Atypical Unilateral Sacral Stress Fracture in a Marathon Runner
Stress fractures are common overuse injuries in athletic population. They contribute to 15-20% of all cases in a sports medicine clinic. These injuries occurs when a normal bone is exposed to excessive, repetitive forces leading to altered bone homeostasis with predominant osteoclastic function with osseous breakdown leading to micro fractures in the bone which may progress to a frank fracture line in the setting of continued exposure.
Introduction
Sacral stress fractures (SSF) are rare injuries in athletes involved in sports like running, badminton, soccer, and volleyball; mostly being reported as isolated case reports in females [4, 5, 6, 7, 8]. It is still rarer in long distance runners especially in males, with only a few case reports available in published literature, so far [4, 7, 9, 10, 11, 12, 13, 14].
We present a case of a male long distance runner with a SSF managed as chronic lumbar strain before presenting to our clinic.
Case Report
A 23 year-old male athlete, presented with complaints of pain in the lower back and left buttock with stiffness in the post thigh for the past four months. Pain was insidious in onset and increased in intensity over the past 4 months. Symptoms initially worsened post-run extending to next morning, and more recently, since a month, the athlete started experiencing pain towards the end of the running session. He had stopped running for the past two weeks.
He is a long distance runner with an average weekly mileage of 120 kilometers. Prior to onset of symptoms there was no history of any increase in intensity, mileage, duration of running, change of surface or shoes. He had a history of bilateral shin pain three years ago for which no formal treatment was taken and had resolved (Figure 1) after he reduced running for 4 weeks.
On examination, there was left paramedian tenderness on sacrum and left sacroiliac joint. There was tightness in the left hamstrings with passive hip flexion. Spinal and hip range of motion were normal along with a normal neurological examination. Hop test reproduced the patient’s pain, more pronounced when hopping on left limb. There was no leg- length discrepancy or any foot misalignment.
His body mass index (BMI) was 22.2 kg/m2 with 23.2 percentage body fat. His energy availability (EA) was 36 kcal/kg FFM/day.
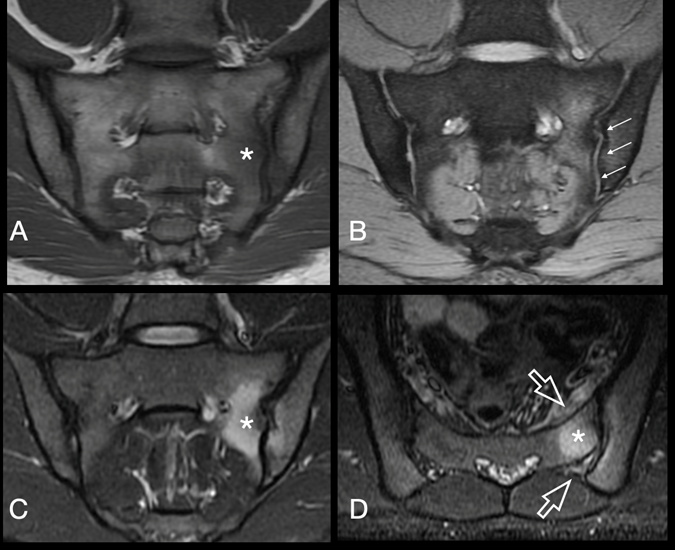
Figure 1: Coronal oblique T1 weighted MRI (A) shows ill-defined low signal at left subarticular sacral marrow (*). Corresponding GRE image (B) exhibits smooth cortical outline ( multiple white arrows) at the left sacro-iliac joint with absence of significant joint effusion on coronal oblique fat supressed proton density image (C) ruling out the possibility of inflammatory or infective pathology. Axial STIR images (D) show mildly edematous pre-sacral and post-sacral soft tissue edema (open arrows).
Plain radiographs of lumbar spine and pelvis were unremarkable. Magnetic resonance imaging (MRI) revealed marrow edema at left paramedian sacrum with a well-defined transverse fracture line at S2 level. Both sacro-iliac joints had smooth, congruent articular margins with no erosions or significant effusion, making the possibility of inflammatory or infective etiology less likely. Bone mineral density (BMD) was 1.364 gm/cm2 with a Z-score of 2.5 & T-score of 1.8. His complete blood count, kidney function test, serum calcium, HLA B27 and urine routine and microscopic examination were normal. Serum vitamin D level was 28 ng/ml.
The athlete was put on a staged rehabilitation program, which started with partial weight-bearing on elbow crutches for three weeks. When the athlete was pain free during activities of daily living for 5 days, he was put on a static strengthening program focusing on core and pelvic musculature. Next, non-impact aerobic activities like cycling and swimming were started. Return to running program was initiated at 8 weeks, starting with pool running and progressing on to treadmill. Treadmill running was preferred as the speed and duration of the run could be better controlled. Lumbo-pelvic stabilization exercises remained a mainstay of rehab program. Return to athlete’s previous level was achieved at 22 weeks after the first presentation. Calcium (2000mg/day) and vitamin D (2000IU/day) supplementation with increased caloric intake was given throughout the treatment period.
Discussion
SSF are uncommon sports injuries, with unknown prevalence [15]. Volpin et al first reported SSF in three military recruits with sacral wing stress injuries [16]. They usually present as insidious onset of low back and buttock pain towards the end of the workout [4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14]. There is usually a delay in diagnosis, as SSFs are uncommon and hence not usually in the top differential. The vague, non-specific low back ache worsening with activity is often misdiagnosed as lumbar strain, disc disease, tendinopathies or sacroiliitis due to overlapping symptomatology. SSF are usually diagnosed on MRI, which is done due to non-responsive treatment aimed at other pathologies as mentioned before [7, 9, 11].
Sacrum is the keystone of the pelvis. SSF occurs as excessive, repetitive forces in the vertebral column get dissipated and concentrated in the sacrum and sacral ala, thereby altering the bone homeostasis. As a result, osteoclastic functions predominates leading to osseous breakdown, micro fracture and eventually a frank fracture line [17].
There is paramedian tenderness on either side of sacrum on examination, or unilateral on the affected side as in our case. Leg length discrepancy has been attributed to unilateral SSF with the longer limb being more affected [14]. Tests for lumbar spine and sacro-iliac joints like hop test, Faber, crossed straight leg raise should be performed [7, 11].
Majority of reported SSFs have been in females who, in general, are at increased risk of stress fractures due to low energy availability (LEA), menstrual dysfunction and low bone mineral density (female athlete triad) [18].
Related to female athlete triad is the relative energy deficiency in sports syndrome (RED-S syndrome). In addition to female athletes, the RED-S model proposes that male athletes, non-Caucasian athletes and athletes with disability may also experience low energy availability and its subsequent adverse health (including bone health) and performance (including risk of musculoskeletal injuries) consequences [19].
The health effects of LEA in men are less established than in women. The RED-S model proposes shared consequences of LEA, though LEA could affect different systems in men than in women and there is not yet a proposed threshold of LEA for men [20].
LEA has been reported as major cause of bone stress injuries. Koehler reported LEA in 56% males & 51% females among young athletes [21]. Heikura et al reported LEA in 25% of male and 31% of female middle and long distance elite athletes but was poorly correlated with factors known to be affected by LEA, including reproductive, metabolic and bone health [22].
Male runners with low BMI (<85% body weight) due to the belief that being thinner leads to faster running performances, running greater than 30 miles (48 km) per week and history of stress fracture are at an elevated risk for impaired skeletal health [23, 24]. Our patient used to run 120 km/Week, had previous history of stress injury and had normal BMI, BMD with subclinical LEA, probably contributing to the stress fracture.
Nutritional and metabolic assessment consisting of calculation of BMI, EA, dietary intake of calcium and vitamin D should be assessed. Blood parameters like complete blood count, kidney function test, serum calcium, vitamin D levels should be done.
Calcium provides strength to the bone through a mineralized matrix while vitamin D helps in the absorption of dietary calcium. Ruohola et al have found an association between vitamin D insufficiency and occurrence of stress fractures [25]. Tenforde et al suggested a daily intake of 1500 mg calcium may reduce the incidence of stress injuries [26]. Our patient had marginal deficiency of vitamin D.
Radiographic evaluation should begin with plain radiographs of lumbar spine and pelvis, although sensitivity to reveal SSF is low [4, 5, 11]. MRI is the gold standard for diagnosing SSF. MRI have a high sensitivity and specificity to detect bone marrow and cortical bone edema [7, 9, 11]. Typical MRI appearance includes periosteal or adjacent soft- tissue edema, band-like bone marrow edema, and T1 hypo intense fracture line. Bone scans are highly sensitive but are associated with the risks of ionizing radiations and SI joint dysfunction, sacroiliitis, and malignancy may produce similar picture [12].
SSF can be managed conservatively with a staged rehabilitation program with rest, activity modification, dietary modification and gradual return to activity. A team approach with sports nutritionist, psychologist and physiotherapist should be employed as the course of treatment can be long and frustrating for both the treating physician and the athlete.
This case is unique as sacral SSF have rarely been reported in male runners and none of such reports has assessed patients on basis of energy availability or BMI while only rarely such cases have been evaluated for BMD [4, 11] and Vitamin D level estimation [7, 11].
Considering the non-specific symptoms and rare presentation, physicians must have a high index of suspicion for SSF even in male long distance runners. Assessment should include EA, MRI, BMI, BMD, serum calcium and vitamin D estimation and appropriate correction.
References
-
Fredericson M, Jennings F, Beaulieu C, Matheson GO (2006) Stress fractures in athletes. Top Magn Reson Imaging 17(5): 309-325.
-
Hosey RG, Fernandez MM, Johnson DL (2008) Evaluation and management of stress fractures of the pelvis and sacrum. Orthopedics 31(4): 383-385.
-
Nalla RK, Kinney JH, Ritchie RO (2003) Letters: mechanistic fracture criteria for the failure of human cortical bone. Nat Mater 2(3): 164-168.
-
Fredericson M, Salamancha L, Beaulieu C (2003) Sacral stress fractures: tracking down nonspecific pain in distance runners. Phys Sport Med 31(2): 31-42.
-
Johnson AW, Weiss CB, Stento K, Wheeler DL (2001) Stress fractures of the sacrum: an atypical cause of low back pain in the female athlete. Am J Sport Med 29(4): 498-508.
-
Shah MK, Stewart GW (2002) Sacral stress fractures, an unusual cause of low back pain in an athlete. Spine 27(4): 104-108.
-
Vajapey S, Matic G, Hartz C, Miller TL (2019) Sacral Stress Fractures: A Rare but Curable Cause of Back Pain in Athletes. Sports Health 11(5): 446-452.
-
Yuasa Y, Miyakoshi N, Hongo M, Ebata K, Tomioka T, et al. (2017) Sacral stress fracture in an amateur badminton player. Case Rep Orthop 2017: 4268981.
-
Major NM, Helms CA (2000) Sacral stress fractures in long-distance runners. Am J Roentgenol 174(3): 727- 729.
-
McFarland EG, Giangarra C (1996) Sacral stress fractures in patients. Clin Orthop Relat Res 329: 240-243.
-
Kahanov L, Eberman L, Alvey T, True J, Yeargin B (2011) Sacral stress fracture in a distance runner. Journal of the American Osteopathic Association 111(10): 585-591.
-
Alsobrook J, Simons SM (2007) Sacral stress fracture in a marathon runner. Curr Sports Med Rep 6(1): 39-42.
-
Delvaux K, Lysens R (2001) Lumbosacral pain in an athlete. Am J Phys Med Rehabil 80(5): 388-391.
-
Eller DJ, Katz DS, Bergman AG, Fredericson M, Beaulieu CF (1997) Sacral stress fractures in long-distance runners. Clin J Sport Med 7(3): 222-225.
-
Bono CM (2004) Low-back pain in athletes. J Bone Joint Surg Am 86(2): 382-396.
-
Volpin G, Milgrom C, Goldsher D, Stein H (1989) Stress fractures of the sacrum following strenuous activity. Clin Orthop Relat Res 243: 184- 188.
-
Boden BP, Osbahr DC, Jimenez C (2001) Low-risk stress fractures. Am J Sports Med 29(1):100–111.
-
Barrack MT, Gibbs JC, Williams NI, Nichols JF, Rauh MJ, et al. (2014) Higher incidence of bone stress injuries with increasing female athlete triad-related risk factors: a prospective multisite study of exercising girls and women. Am J Sports Med 42(4): 949-958.
-
Mountjoy M, Burke L, Carter S, Constantini N, Lebrun C, et al. (2014) The IOC consensus statement: beyond the Female Athlete Triad-Relative Energy Deficiency in Sport (RED-S). Br J Sports Med 48(7): 491-497.
-
Burke LM, Close GL, Lundy B, Mooses M, Morton JP, et al. (2018) Relative Energy Deficiency in Sport in Male Athletes: A Commentary on Its Presentation Among Selected Groups of Male Athletes. Int J Sport Nutr Exerc Metab 28(4): 364-374.
-
Koehler K, Achtzehn S, Braun H, Mester J, Schaenzer W (2013) Comparison of self-reported energy availability and metabolic hormones to assess adequacy of dietary energy intake in young elite athletes. Appl Physiol Nutr Metab 38(7): 725-733.
-
Heikura IA, Uusitalo ALT, Stellingwerff T, Bergland D, Mero AA, et al. (2018) Low energy availability is difficult to assess but outcomes have large impact on bone injury rates in elite distance athletes. International Journal of Sport Nutrition and Exercise Metabolism 28(4): 403- 411.
-
Barrack MT, Fredericson M, Tenforde AS, Nattiv A (2017) Evidence of a cumulative effect for risk factors predicting low bone mass among male adolescent athletes. Br J Sports Med 51(3): 200-205.
-
Tenforde AS, Fredericson M, Sayres LC, Cutti P, Sainani KL (2015) Identifying sex-specific risk factors for low bone mineral density in adolescent runners. The American Journal of Sports Medicine 43(6): 1494-1504.
-
Ruohola JP, Laaksi I, Ylikomi T, Haataja R, Mattila VM, et al. (2006) Association between serum 25(OH) D concentrations and bone stress fractures in Finnish young men. J Bone Miner Res 21(9):1483-1488.
-
Tenforde AS, Sayres LC, Sainani KL, Fredericson M (2010) Evaluating the relationship of calcium and vitamin D in the prevention of stress fracture injuries in the young athlete: a review of the literature. PM & R 2(10): 945- 949.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage