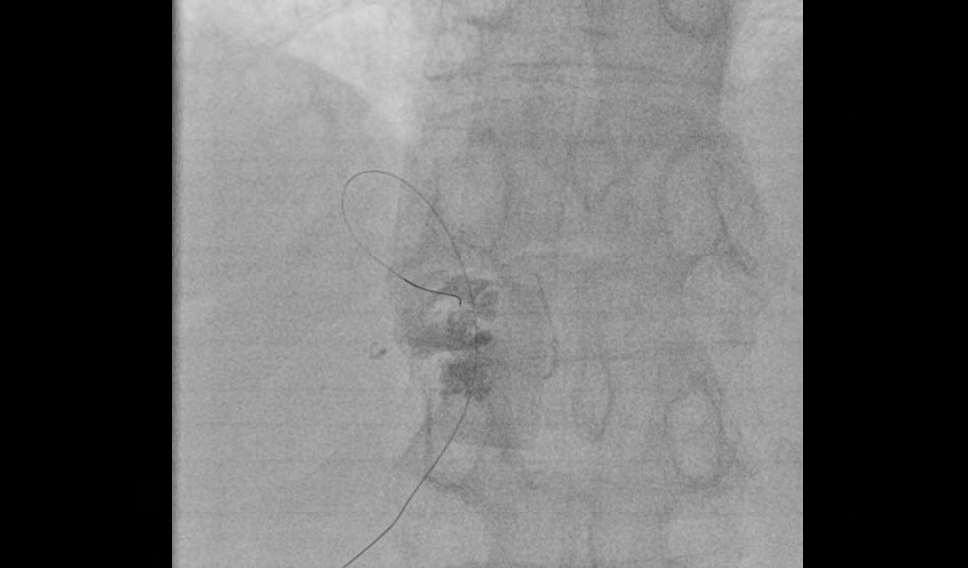
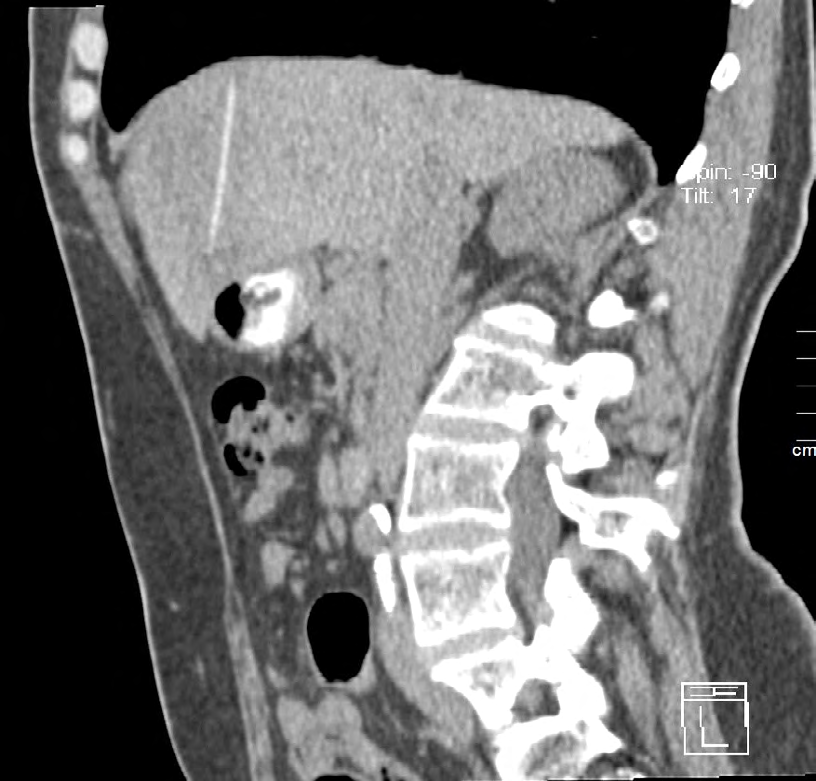
Abdominal X-ray and ultrasound were performed with signs of hepatomegaly, no evidence of pneumoperitoneum, air-fluid levels in bowels, or any lesions. Due to her persistent abdominal pain CT was ordered and revealed hypoattenuate 4cm solid lesion with peripheral enhancement and gas in segments 4 and 2 of the liver. There was evidence of thickened stomach wall associated with discreet intramural air bubbles. The source of the abscess was not discovered and percutaneous abscess drainage under fluoroscopic guidance was performed. Three days after the procedure of pus aspiration CT was performed again. The images of the latest CT showed heterodense zone where the abscess was situated and foreign body /FB/ 85HU, 6/0.3 cm in size was localized within its boundaries. The FB was categorized as fishbone because of its shape and confirmation by the patient for fish consummation a day before her complaint had been started. The patient was treated conservatively, she recovered unremarkable and had been under follow-up by ultrasound exams with no complications (Figures 1-6).



Discussion
Liver abscesses are not a common condition. Most symptoms are non-specific and diagnosis requires a high index of suspicion [2]. It is imperative to recognize the source for the liver abscess and to treat it upon discovery. Fishbone as a foreign body in the liver is an extremely rare and most frequent way of penetration is migration through the gastrointestinal tract /stomach, duodenum/ [3, 4]. Our patient had only abdominal pain and evidence of hepatomegaly showed on abdominal X-ray. CT is the first choice of modality because of its high resolution [5]. In our case, the first CT scan confirmed lever abscess, did not reveal its source but discovered a thickened stomach wall and intramural air bubbles. Drainage of the abscess was needed as the first step of treatment [1]. Procedures of needle aspiration and catheter placement were sufficient for detecting the causative factor of the liver abscess during post aspiration CT performance in which a foreign body with fishbone shape was discovered. Retrospectively, secondary findings into the stomach wall suggested the migration of the FB in the liver through the gastrointestinal tract.
Conclusion
Fishbone in the liver is a rare condition. Ultrasound/ fluoroscopy-guided percutaneous drainage is an effective procedure for detecting the abscess source which nature is determinative for further management [5]. Moreover, a minimally invasive percutaneous drainage of liver abscess, conservatively treatment and careful follow-up are sufficient for favorable outcomes.
References
-
Zerem E, Hadzic A (2007) Sonographically guided percutaneous catheter drainage versus needle aspiration in the management of pyogenic liver abscess. AJR Am J Roentgenol 189(3): 138-142.
-
Branum GD, Tyson GS, Branum MA, Meyers WC (1990) Hepatic Abscess. Changes in Etiology, Diagnosis, and Management. Ann Surg 212(6): 655-662.
-
Lotfi M (1976) Foreign body in the liver. Int Surg 61(4): 228.
-
Mohammadi A, Khodabakhsh M (2009) Foreign body: A sewing needle migrating from the gastrointestinal tract to the liver. Iran J Radiol 6(4): 199-201.
-
Miłek T, Ciostek P (2019) Percutaneous Treatment of Liver Abscess-Outcomes. Prz Gastroenterol 14(2): 129- 132.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage