Tuberous Sclerosis with Typical Neuroimaging Findings-A Case Report
Tuberous sclerosis (TS) is an autosomal dominant disorder, also known as Bourneville-Pringle disease. The disease is classically characterized by the presence of hamartomatous growths in multiple organs. TS and tuberous sclerosis complex (TSC) are different terms for the same genetic condition. The major sign and symptoms include, central nervous system manifestations including epilepsy, cognitive impairment and autism spectrum disorders, cutaneous, cardiac, renal and ophthalmic manifestations with Epilepsy being the most common symptoms and affects 70% - 90% of patients.
Introduction
The prevalence of TS is reported to be approximately 1:6000 - 10,000 live births [1]. TSC is caused by mutations on either of two genes, TSC1 and TSC2, which encode for the proteins hamartin and tuberin respectively. Desire-Magloire Bourneville first described the disease in 1880, when post-mortem examination of 15 year old girl patient with psychomotor retardation, epilepsy and a “confluent vascular-papulous eruption of the nose, the cheeks and forehead, disclosed hard, dense tubers in the cerebral convolutions, which Bourneville named Sclerose tubereuse des circonvolutions cerebrales [2, 3, 4]. The term tuberous describes the potato-like consistency of gyri with hypertrophic sclerosis A four and half year-old female child was referred to the radiology department for brain MRI with a provisional diagnosis of TS. The physical examination revealed multiple skin lesions consistent with angiofibromas (Figure 1A) on the face, hypopigmented skin lesions (ash leaf spot) (Figure 1B) on chest wall. there was history of seizures since child was 6-month-old. The patient has normal cognitive function and same was confirmed during our interaction with patient prior to imaging. There was no extended family history of this type of dermatological or seizure disorder. Pre-natal and post-natal periods were uneventful according to the mother. He had no delayed milestones.

Figures 1A-B: Figure 1A show multiple tiny dome-shaped papules in the face representing Facial angiofibromas. Figure 1B show hypopigmented macules represent ash leaf spots (arrows).
Figures 2A-D: Axial FLAIR MR image shows heterogeneously enhancing hyperintense lesions consistent with SEGA (wide arrow in image 2 A-C) in B/L frontal horn of lateral ventricle at the level of the foramen of Monro. Axial contrast enhanced T1- weighted MR image shows enhancement of the subependymal nodules (Thin arrow in 2D).
Figures 3A-D: Axial FLAIR and T2WI MR Image showing multiple hyperintense lesions (arrows) in the cortex in B/L cerebral parenchyma, consistent with cortical tubers.
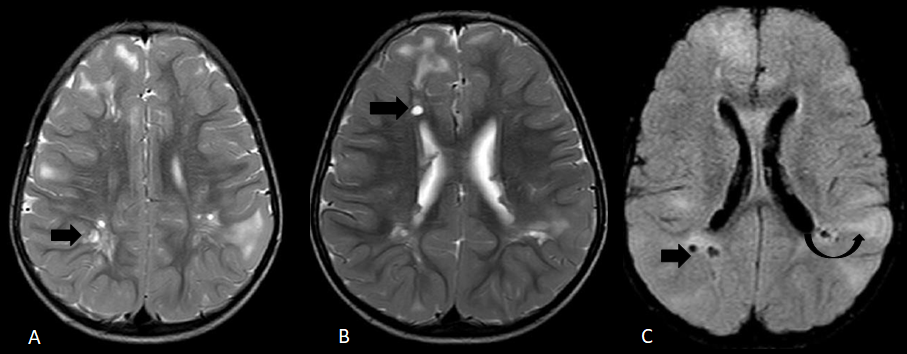
Figures 4A-C: Axial T2-weighted and Axial fluid-attenuation inversion-recovery MR images show a well- demarcated cystic white matter lesions (Wide arrows in 4 A-C) in white matter, isointense to cerebrospinal fluid. Axial fluid-attenuation inversion- recovery MR image demonstrates linear radial white matter bands extending from the cortex to the lateral ventricles (curved arrow in 4C).
After relevant laboratory investigations and normal renal function test, contrast enhanced MRI brain was done which showed, two heterogeneously enhancing subependymal masses approaching foramen of Monro representing subependymal giant cell astrocytomas (Figures 2 A-C). No associated obstructive hydrocephalus seen. Focal thickenings/nodules representing subependymal nodules were seen along the subependymal region of the body of the lateral ventricles (Figure 2D). There were multiple areas of T2 and FLAIR hyperintensities in the cortex, consistent with cortical tubers (Figures 3 A-D). Few small well-demarcated lesions of cerebrospinal fluid signal on all sequences were seen in white matter in periventricular location (Figures 4 A-C) radial white matter bands were also seen (Figure 4C).
Discussion
TS is associated with variety of intracranial manifestations with most common CNS abnormalities include Cortical Tubers, Subependymal Nodules (SEN), Subependymal Giant Cell Astrocytomas (SGCAs), and white matter abnormalities. Except for SGCAs, these abnormalities can be seen in almost all patients with TS. The estimated prevalence of cortical tuber and subependymal nodule is 95%-100% and that of white matter abnormalities is 40%–90% [5]. Tubers are often epileptogenic [6]. They vary widely in size, location, and appearance [7], but in contrast to SENs, tubers are thought to remain stable in size over time. Calcification of SENs is frequent (93%) in patients with TSC, especially after 18 months of age, and increase in size with time in 35% of patients. Calcification in tubers has been reported in 43 to 62% of patients and prevalence increases with age [7, 8, 9]. Other CNS abnormalities are radial white matter bands, and cyst like white matter lesions. The reported frequency of radial white matter abnormalities 15%–27% and of cyst like lesions is 15%-44% [10].
Conclusion
TS is a neurocutaneous syndrome with clinical history of seizures and cutaneous lesions, imaging plays an important role in diagnosis. The present case highlights the typical neuroradiological findings in TS.
References
-
Leung AKC, Robson WLM (2007) Tuberous sclerosis complex: a review. J Pediatr Health Care 21(2): 108-114.
-
Jansen FE, Nieuwenhuizen OV, Huffelen ACV (2004) Tuberous sclerosis complex and its founders. J Neurol Neurosurg Psychiatry 75(5): 770.
-
Virchow R (1994) Die Krankhaften Geschwülste, Vol II. Berlin: August Hirschwald pp: 148.
-
Wilkins RH, Brody IA (1997) XXXI Tuberous Sclerosis. In: Wilkins RH, et al. (Eds.), Neurological Classics. American Association of Neurological Surgeons, pp: 149-152.
-
Tassel PV, Cure JK, Holden KR (1997) Cystlike white matter lesions in tuberous sclerosis. AJNR Am J Neuroradiol 18(7): 1367-1373.
-
Crino PB, Nathanson KL, Henske EP (2006) The tuberous sclerosis complex. N Engl J Med 355(13): 1345-1356.
-
Gallagher A, Grant EP, Madan N, Jarett DY, Lyczkowski DA, et al. (2010) MRI findings reveal three different types of tuber in patients with tuberous sclerosis complex. J Neurol 257(8): 1373-1381.
-
Martin N, Broucker TD, Cambier J, Marsault C, Nahum H (1987) MRI evaluation of tuberous sclerosis. Neuroradiology 29(5): 437-443.
-
Koh S, Jayakar P, Dunoyer C, Whiting SE, Resnick TJ, et al. (2000) Epilepsy surgery in children with tuberous sclerosis complex: presurgical evaluation and outcome. Epilepsia 41: 1206-1213.
-
Shepherd CW, Houser OW, Gomez MR (1995) MR findings in tuberous sclerosis complex and correlation with seizure development and mental impairment. AJNR Am J Neuroradiol 16(1): 149-155.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage