Diagnostic Challenges in a Patient with Metastatic Merkel Cell Carcinoma and Abdominal Pain
We examined a 51-year-old white male patient diagnosed with metastatic Merkel cell tumor, treated with immunotherapy, who came to the emergency room with upper abdominal pain and elevated pancreatic serum enzymes. He was suspected to have acute pancreatitis and was referred for computed tomography examination, which didn’t depict any sign of acute pancreatitis, showing a solid mass adjacent to the pancreatic head, retroperitoneal lymphadenopathies, solid nodules in the subcutaneous fat, and retroperitoneum.
Introduction
Merkel cell carcinoma (MCC) is a rare epidermal malignant tumor that appears on the sun-exposed tegument of the head and neck in old patients and is considered to be a neuroendocrine tumor derived from the Merkel cells [1, 2]. This is an aggressive lesion that causes regional lymphadenopathies and metastases in subcutaneous fat, the liver, bones, brain, and lungs [3, 4], which are all grouped under stage IV [4, 5]. The impact of the M1a to M1c categories on prognosis is not certain. M1a disease is metastasis to distant skin, subcutaneous tissue, or lymph nodes. M1b represents metastasis to the lungs, and M1c to all other visceral sites [6, 7].
MCC doesn’t have a durable response to chemotherapy, so immunotherapy became the first-choice drug for treating metastatic MCC [6]. This is a human monoclonal antibody that causes several serious adverse reactions like pneumonitis, hepatitis, colitis, pancreatitis, endocrinopathies, and some undesirable effects like fatigue, nausea, diarrhea, and abdominal pain [8, 9].
We examined a 51-year-old white male patient diagnosed with metastatic Merkel cell tumor; the primary tumor was located on the antero-inferior part of the neck and was surgically resected, but at the time he already had metastases, so he began immunotherapy (2 cures of checkpoint inhibitors - Avelumab); the patient came to the emergency room with upper abdominal pain and elevated LDH (911 U/L) and pancreatic enzymes (serum amylase = 330 U/L, serum lipase = 517 U/L). He was suspected to have acute pancreatitis and was referred for abdominal ultrasound and computed tomography examinations.
Abdominal ultrasound revealed lobulated, inhomogeneous, confluent hypoechoic masses in the pancreatic head and a mildly dilated main pancreatic duct;
there was no retroperitoneal or intraperitoneal fluid. We performed contrast-enhanced abdomino-pelvic MDCT, with a noncontrast-enhanced phase, intravenous injection of iodinated contrast medium (1 ml/kg, 3 ml/s), followed by arterial and portal venous phases, and we found the following lesions:
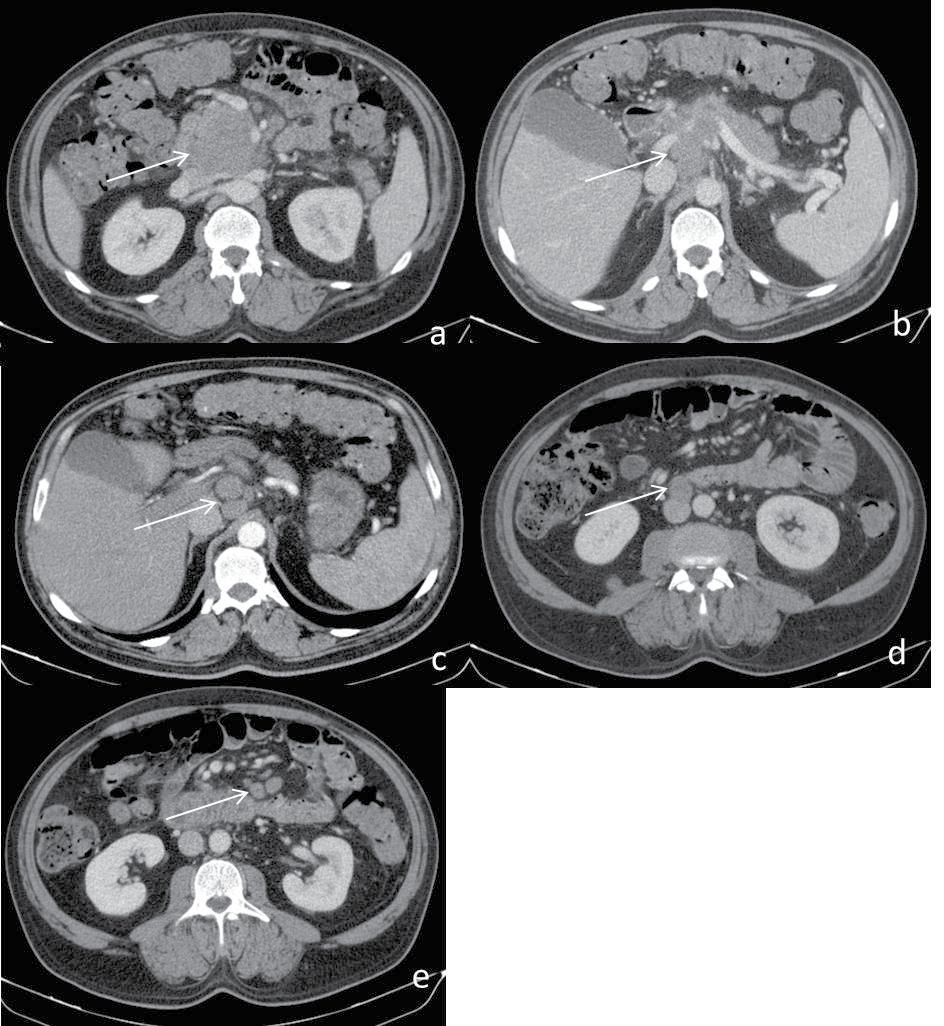
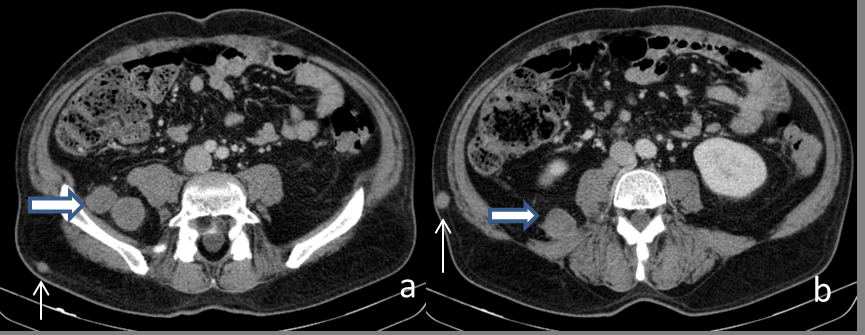
• Large, solid, slightly enhancing, well-defined, lobulated mass nearby the pancreatic head, which compresses pancreatic parenchyma, portal, and splenic veins; pancreatic body and tail with normal dimensions and structure, with mildly dilated main pancreatic duct (4 mm) (Figure 1). • lymphadenopathies all over the retroperitoneum (interaortocaval, precaval, mesenteric root, nearby internal and external iliac vessels) but also in the inguinal region, retrocrural, and paravertebral (Figure 1). • hyperdense, slightly enhancing round nodules localized subcutaneously on the abdominal wall and in the posterior pararenal space (Figure 2). • no focal lesions in the liver, adrenals, spleen, or kidneys; • no retroperitoneal or intraperitoneal fluid.
Discussion
The 51-year-old construction worker with MCC we examined is a particular case because:
He is middle-aged (the literature reports this malignant skin tumor in older patients) [1]; He had an acute development after immunotherapy, consisting of upper abdominal pain (which frequently appears after this treatment), associated with elevated pancreatic enzymes.
Abdominal ultrasound was inconclusive for the suspicion of acute pancreatitis and revealed instead hypoechoic lesions in the pancreatic head.
The MDCT examination didn’t depict any sign of acute pancreatitis and showed a solid mass adjacent to the pancreatic head, retroperitoneal lymphadenopathies, solid nodules in the subcutaneous fat, and right posterior pararenal space (which were suspected to be secondary lesions), but no liver or bone metastases; the solid nodules in the subcutaneous fat and pararenal space enhanced mildly, although in the literature the metastases from Merkel cell carcinoma are known to have intense uptake of contrast medium.
Merkel cell tumors frequently cause regional lymphadenopathies; instead, our patient has retroperitoneal and inguinal lymph node involvement [7].
The metastatic lesions cited in the literature are in subcutaneous fat, liver, bones, brain, and lungs, but in this case the secondary lesions were located in subcutaneous fat and in the pararenal fat without other secondary lesions in the organs (M1a) [10].
An elevated level of LDH indicates tissue damage, which has multiple causes and can appear not only in pancreatitis but also in cases of metastatic malignant tumors. Studies show a link between tumor lactate concentration and the frequency of metastasis in head and neck cancer, and a high level of lactate production has been recognized as the hallmark of cancer [11, 12].
The main diagnosis problem was the mass nearby the pancreatic head, which raised several differential diagnosis problems: • Pancreatic cancer is a solid lesion, slightly hipodense on noncontrast enhanced and postcontrast scans, with poorly defined margins, invading the peripancreatic fat, peripancreatic vessels, and adjacent organs [13]; • neuroendocrine pancreatic tumor: on MDCT the lesion has intense contrast enhancement; • Focal autoimmune pancreatitis is a mass with homogenous enhancement, which determines a smooth narrowing of the Wirsung duct and a mild dilatation upstream [13]. • Mass-forming chronic pancreatitis is a hypoattenuating mass (noncontrast enhanced CT) and hypovascular on contrast-enhanced scans, with well-defined margins, often located in the pancreatic head [14]. • Paraduodenal pancreatitis (groove pancreatitis) is a form of chronic pancreatitis that appears in the groove between the pancreatic head and duodenum, sometimes involving the pancreatic head, and usually does not encase the gastroduodenal artery or the biliary duct [15]. • Peripancreatic lymphadenopathies are lobulated, well- defined masses that compress the elements around them but do not invade them, and have mild contrast enhancement.
We concluded that the lesion adjacent the pancreatic head was in fact represented by lymphadenopathies, based on their appearance (well-defined, lobulated mass), lack of pancreatic and vessel invasion, and mild uptake of contrast medium.
Acute pancreatitis induced by immunotherapy is rarely reported (less than 1%), and MDCT examination can establish the diagnosis of acute pancreatitis but is not specific for autoimmune pancreatitis, and we could not correlate this diagnosis with checkpoint inhibitors treatment (there are no typical lesions of acute pancreatitis on MDCT). The elevated pancreatic enzymes could appear as a pancreatic reaction to any other digestive diseases or even with the treatment.
Conclusion
We examined a patient with metastatic Merkel cell carcinoma, treated with immunotherapy, who came with upper abdominal pain and elevated LDH and pancreatic enzymes. The suspected diagnosis was acute pancreatitis, but abdominal ultrasound and computed tomography did not confirm the diagnosis, finding instead secondary lesions in the subcutaneous and retroperitoneal fat and abdominal (including peripancreatic head) and pelvic lymphadenopathies. The throwback of our statement is that we did not have any pathological confirmation for the metastases or lymphadenopathies, but in the case of this patient with Merkel cell carcinoma and no other malignancies, this was the only logical conclusion.
References
-
Ramahi E, Choi J, Fuller CD, Eng TY (2013) Merkel Cell Carcinoma. Am J Clin Oncol 36(3): 299-309.
-
Poulsen M (2005) Merkel Cell Carcinoma of Skin: Diagnosis and management strategies. Drugs Aging 22(3): 219-229.
-
Eichorn FC, Dubey A, Pathak KA (2023) Merkel Cell Carcinoma of the Head and Neck. Plast Surg (Oakv) 31(2): 146-150.
-
Tetzlaff MT, Nagarajan P (2018) Update on Merkel Cell Carcinoma. Head Neck Pathol 12(1): 31-43.
-
Senchenkov A, Moran SL (2013) Merkel Cell Carcinoma: Diagnosis, management, and outcomes. Plast Reconstr Surg 131(5): 771-778.
-
Mehrany K, Otley CC, Weenig RH, Phillips PK, Roenigk RK, et al. (2002) A Meta-analysis of the Prognostic Significance of Sentinel Lymph Node Status in Merkel Cell Carcinoma. Dermatol Surg 28(2): 113-117.
-
Yusuf MB, McKenzie G, Rattani A, Tennant P, Bumpous J, et al. (2021) Merkel Cell Carcinoma of the Head and Neck: Epidemiology, Pathogenesis, Current State of Treatment and Future Directions. Cancers (Basel) 13(14): 3506.
-
D’Angelo SP, Russell J, Lebbe C, Chmielowski B, Gambichler T, et al. (2018) Efficacy and Safety of First- line Avelumab Treatment in Patients with Stage IV Metastatic Merkel Cell Carcinoma: A Preplanned Interim Analysis of a Clinical Trial. JAMA Oncol 4(9): e180077.
-
Zhao B, Gao M, Zhao H, Zhao J, Shen X (2021) Efficacy and safety profile of Avelumab monotherapy. Crit Rev Oncol Hematol 166: 103464.
-
Gaiser MR, Bongiorno M, Brownell I (2018) PD-L1 inhibition with avelumab for metastatic Merkel cell carcinoma. Expert Rev Clin Pharmacol 11(4): 345-359.
-
Shirley M (2018) Avelumab: A Review in Metastatic Merkel Cell Carcinoma. Target Oncol 13(3): 409-416.
-
Xu HN, Kadlececk S, Profka H, Glickson JD, Rizi R, et al. (2014) Is Higher Lactate an Indicator of Tumor Metastatic Risk? A Pilot MRS Study Using Hyperpolarized (13)C-Pyruvate. Acad Radiol 21(2): 223-231.
-
Chang WI, Kim BJ, Lee JK, Kang P, Lee KH, et al. (2009) The clinical and radiological characteristics of focal mass- forming autoimmune pancreatitis: comparison with chronic pancreatitis and pancreatic cancer. Pancreas 38(4): 401-408.
-
Srisajjakul S, Prapaisilp P, Bangchokdee S (2020) CT and MR features that can help to differentiate between focal chronic pancreatitis and pancreatic cancer. Radiol Med 125(4): 356-364.
-
Triantopoulou C, Dervenis C, Giannakou N, Papailiou J, Prassopoulos P (2009) Groove pancreatitis: a diagnostic challenge. Eur Radiol 19(7): 1736-1743.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage