A Radiologist Approach to Acute Parenchymal Hemorrhages How to Intercept Shrouded Dragons
Primary intracranial hemorrhage (ICH) or hemorrhagic strokes etiology is unknown in the initial stage. The location, size and morphology are three important factors when reading the scan of intracranial hemorrhage. Clinical ICH score correlates with a 30 day mortality which takes into consideration admission Glasgow coma scale,>80 years old, ICH volume, infratentorial and presence of intraventricular hemorrhage. Management includes finding the cause of hemorrhage or symptomatic management.
Introduction
Acute intracranial bleeding can be due to a myriad of reasons [1]. Most of these are obvious and can be easily picked on imaging. Sometimes, however, it may be challenging to determine the precise reason for these bleeds on initial examination. In such cases, it is crucial to do a thorough workup of the patient so as not to miss any occult lesion [2, 3]. While intracranial hemorrhage prompts the surgeon to opt for immediate intervention, it is pertinent to find the cause of hemorrhage before running any intervention, as the hemorrhage could be associated with an underlying occult lesion. Blind mediation in such cases can have catastrophic results for the patient [4, 5].
In this abstract we’ll be highlighting seven different cases presenting with intracranial hemorrhage all with occult causes that resulted in bleeding. This abstract signifies the importance of detailed investigation/imaging to reveal the cause of bleed before proceeding towards any kind of intervention.
Hypertensive Hemorrhage
Round or oval hyperdense mass in basal ganglia (BG) or thalamus in patients with HTN [6].
Cerebral Amyloid Angiopathy
Normotensive demented patient with Lobar hemorrhage(s) of different ages.Multifocal cortical/ subcortical microhemorrhages “black dots” on T2* [7, 8].
Hemorrhagic Neoplasm
Metastases at grey white matter junction with disproportional oedema. Primary may be solid or cystic with rim enhancement and tiny vascular flow voids [9].
Drug Abuse
Young/middle-aged adult with ischemic or hemorrhagic stroke in close temporal proximity to drug administration [12].
Vascular Malformation
Popcorn appearance with complete hypointense hemosiderin rim on T2 MR [13]. Less common = thrombosed hemorrhagic arteriovenous malformation (AVM), dural arteriovenous fistula (dAVF) or middle cerebral artery (MCA) aneurysm. Look for stagnating vessels, early draining veins on DSA [14, 15].
In this review we’ll be highlighting different cases presenting with intracranial hemorrhage all with occult causes that resulted in bleeding. This signifies the importance of detailed investigation/imaging to reveal the cause of bleed before proceeding towards any kind of intervention.
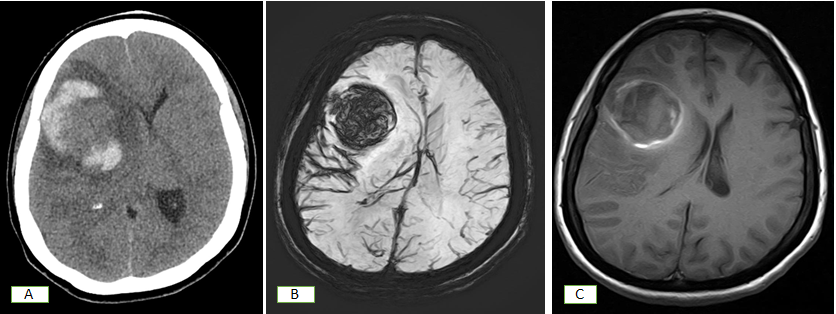
The first case is of a middle aged lady, who was a known case of hypertension, presented with left sided headache and right sided weakness. On initial MRI, she was diagnosed with a large intraparenchymal hematoma in the right frontal lobe. CT angiography done at that time did not show any aneurysm or AV malformation. Following this, she underwent digital subtraction angiography (DSA) which showed an abnormal blush with neovascularization in the right cerebral hemisphere, suspicious of tumor vascularity.
A few days later she presented with headache and periorbital pain with drop in GCS. She underwent CT head which revealed development of an acute intraparenchymal hemorrhage in interval on a background of previously resolving haematoma in right frontal lobe. The diagnosis of a possible intra-tumoral rebleed was made. The patient then underwent right frontotemporal craniotomy and debulking of tumor with clot evacuation. She was found (Figure 1) to have grade IV glioblastoma on histopathology.
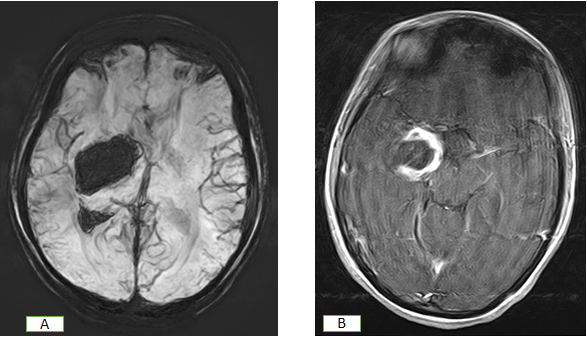
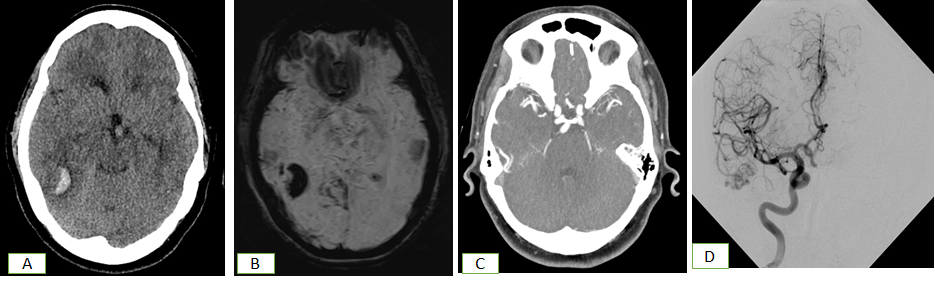
The second case is of a 24-year-old lady who presented with complaints of left-sided facial palsy and body weakness for three months with sudden onset left sided hemiparesis for one day. On brain MRI, she was found to have chronic/resolving right basal ganglia hemorrhage with intraventricular extension suspicious for an underlying neoplastic lesion. Subsequent DSA showed a hematoma, raising the possibility of an occult lesion with no intracranial aneurysm or AV malformation. Neuronavigation-guided right fronto-temporal craniotomy and debulking of lesion was carried out. On histopathology, the patient was found (Figure 2) to have grade I pilocytic astrocytoma.
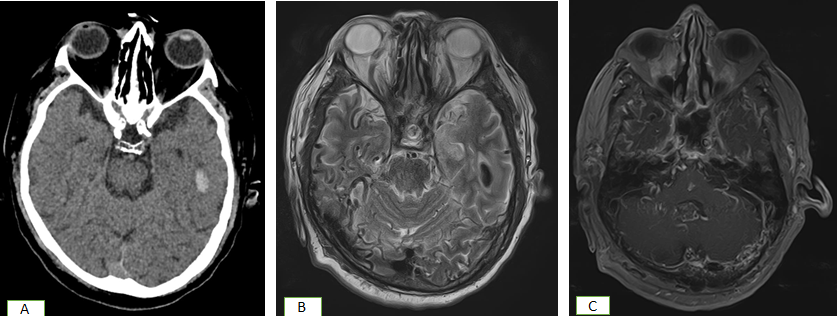
The third case is of a 72-year-old gentleman who presented to the ER with complaints of generalized tonic clonic fits and altered level of consciousness. He also gave a history of gait problems and dementia for the past four years. The patient underwent CT scan of the brain which showed left temporal lobe contusion with minimal surrounding subarachnoid hemorrhage. It also showed subtle gyral hyperdensity in the right parietal region and along the margins of the right lateral ventricle. On subsequent MRI, the patient was found to have irregularity along the transverse sinuses with multiple serpiginous flow voids in bilateral occipital regions, along the transverse sinuses and occipital bone. Findings were found (Figure 3) to be highly suspicious for dural arteriovenous fistula.
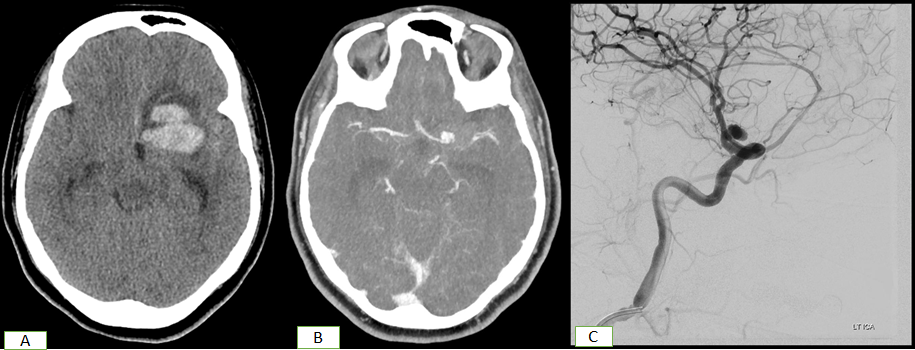
In the fourth case of this series, a 45-year-old lady presented with sudden onset drowsiness and acute loss of consciousness. Her CT brain showed left frontal intraparenchymal hemorrhage with intraventricular extension and subarachnoid hemorrhage. Her CT angiography showed (Figure 4) a narrow neck aneurysm at the bifurcation of the left internal carotid artery. On subsequent DSA, successful coiling of left ICA terminus aneurysm was performed with good aneurysm packing.
In the fifth case, a 46-year-old lady presented with complaints of seizures followed by drowsiness. Her initial workup was done with CT brain which showed a small right temporal lobe hemorrhage. She was also found to have diffuse cerebral oedema along with hydrocephalus. She then underwent an MRI brain which redemonstrated right temporal lobe hemorrhage. Marked intracranial atherosclerotic disease with ectasia was also seen.
Subsequent CTA revealed an abnormal bunch of vessels in the right posterior temporal lobe, representative of a small vascular malformation. Further imaging with DSA showed a pial AVM with nidus in the parietotemporal region supplied by feeders from the temporal branch of right MCA and posterior division of right middle meningeal artery, seen (Figure 5) draining into the confluence of sinuses via a single tortuous vein.
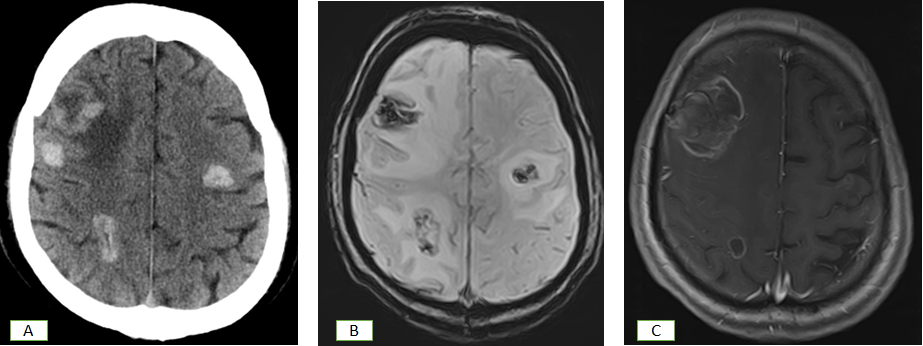
The sixth case is of a 56-year-old gentleman, who was a known case of small cell carcinoma of lung, presenting with focal seizures for three days. On CT brain performed at the time of presentation to the hospital, the patient was found to have multifocal peripherally enhancing lesions involving the grey-white matter junction of the brain likely representing metastasis. On subsequent MRI, hemorrhagic metastasis of varying sizes with significant perilesional oedema and some with central areas of necrosis were seen both in infratentorial and supratentorial areas. She was diagnosed (Figure 6) with small cell carcinoma with hemorrhagic metastasis to the brain.
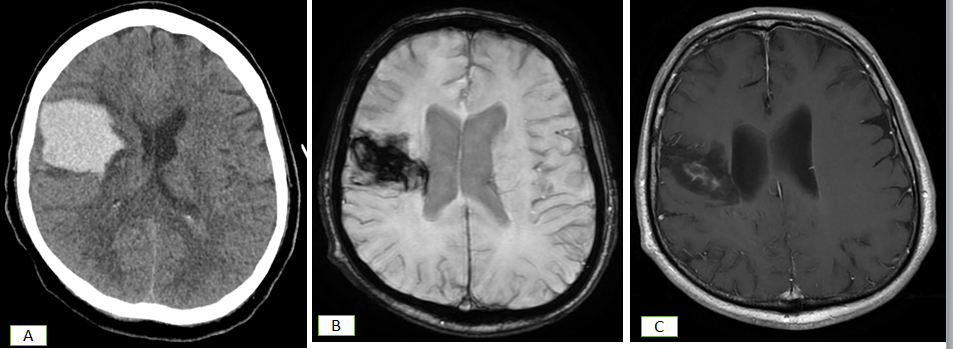
The final case in this case series is of a 56-year-old gentleman who presented with left sided weakness. On initial CT brain, right frontoparietal intraparenchymal bleed was seen causing mass effect and midline shift with intraventricular extension. On subsequent MRI, an abnormal signal intensity area was seen at the site of prior hemorrhage in the right frontal region. This showed dense internal hemosiderin staining and rim-like peripheral hemosiderin deposition. A scar-like area of enhancement was seen in the center of the previously mentioned abnormal signal intensity area. These findings were found (Figure 7) to be atypical for a bland hematoma with differential possibility of a Cerebral amyloid angiopathy.
Conclusion
In conclusion, we would once again like to highlight the importance of proper imaging with the appropriate imaging modality to reach the root cause of the bleed. Only then should we proceed for any kind of intervention. However, we have designed an action plan and protocol to be followed for proper evaluation:
- Screen = NECT in cases with HTN
- Atypical age or history = MR with T2*/SWI/T1 C+ or CTA
- If hyperacute ischemic “stroke” = MR with T2*/SWI and DWI
- If MR shows atypical hematoma=MRA or CTA
- If MRA or CTA inconclusive, go for DSA
References
-
Anderson E, Kryzanski J (2020) Prognosis and futility in neurosurgical emergencies: a review. Clin Neurol Neurosurg 195: 105851.
-
Furlan AB, Joshi KC, Vargas A, Chen M (2020) Endovascular management of symptomatic intracranial pseudoaneurysm and intimal flow-limiting dissection with a single device. World Neurosurg 141: 72.
-
Nawabi J, Elsayed S, Kniep H, Sporns P, Schlunk F, et al. (2020) Inter- and intrarater agreement of spot sign and noncontrast CT markers for early intracerebral hemorrhage expansion. J Clin Med 9(4): 1020.
-
Hoffman H, Jalal MS, Chin LS (2020) Prediction of mortality after evacuation of supratentorial intracerebral hemorrhage using NSQIP data. J Clin Neurosci 77: 148- 156.
-
Ironside N, Chen CJ, Mutasa S, Sim JL, Ding D, et al. (2020) Fully automated segmentation algorithm for perihematomal edema volumetry after spontaneous intracerebral hemorrhage. Stroke 51(3): 815-823.
-
Patel VD, Garcia RM, Swor DE, Liotta EM, Maas MB, et al. (2020) Natural history of infratentorial intracerebral hemorrhages: two subgroups with distinct presentations and outcomes. J Stroke Cerebrovasc Dis 29(8): 104920.
-
Sembolini A, Romoli M, Pannacci U, Gambaracci G, Floridi P, et al. (2020) Acute hematoma expansion after spontaneous intracerebral hemorrhage: risk factors and impact on long-term prognosis. Neurol Sci 41(9): 2503- 2509.
-
Miller TR, Shankar RS, Basha MM, Gandhi D (2015) Reversible cerebral vasoconstriction syndrome, part 1: epidemiology, pathogenesis, and clinical course. Am J Neuroradiol 36(8): 1392-1399.
-
Wu J, Liu Q, Wang K, Yang J, Jiang P, et al. (2021) Emergency surgery is an effective way to improve the outcome of severe spontaneous intracerebral hemorrhage patients on long-term oral antiplatelet therapy. Neurosurg Rev 44(2): 1205-1216.
-
Ng D, Churilov L, Mitcohell P, Dowling R, Yan B (2018) The CT swirl sign is associated with hematoma expansion in intracerebral hemorrhage. AJNR Am J Neuroradiol 39(2): 232-237.
-
Kumar NSS, Neeraja V, Raju CG, Padala RK, Kumar TK (2015) Multiple spontaneous hypertensive intracerebral hemorrhages. J Stroke Cerebrovasc Dis 24(1): 25-27.
-
Rammos SK, Gardenghi B, Bortolotti C, Cloft HJ, Lanzino G (2016) Aneurysms associated with brain arteriovenous malformations. AJNR Am J Neuroradiol 37(11): 1966- 1971.
-
Alexander MD, Cooke DL, Nelson J, Guo DE, Dowd CF, et al. (2015) Association between venous angioarchitectural features of sporadic brain arteriovenous malformations and intracranial hemorrhage. AJNR Am J Neuroradiol 36(5): 949-952.
-
Kranz PG, Amrhein TJ, Provenzale JM (2015) Spontaneous brain parenchymal hemorrhage: an approach to imaging for the emergency room radiologist. Emerg Radiol 22(1): 53-63.
-
Ciura VA, Romero JM (2014) Nontraumatic acute intraparenchymal hemorrhage: algorithm for workup and differential diagnosis. Semin Roentgenol 49(1): 112- 126.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage