Impaction of Primary Molars in Indian Children – A Retrospective Radiographic Study and Upgraded New Classification System
Aim: To evaluate the prevalence of impacted primary molars including both first and second molars in children of Indian ethnicity. Materials and Methods: The present study included children with age ranging from 3 to 15 years who reported to Dental Outpatient wing, Karnataka ENT Hospital and Research centre, Chitradurga, Karnataka, India for their dental problems during the period from 2020 to 2022. Orthopantomograph radiographs of children were investigated for the prevalence, unilateral or bilateral occurrence and ratio between two genders found with impacted primary mandibular molars were recorded and the data obtained was subjected to statistical analysis using descriptive statistics. Results: The present study recorded a total of five cases of impacted primary mandibular molars among Indian children. In one case, first primary molar was involved (20%) and remaining four cases were associated with second molars (80%). No bilateral occurrences of impaction were observed. Four cases occurred on the left side (80%) and one on the right side (20%). Three cases were noticed in males (60%) and remaining two cases in girls (40%). Regarding the level of the impaction, two cases were classified as extremely severe (Type III) (40%), two as severe (Type II) (40%), and one as moderate (Type I) (20%). Pertaining to treatment, none of the cases received treatment. When assessing the condition of the succedaneous premolars, two patients exhibited distal drifting of the second premolar tooth bud towards the second primary molar. In one case malformed second premolar was erupted clinically and in another case odontoma formation was noticed, and in one case, second premolar was erupted buccally. Conclusion: Occurrence of ankylosed and impacted primary molars does exist and hence all clinicians should be aware of its occurrence as treatment of this condition requires early diagnosis followed by meticulous management including a multidisplinary approach. More research including large number of epidemiological studies are highly warranted on this domain to formulate new diagnostic and therapeutic guidelines.
Introduction
Any disturbances in the process of tooth eruption can give rise to eruptive disturbances which includes tooth impaction, ectopic eruption and delayed eruption. Compared to permanent teeth incidence of primary tooth impaction and eruption failure is extremely rare as evident from the dental literature [1, 2, 3]. A tooth impaction is defined as any tooth that fails to erupt into a normal functional position and remains unerupted in the jaw beyond the time when it should normally erupt [4]. In primary dentition the most commonly observable tooth with impaction is the second primary molars followed by central incisors. There is no exact true etiology behind the occurrence of this condition, however, it is been speculated that trauma is the most frequent cause damaging either the dental follicle or the developing periodontal ligament [5, 6, 7, 8].
Impaction of the primary tooth results in displacement of the succedaneous permanent tooth and in turn disturbs the growth of the permanent dental arch, root resorption of permanent teeth, cyst formation and malocclusion [4, 5, 6, 7, 8]. In addition to these, other clinical consequences seen with impacted primary molars are hooked roots or impaction of permanent successors, loss of arch length, alveolar bone defects, and occlusal disturbances [3]. Therefore, it is highly essential for the detection and treatment of impacted primary teeth as early as possible. As pediatric dentist is the first person to see children from one year of their life, it is necessary to detect the impaction of the primary molars during primary dentition stage in order to prevent disturbed complete and sound eruption of permanent dentition and also to avoid treatment complications.
Literature shows scanty countable numbers of publications on impacted primary molars [8, 9, 10, 11]. There is no exact data on the prevalence of its occurrence in the general population. Therefore, the present study was undertaken to evaluate the total prevalence of primary mandibular molars impaction including both first and second molars in Indian population. In addition to this, author has suggested a new classification system to classify the level of impaction seen in primary mandibular molars including both first and second molars which is explained in detail along with reference to the particular figures showing the different level of impaction (Table 1).
| Type | Level of Impaction | Description |
|---|---|---|
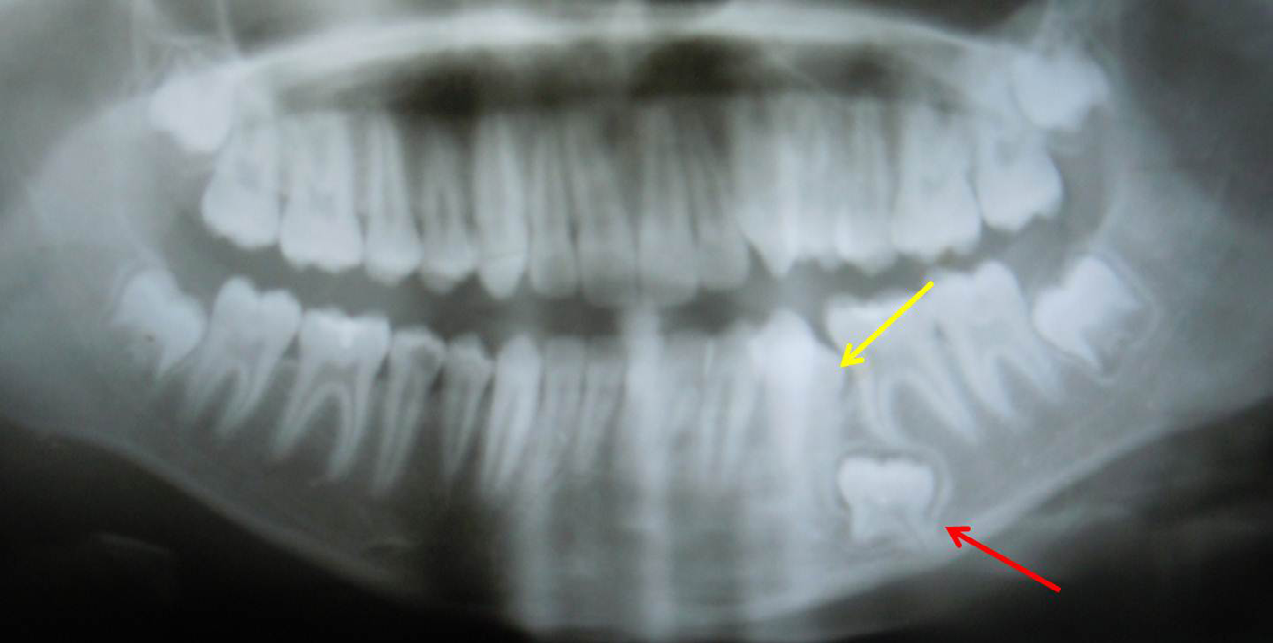
| Type I | Moderate (Figure 3) | Impacted primary molar placed below the level of cervical third of adjacent erupted teeth within the alveolar bone |
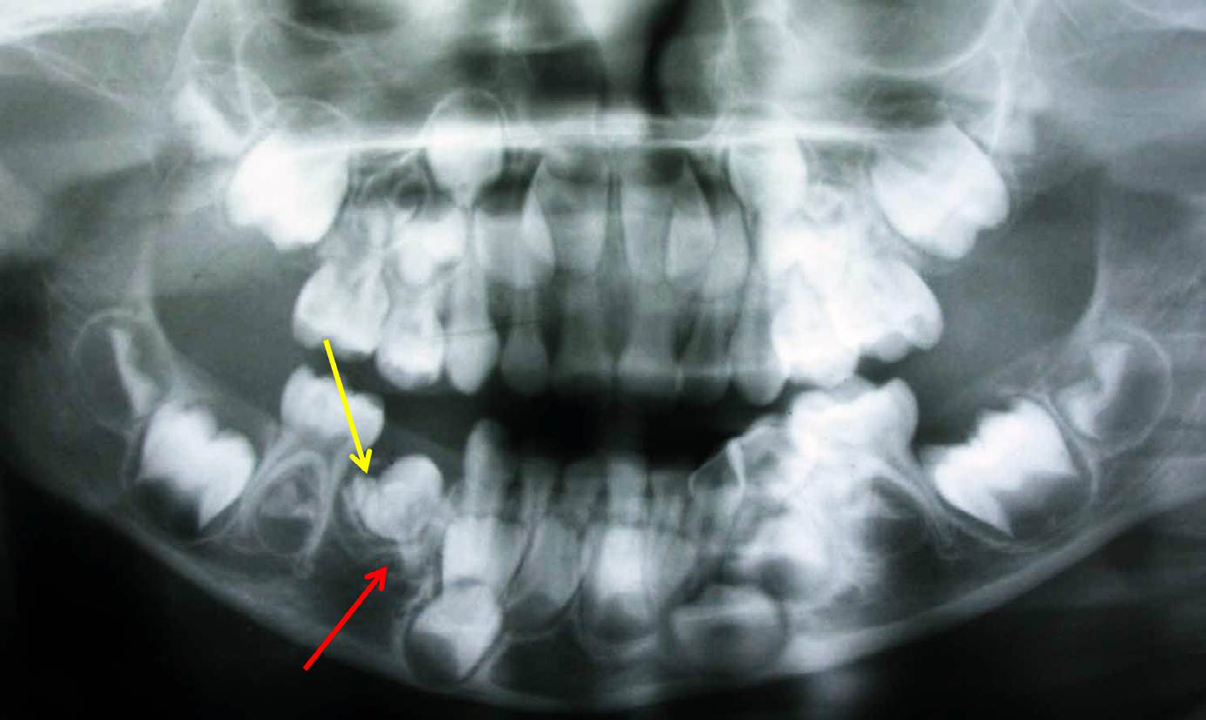
| Type II | Severe (Figure 2) | Impacted primary molar placed within the alveolar bone, with its root apices almost close to the mandibular canal |
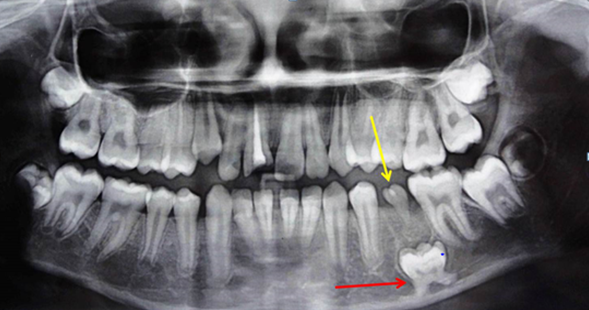
| Type III | Extremely severe (Figure 1) | Impacted primary molar placed within the alveolar bone with its root apices touching the inferior border of the mandible |
Table 1: New Classification System on Primary Mandibular Molar Impaction Suggested by Nagaveni NB in 2024.
Materials and Methods
Children aged 3 to 14 years who reported to Dental wing, Karnataka ENT Hospital and Research centre, Chitradurga, Karnataka, India during the period from 2000 to 2022 were considered for the present investigation.
Inclusion Criteria
Children aged 3 to 14 years and having either complete primary dentition or mixed dentition were included for the study. Children having complete permanent dentition were not included in this study. Children requiring pulpotomy or pulpectomy treatment for the primary molars either unilateral or bilateral (mandibular) and when radiographic examination is required to rule out any pathology were included in this study. Prior to the start of the study patient consent was obtained to use their radiographs in this study. The orthopantomograph and periapical radiographs taken for particular diagnostic or treatment requirements were utilized for screening and examination. The orthopantomographs and periapical radiographs were exposed using the standardized technique with appropriate exposure requirements suggested for these radiographs in order to obtain images with adequate quality. The blurred images were excluded from the study. The retrieved radiographs were examined by a single examiner for the presence of impacted primary molars. To consider the primary molar to be defined as “impacted,” the following description was followed in this study. Any primary molar which was clinically not visible and on radiographic examination found to be located within the alveolar bone and for extent of depth of impaction, impacted primary molar located anywhere from below the cervical margin of the adjacent erupted tooth within the alveolar superior margin to the inferior border of the mandible was considered to classify the level of impaction. The total prevalence, prevalence of first and second molars along with sex ratio and prevalence of unilateral or bilateral and right or left sided occurrence of primary molars were recorded and subjected to statistical analysis.
Statistical Analysis
The final data obtained was statistically analyzed using descriptive statistics to calculate the results in percentages.
Results
In this retrospective analysis, five cases of primary molar impaction were observed in five patients (Figures 1-5) which included both clinical and radiographic examination (Table 2). In this study there were three boys (60%) and two girls (40%) found with impacted primary molars. The age of the children ranged from three to 15 years. Impaction was observed in both primary first and second molars. All impactions were found in the mandibular arch only with no involvement in the maxillary arch. In the mandibular arch, impaction of the first primary molar was observed in only one case (20%) followed by four cases of second molar impaction (80%). Among five cases, including both primary first and second molars, four cases were found on the left side (80%) with only one case on the right side (20%). On the right side, it involved the first molar and one the left side it involved all second molars. There was no bilateral occurrence of primary molar impaction noticed in this study. When level of impaction was graded, two cases were found with Type III (extremely severe variety) (40%) with two graded as Type II (severe type) (40%) and one with moderate type (Type I) (20%). When the condition of succedaneous premolar was evaluated, in one case (20%), malformed second premolar was erupted clinically, in one case odontoma formation was observed (20%), in two cases (40%), the second premolar tooth bud was drifted distally to the primary molar and in another case the premolar was erupting on buccal side (20%). Regarding treatment provided, in none of the patient treatment was rendered.
| Case No. | Gender | Patient age | Impacted primary molar | Symmetry | Presence/absence of succedaneous premolars | Type of impaction | Treatment provided |
|---|---|---|---|---|---|---|---|
| (in years) | |||||||
| 1 (Figure1) | Male | 15 | Second molar | Unilateral (left) | Malformed erupted second premolar | Extremely Severe (Type III) | |
| 2 (Figure2) | Female | 6 | Second molar | Unilateral (left) | Distally drifted second premolar tooth bud | Severe (Type II) | |
| 3 (Figure3) | Male | 4 | First molar | Unilateral (right) | Odontoma formation | Moderate (Type I) | |
| 4 (Figure4) | Female | 15 | Second molar | Unilateral (left) | Buccally erupting second premolar | Extremely Severe (Type III) | |
| 5 (Figure5) | Male | 4 | Second molar | Unilateral (left) | Distally drifted second premolar tooth bud | Severe (Type II) |
Table 2: Characteristic Features of Primary mandibular molars’ impaction found in Indian children.


Discussion
Prevalence of primary molar impaction in different ethnic population is highly essential to formulate diagnostic and therapeutic guidelines for the management of impacted primary molars in children. Occurrence of impaction in the primary molars in turn its occurrence in the early age of the child results in complications and various clinical problems associated with it [3, 4, 5, 6]. As a result, its diagnosis is very important among all clinicians not only with pediatric dentist. Therefore, this retrospective analysis aimed to evaluate the prevalence of primary molar impaction in Indian children using radiographs. Noda T, et al. [6] in 2006, examined 700 patients including 364 males and 336 females and 748 teeth consisting of 26 primary teeth and 722 permanent teeth who were treated for eruption disturbances between 1979 and 2002. The age of the children ranged from one to 16 years. In the primary dentition, the mandibular second primary molar was the most frequently affected tooth followed by the maxillary second primary molar. Pertaining to gender distribution of eruption failure, 30.8% (8 cases) occurred in males about 69.2% (18 cases) were found in females. From this investigation, authors also evaluated the different types of eruption disturbances such as the delayed eruption, impaction, ectopic eruption and occurrence of cystic changes. In the primary dentition, delayed eruption was observed in 16 cases and impaction in 10 cases. The average age when the treatment was commenced for each type of tooth assessment showed that in youngest patient it was one year and 2 months old and the oldest patient was 16 years and 10 months old. Regarding treatment procedures carried out for each type of eruption disturbance, with reference to the primary teeth, exposure of the crown was most frequently carried out treatment. Overall, 19 primary teeth were exposed, 14 of which were primary second molars. Traction was noted only on the primary molars [6]. In the present study, five cases of primary molar impaction were observed, with three cases occurred in boys and two cases occurred in girls. Out of five cases, four were associated with second molars with only one case observed with first molar. This observation was found similar to many previous studies and case reports [1, 2, 3, 4, 5, 6, 7].
Otsuka Y, et al. [7] reviewed clinical features in 13 cases of impacted primary teeth treated at a Pediatric Dental Clinic over a period of 18 years using clinical records, radiographs and oral photographs. This study included five males and eight females aged from one year two months to seven years five months. The mandibular primary second molar was the tooth most frequently involved. This finding was in consistent with the present study. Permanent successor tooth germs were identified in 12 teeth but not in two cases. Five cases were impacted because of presence of odontomas. In this study, the age of the children ranged from three to 15 years old. In one case odontoma formation was observed, in two cases, second premolar tooth bud was drifted distally to the primary second molar, in one case malformed second premolar was erupted clinically and in one case second premolar was erupted buccally.
According to Krakowiak FJ [1], the prevalence of ankylosis of primary molars estimated was of 3.7%. Among the 2234 children evaluated exhibited ankylosis, consisting of a higher prevalence of ankylosis among white children (4.10%) compared to that of black children with a prevalence of 0.93%. The occurrence of ankylosis of mandibular first primary molar was found at an earlier age of the children and more frequently compared to other molars. The frequency of occurrence of second primary molar was more in older children. The same observation was noticed in the present study too. When age of the child was evaluated the increased incidence of ankylosed primary teeth was seen in children between seven and eleven years of age. Based on another 1980 longitudinal study performed by Messer LB, et al. [3], the reported frequency of dental ankylosis estimated was 1.3% to 38.5%.
In cases of severe impaction of the primary molars the succedaneous second premolar is usually placed over the impacted second primary molar. In a study performed by Kjaer I, et al. [5], four cases out of 29 cases evaluated showed arrested eruption of the primary molars and stated that the permanent successors were placed on the occlusal side of the unerupted primary molar as evident from the radiographic examination. In some severe cases of primary molar impaction, the impacted tooth found deep down in the mandible, with the root apex extremely closer to the mandibular canal and nerve. In this retrospective analysis, in two cases the impacted second molar was almost close to the inferior border of the mandible crossing the mandibular canal as evident on the radiographs. These cases were graded as extremely severe form (Type III). In two cases with severe grade, the impacted primary molar root apices were closer to the mandibular canal. Pertaining to impaction of primary molars there is no proper classification system to categorize the level of impaction, as the there is no precise data on its prevalence in different population. Regarding ankylosed and infra-occluded primary molars, Messer researcher [3] in 1980 has given a classification system. Nagaveni NB [12] in her 2024 article, based on her case report and from the data of the previously published case records, has given a new classification system in grading the submerged and ankylosed primary molar. In the present study, author has made an effort to classify the primary mandibular molars impaction based on the findings of different cases found and based on the radiographic features. Author has classified the level of impaction associated with primary mandibular molars including both first and second molars into three types as Type I, II and III which is described in Table 2. Therefore, in the present study this new classification system was used to categorize the impaction level of primary molars observed in Indian children. The current classification system might shed the bright light on other researchers to detect and diagnose the greater number of primary molar impaction in order to render appropriate treatment for children.
Radiographically a well-defined smooth border and a tooth-like appearance of radiopaque structure almost resembling an odontoma type of formation was recorded in some studies and showed that presence of odontomas interfere with eruption of either primary or permanent teeth [13]. Present study also showed presence of odontoma type of radiopaque structure in the place of follicle of impacted primary molar on radiographic examination. In one case, extremely malformed second premolar almost resembling a flower appearance having two cusp like projections and erupted clinically was noticed. Author of this paper has published this interesting and unusual occurrence of malformed second premolar recently [12]. In this study author identified some peculiar radiographic features associated with an impacted primary molar. The impacted primary molar whether it is first or second was surrounded by a thin radiopaque sclerotic border all around the tooth.
Treatment of ankylosed or impacted primary molars depends on evaluation of growth potential of the child. A treatment consisting of early extraction and subsequent space management especially in the younger children is the recommended treatment of choice as mentioned in the available literature. Most of the time conservative monitoring of impacted primary molars is recommended. Extraction is considered when the permanent successor has altered the path of eruption of premolar or if the ankylosed primary molar is severely infraoccluded with the adjacent teeth tipping to prevent the successor from its eruption or both. In this study no definite treatment was considered in none of the cases diagnosed [14, 15]. Some authors suggested enucleation in few cases. However, there is a risk of damage happening to the mental foramen or inferior dental canal during surgical procedures [16]. Therefore, for proper location of impacted primary molars and its relation to the adjacent anatomic structures, advanced imaging modalities including Cone beam computed tomography scan or Magnetic Resonance Imaging can be used in order to avoid complications. It is also important that when planning for surgical procedures including removal of impacted primary molars the potential risks must be carefully evaluated.
Literature shows some diagnostic criteria for the correct diagnosis of primary molars impaction [3, 4, 5, 6, 7, 8, 9, 10]. They are deep retention into the bone, absence of caries or restorations of the crown, no resorption of the roots, frequent passing of the corresponding permanent tooth and possible retention and malposition of the corresponding adjacent permanent tooth [3, 4, 5, 6, 7, 8, 9, 10]. All these criteria clearly differentiate primary molar impaction from the infraoccluded or submerged primary molars [1, 2]. In the present study the above criteria were followed during detection of impacted primary molars using radiographs.
In general, when, impaction of teeth occurs the impacted tooth sometimes undergoes inversion meaning upside down placement of the tooth within the bone with crown facing towards the bone and roots face towards the occlusal level. This type of dental phenomenon is reported with permanent and supernumerary teeth [17, 18]. However, there are publications showing inverted primary molars which are impacted in the alveolar bone of children [19]. Permanent second premolars are the tooth most commonly found with malformations [20].
Conclusion
The present study of retrospective analysis evaluated the impaction of primary mandibular molars occurring in Indian children and found five cases of impacted primary molars including both first and second molars. More number of epidemiological studies including larger sample size is highly essential to predict the exact prevalence of impacted primary molars for early detection and initiation of treatment objectives in children.
References
-
Krakowiak FJ (1978) Ankylosed primary molars. ASDC J Dent Child 45(4): 288-292.
-
Tieu LD, Walker SL, Major MP, Carlos FM (2013) Management of ankylosed primary molars with premolar successors: a systematic review. J Am Dent Assoc 144(6): 602-611.
-
Messer LB, Cline JT (1980) Ankylosed primary molars: Results and treatment recommendations from an eight- year longitudinal study. Pediatric Dent 2(1): 37-47.
-
Matsuyama J, Shoko KK, Sachiko HS, Mitomi T, Tomiko SA (2015) Severe impaction of the primary mandibular second molar accompanied by displacement of the permanent second premolar. Case Report Dent 2015: 582462.
-
Kjaer I, Merete FJ, Andreasen JO (2008) Classification and sequelae of arrested eruption of primary molars. Int J Paediatr Dent 18(1): 11-17.
-
Noda T, Takagi M, Sachiko HS, Taguchi Y (2006) Eruption disturbances in Japanese children and adolescents. Pediatric Dental Journal 16(1): 50-56.
-
Otsuka Y, Mitomi T, Tomizawa M, Noda T (2001) A review of clinical features in 13 cases of impacted primary teeth. Int J Paediatr Dent 11(1): 57-63.
-
Bianchi SD, Roccuzzo M (1991) Primary impaction of primary teeth: a review and report of three cases. J Clin Pediatr Dent 15(3): 165-168.
-
Borsatto MC, Santanna AT, Niero H, Soares UN, Pardini LC (1999) Unerupted second primary mandibular molar positioned inferior to the second premolar: case report. Pediatr Dent 21(3): 205-208.
-
Ferro R, Besostri A, Stellini E, Denotti G, Canesso A (2012) A rare case of unerupted second deciduous molar located inferior to the second premolar: case report. Eur J Paediatr Dent 13(3): 236-238.
-
Nanduri MK, Javangula TP, Mallineni SK, Namineni S (2018) Impacted primary mandibular second molar associated with late-formed second premolar: A rare entity of reverse dentition. Contemp Clin Dent 9(1): S177-S179.
-
Nagaveni NB (2024) Permanent mandibular second premolar with unusual morphology in association with other dental variations – Report of a rarest case. J Dent Res Treat 1(2): 1-8.
-
Nagaveni NB (2023) Complex and composite odontomas – Report of case series with literature review. Clin Pathol 7(1): 000172.
-
Yawaka Y, Shinoguchi K, Fujii M, Oshima S (2022) Impacted mandibular primary second molar: A case report. Pediatric Dental Journal 32(2): 123-128.
-
Sfasciotti GL, Di Carlo G, Marini R, Colaci R, Solidani M, et al. (2017) Surgical management of impacted primary teeth: Report of two cases. Eur J Paediatr Dent 18(1): 19- 22.
-
Karacay S, Aykan OA, Aykan F, Tuzuner T (2014) Impacted deciduous mandibular second molar positioned inferior of impacted second premolar. Gulhane Tip Derg 56: 114- 116.
-
Nagaveni NB, Umashankar KV, Ashwini KS, Chiranjeevi H (2024) ‘Inversion’ of impacted mandibular third molar in ascending ramus of the mandible – Report of a rarest case. Clin Pathol 8(1): 000185.
-
Nagaveni NB (2023) Inversion of impacted mesiodens: Report of case series with literature review. Glob J Res Dent Sci 3(5): 7-12.
-
Jameson GD, Burke PH (1987) “Inversion of second deciduous molar and second premolar”. Br Dent J 162(7): 265-266.
-
Nagaveni NB (2023) A rare combination of tooth agenesis in association with anomalous supernumerary tooth: Report of a rare case. Oral Health Dent 6(1): 18- 21.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage