Does Diabetes and Hypertension have Common Pathophysiology-A Study
Diabetes and hypertension often occur together. Hence they may share some common causes. These causes may be obesity, inflammation, oxidative stress and insulin resistance. Type 2 diabetes may cause hypertension by atherosclerosis. It suggests the importance of keeping an optimal glycaemic profile in general populations. BP screening and monitoring, especially systolic BP, is essential in patients with type 2 diabetes. There are many theories and there is no confirmed mechanisms but, genetic predisposition, insulin resistance, inflammation, oxidative stress, endothelial dysfunction, and have been suggested to explain the link between higher hypertension and diabetes. In our study it was found that 51.8 percent had normal blood sugar and 19% are pre diabetic and 29% are diabetic. As the age increases the incidence of prediabetes and diabetes also increases. Incidence of Diabetes is more in males than in females. Similarly, the prediabetes is also more common in males. Among females 10.75% had normal blood sugar and normal BP and among Males only 3.7% had normal blood sugar and normal BP. Females are more in the prediabetes and elevated & Stage I BP and more males are diabetic and hypertensive.
Introduction
As hypertension is more common in diabetes and they may share some common pathophysiology. The relationship between hypertension and type 2diabetes may not be causal. Type 2 diabetes mellitus (T2DM) has high risk of early mortality and morbidity due to hypertension. Although there are no confirmed mechanisms, genetic predisposition, insulin resistance, inflammation, oxidative stress, endothelial dysfunction, and have been proposed to explain the link between hypertension and diabetes. Blood pressure (BP) and diabetes most probably share common mediators, like inflammation and endothelial dysfunction. Antihypertensive drugs depending upon their ability to counteract the mechanisms that causes endothelial dysfunction can improve or restore endothelium-dependent vasodilatation. In our study it was found that 16.6% of females are prediabetes and 30% are diabetic, among males 2.3% are prediabetes and 28% are diabetic. Above 60 years the pre diabetic [7.5%] and diabetics [10.3%] of the sample population and in the 40-60 years age group 10 % are diabetics. 30% of the people above 60 years are hypertensive and 14.5% in the age group of 40-60 years are hypertensive. Diabetes is more common in males and is also more common in males. More males are hypertensives than females. Only 22% of hypertensives had normal blood sugar and 28% of Elevated or Stage 1 hypertension had normal blood sugar. Among females 62.7 hypertensives are diabetic. There is not much difference between male and female in blood sugar level. More females had normal blood sugar than males. More females had elevated BP and Stage I hypertension than males with prediabetes. Among the hypertensives fewer females and more males are diabetic. The females are more in the prediabetes and elevated & Stage I BP and more males are diabetic and hypertensive. It suggest the importance of keeping an optimal glycaemic profile in general populations, BP screening and monitoring, especially systolic BP is essential in patients with type 2 diabetes.
Material and Methods
Randomised study was conducted on 186 pilgrims attending a religious festival for type 2 diabetes and hypertension. The incidence of diabetes, prediabetes, hypertension, elevated blood pressure, stage 1 & 2 hypertension was recorded. They were analysed for the incidence of hypertension with diabetes, pre diabetes with hypertension, diabetes with elevated BP, diabetes with stage1 & 2 hypertension. The incidence of Diabetes with hypertension among males and females were found out. Incidence of hypertension and diabetes among different age group was analysed.
Results
Out of 186 people 51.8 percent had normal blood sugar and 19% are pre diabetic and 29% are diabetic. Among them 16.6% of females are prediabetes and 30% are diabetic among males 2.3% are prediabetes and 28% are diabetic (Chart 1).
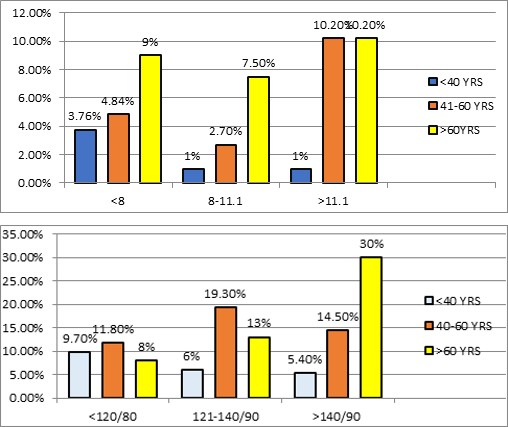
Chart 1: Age and Blood Sugar.
As the age advances the incidence of prediabetic and diabetes also increases. Above 60 years the pre diabetic [7.5%] and diabetics [10.3%] of the sample population.and inn the 40-60 years age group 10 % are diabetics (Chart 2).
Chart 2: Age and Blood pressure.
30% of the people above 60 years are hypertensive and 14.5% in the age group of 40-60 years are hypertensive (Chart 3). Diabetes is more common in males [9.7% and in female 4.85%. Similarly the prediabetes are also more common in males [8.6% to 2%] (Chart 3).
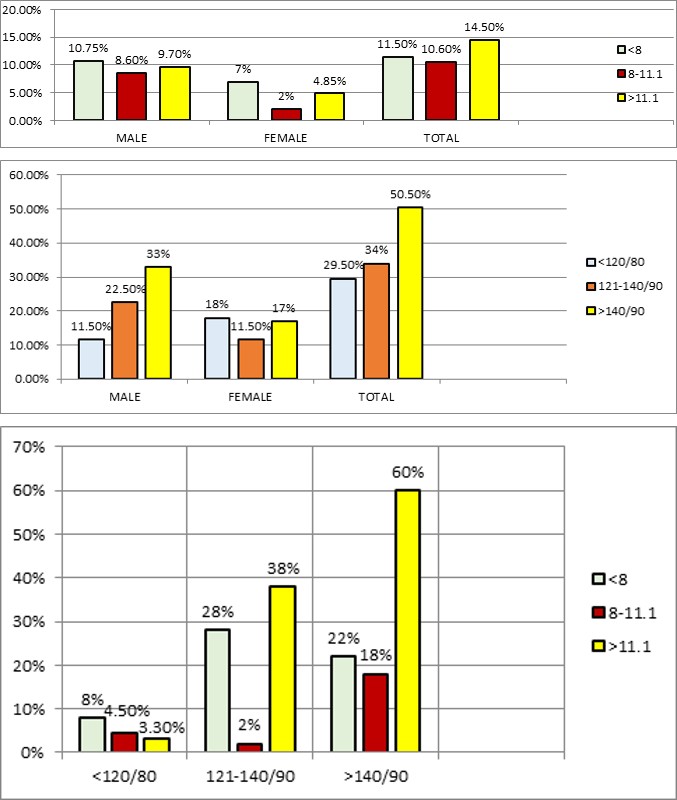
Chart 3: Sex and Blood Sugar.
More males are hypertensives 33% and females 17%, (Chart 4).
Chart 4: Sex and Blood Pressure.
60% of males are both diabetic and hypertensives and 18% are prediabetic with hypertension. 38% of males are diabetic and have elevated or Stage 1 hypertension. Only
22% of hypertensives had normal blood sugar and 28% of Elevated or Stage 1 hypertension had normal blood sugar (Chart 5).
Chart 5: Percentage of Male: Blood Sugar and Blood Pressure.
Among females 62.7 hypertensives are diabetic and 27.6 % have elevated or Stage 1 hypertension. 72% of prediabetes has hypertension and 9% have elevated or Stage 1 hypertension (Chart 6). When analysing the data of 186 persons both male and female 52% had normal blood sugar,19.5% are pre diabetic and 30% are diabetic. There is not much difference between male and female as blood sugar in female is normal in 24% and in male 28%, pre diabetic 7.5% and 12% and diabetic 14% and 16 % respectively. Regarding blood pressure 23.6% had normal blood pressure, 33.3% had elevated or Stage 1 hypertension and 43.1% are hypertensives. Both female and male had normal BP is 52%, Elevated and stage 1 BP 19.5% and Stage II hypertension is 30% (Table 1).
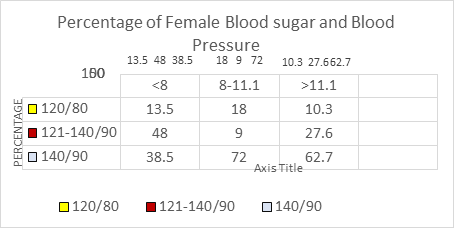
Chart 6: Female: Blood Sugar and Blood Pressure.
| Female 85 | BP 120/80 | BP121/140/90 | BP >140/90 | Percentage | ||||
|---|---|---|---|---|---|---|---|---|
| Normal BP Female | Normal BP Male + Female | Elevated BP& Grade1 Female | Percentage Male +Female | GRADE 2 Hypertension Female | BP Male + Female 186 | Blood sugar % Female 85 | Blood sugar Female % of total 186 | |
| Blood sugar <8 | 20 [24%] | 10.70% | 12 [26.7%] | 6.50% | 13[28.9%] | 7% | 45 [53.6%] | 24.20% |
| Blood sugar 8.1-11.1 | 3 [21.4%] | 2% | 7[50%[ | 3.75% | 4 [28.6] | 2% | 14 [16.6%] | 7.50% |
| Blood sugar >11.1 | 7 [28%] | 3.75 | 9 [36%] | 4.80% | 9 [36%] | 4.80% | 25/84 [29.8%] | [25/186] 14% |
| Total | 30 [35.7] | 16% | 28 [33.3] | 15% | 26 [31%] | 14% | 84 | [84/186] 45% |
| Male 102 | Blood sugar %Male 102 | Blood sugar % of total | ||||||
| Blood sugar < 8 | 7 [13.5%] | 3.70% | 25 [48.1%] | 13.50% | 20 [38.4%] | 24.20% | 52 [51%] | 28% |
| Blood sugar 8.1-11.1 | 4[18.2%] | 2% | 2 [9.1%] | 1% | 16 [72.7%] | 7.50% | 22 [21.5%] | 12% |
| Blood sugar >11.1 | 3[10.3%] | 1.60% | 8[27.6%] | 4.30% | 18[62.7] | [25/186] 14% | 29/102 [28.5%] | 16% |
| 14[13.4%] | 7.50% | 34[33.3%] | 18.20% | 54[53%] | [84/186] 45% | 102 | [102/186] 55% | |
| Total 186 | 44 [23.6%] | 62 [33.3%] | 80 [43.1%] | 186 |
Table 1: Male & Female with Blood Sugar and Blood Pressure.
Among 85 females 10.75% had normal blood sugar and normal BP and among 102 Males only 3.7% had normal blood sugar and normal BP. Among those who had elevated BP and Stage I hypertension, 50 % of females and 9.1% of males are prediabetes and 36% females and 27.6% males are diabetic. Among the hypertensives 28.6% of female and
38.5% of males are pre diabetic and 36% of females and 62.7% of males are diabetic.
When we observe the chart, the females are more in the prediabetes and elevated & Stage I BP and more males are diabetic and hypertensive (Chart 7).
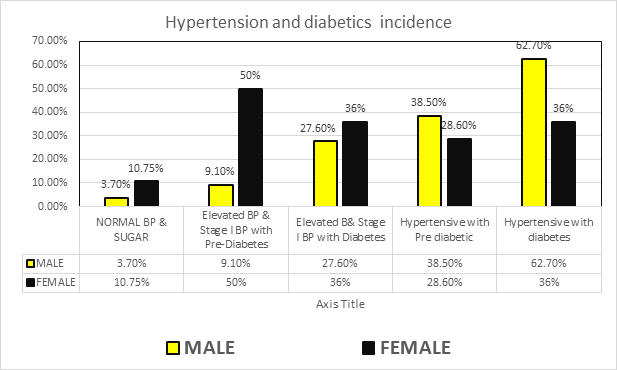
Chart 7: Both Hypertension and Diabetes.
Discussion
Hypertension and type 2 diabetes [T2D] are two different aspects of metabolic syndrome which includes obesity and cardiovascular disease. It is often found that diabetes and hypertension often occur together. Hence they may share some common causes like obesity, inflammation, oxidative stress and insulin resistance. Diabetes induced atherosclerosis make the arteries non-elastic and high blood pressure. Hypertension is common among diabetic patients. Prevalence of hypertension among diabetes depends on type and duration of diabetes, sex, age, race/ethnicity, BMI, glycaemic control, and the presence of renal disease [1]. The relationship between hypertension and type 2 diabetes may not be causal. To prevent hypertension it is important to keep an optimal glycaemic profile in general populations, BP screening and monitoring, especially systolic BP is essential in patients with type 2 diabetes [2]. In patients with hypertension or diabetes there are changes in left ventricular (LV) diastolic filling anticipate diastolic heart failure. This hypothesis was tested and proved that increased fasting and post prandial glucose is associated with significant diastolic dysfunction as demonstrated by tissue Doppler imaging (TDI) in hypertensive patients. Initially abnormal fasting and post prandial glucose levels are associated with increased diastolic impairment in uncomplicated hypertensive patients, suggested that hyperglycaemias may increase the risk of diastolic heart failure even without diabetes [3]. Diabetes has been shown to be associated with a 2-fold increased risk of all-cause mortality and a 3-fold increased risk of cardiovascular disease mortality relative to age and sex-matched controls in a contemporary primary care population in the United Kingdom [4].
Type 2 diabetes mellitus (T2DM) is associated with a high risk of early mortality and morbidity from hypertension. The prevalence of hypertension among type 2 diabetes patients was found to be 59.5%. Stage 1 hypertension was the most common (30.95%). The odds of hypertension was higher among age group of 50-60 years, patients from urban area, with longer duration of T2DM, with BMI ≥25 kg/m2, with poor glycaemic control and patients who were current cigarette smokers [5]. Among the overall cohort, 20 mm Hg higher SBP and 10 mm Hg higher diastolic BP were associated with a 58% and a 52% higher risk of new-onset diabetes [6]. A large Mendelian randomization study using 28 genetic variants as an instrumental variable to exclude confounding effects showed that genetically elevating the systolic BP by 1 mm Hg was associated with a 2% increased risk of T2DM or 22% for a 10-mm Hg change in systolic BP in Europeans [7]. Emdin, et al. [6] stated that hypertension is a significant risk factor for developing type 2 diabetes (T2DM), and concluded that more investigations are needed to determine whether this association is causal. A study was conducted a random- effects meta-analysis of prospective observational studies of BP and incident diabetes. Findings from 30 studies having 285,664 participants revealed 17,388 had diabetes [8].
In another study done on 4.1 million adults in 2015 revealed that the systolic blood pressure by 20 mm Hg and higher diastolic blood pressure by 10 mm Hg were associated with increased risk for type 2 diabetes [6]. Among middle-aged and elderly Chinese population hypertension is a risk factor for type 2 diabetes. The incidence of diabetes was 2.57%, 3.75%, and 6.71% in the normal BP, elevated BP& stage 1 hypertension, and hypertension groups, respectively. The association of hypertension with diabetes was more in patients of 50 age than the older age groups: In Chinese adults both hypertension and prehypertension were associated with higher risk of developing diabetes compared to normal BP. It has been found that an increase of 10 mm Hg in systolic blood pressure 5 mm Hg in diastolic blood pressure was associated with an 8% increased risk of incident type 2 diabetes. Insulin resistance, genetic factors, inflammation, endothelial dysfunction, oxidative stress has been proposed to explain the link between hypertension and diabetes [9].
The link between diabetes and hypertension may be due to certain processes in the body that can affect both conditions such as inflammation. A meta-analysis in revealed that people with hypertension have a higher risk of developing type 2 diabetes [6]. Hypertension and diabetes may share common mediators, like inflammation and endothelial dysfunction [10]. Chronic inflammation is found to be associated with hypertension [11]. Both Interleukin-6 and nitric oxide appear to be mediators of diabetes risk and also cause hypertension by endothelial impairment. Essential hypertension is found to be associated with impaired endothelium-dependent vasodilation which is caused the production of oxygen free radicals which can destroy nitric oxide (NO), and its protective effects on the blood vessel wall. Antihypertensive drugs depending upon their ability to counteract the mechanisms that causes endothelial dysfunction can improve or restore endothelium-dependent vasodilatation. Calcium channel blockers, dihydropyridine- like drugs, can reverse the impaired endothelium-dependent vasodilation. Angiotensin II receptor antagonist can also improve basal NO release and decrease the vasoconstrictor effect of endogenous endothelin-1.This makes us to suspect that elevated BP may cause new-onset diabetes [12]. It is rationale to suspect that elevated BP may cause new-onset diabetes [13].
Some believe that oxidative stress has shared pathways for diabetes and C-reactive protein which is an inflammatory biomarkers is reported to be associated with both an elevated BP and diabetes in the general population [14, 15, 16]. Endothelial dysfunction is involved in the development of hypertension whose biomarkers are associated with increased risk of diabetes [16, 17]. Insulin resistance is one of the causes of diabetes is thought to increase the risk of hypertension and thus can partly explain the link between BP and diabetes [18]. In women the association between fasting insulin concentrations and risk of hypertension is more pronounced in women. In the general population elevated fasting insulin concentrations or insulin resistance is with an exacerbated risk of developing. Early investigations to identify hyperinsulinemia or insulin resistance will help clinicians to identify the high risk of hypertensive population [18]. There is a modest protective association between increased insulin sensitivity and lesser risk of developing hypertension. By improving insulin sensitivity we can prevent the development of hypertension [19].
Both diabetes and hypertension must share a genetic susceptibility [20]. C-reactive protein is associated with an increased chance of developing hypertension even in persons with lower baseline blood pressure. Increasing level of C-reactive protein will predict future development of hypertension. Hence it suggests that hypertension may be an inflammatory [18]. The inflammatory markers, like interleukin 6 (IL-6) and tumour necrosis alpha (TNF-alpha) were found to be elevated in hypertension in well-controlled studies. TNF-alpha and IL-6 can be independent risk factors for hypertension in normal subjects [19]. Increased level of other biomarkers like ICAM-1 and E-selectin predicts the development of type 2 diabetes [20]. Variants in genes encoding like adiponectin, adrenomedullin, apolipoprotein found to correlate with both diabetes and hypertension. Using Mendelian randomization, genetically modified hypertension and type 2 diabetes were constructed using 233 and 134 single nucleotide polymorphisms, respectively. It was found that genetically modified type 2 diabetes is associated with increased risk of hypertension whereas the genetically determined hypertension showed no such relationship with type 2 diabetes. Type 2 diabetes may causally affect hypertension, whereas the relationship from hypertension to type 2 diabetes is may not be causal [2].
When hypertension is treated with angiotensin- converting enzyme inhibitors and angiotensin receptor blockers there is reduced incidence of diabetes [21]. Some antihypertensive medications used to treat hypertension has reduced the risk of diabetes [21, 22]. The association of antihypertensive drugs with incident diabetes is therefore lowest for angiotensin-converting-enzyme (ACE) inhibitors with angiotensin-receptor blockers (ARB) followed by Calcium channel blocker and placebo, beta blockers and diuretics in rank order [21].
References
-
Ian H de Boer, Sripal Bangalore, Athanase Benetos, Andrew M Davis, Erin D Michos, et al. (2017) Diabetes and Hypertension: A Position Statement by the American Diabetes Association. Diabetes Care 40(9): 1273-1284.
-
Dianjianyi Sun, Tao Zhou, Yoriko Heianza, Xiang Li, Mengyu Fan, et al. (2019) Type 2 Diabetes and Hypertension. Circ Res 124(6): 930-937.
-
Cristiana Catena, GianLuca Colussi, Flavia Martinis, Francesca Pezzutto, Leonardo A Sechi (2013) Plasma glucose levels and left ventricular diastolic function in nondiabetic hypertensive patients. Am J Hypertens 26(11): 1353-1361.
-
Taylor KS, Heneghan CJ, Farmer AJ, Fuller AM, Adler AI, et al. (2013) All-cause and cardiovascular mortality in middle-aged people with type 2 diabetes compared with people without diabetes in a large U.K. primary care data base. Diabetes Care 36(8): 2366-2371.
-
Yonas Akalu, Yitayeh Belsti (2020) Hypertension and Its Associated Factors Among Type 2 Diabetes Mellitus Patients at Debre Tabor General Hospital, Northwest Ethiopia. Diabetes Metab Syndr Obes 13: 1621-1631.
-
Connor A Emdin, Simon G Anderson, Mark Woodward, Kazem Rahimi (2015) Usual Blood Pressure and Risk of New-Onset Diabetes: Evidence From 4.1 Million Adults and a Meta-Analysis of Prospective Studies. Journal of the American College of Cardiology 66(14): 1552-1562.
-
Aikens RC, Zhao W, Saleheen D, Reilly MP, Epstein SE, et al. (2017) Systolic blood pressure and risk of type 2 diabetes: a Mendelian randomization study. Diabetes 66(2): 543-550.
-
Donna K Arnett (2015) Analysis of Large Electronic Health Record Databases Supports Blood Pressure- Incident Diabetes Association. Journal of the American college of cardiology 66(14): 1563-1565.
-
Xue Yang, Jian Chen, An Pan, Jason H Y Wu, Fei Zhao, et al. (2020) Association between Higher Blood Pressure and Risk of Diabetes Mellitus in Middle-Aged and Elderly Chinese Adults. Diabetes Metab J 44(3): 436-445.
-
Reaven GM, Lithell H, Landsberg L (1996) Hypertension and associated metabolic abnormalities-the role of insulin resistance and the sympathoadrenal system. N Engl J Med 334(6): 374-381.
-
Chamarthi B, Williams GH, Ricchiuti V, Srikumar N, Hopkins PN, et al. (2011) Inflammation and hypertension: the interplay of interleukin-6, dietary sodium, and the renin-angiotensin system in humans. Am J Hypertens 24(10): 1143-1148.
-
Taddei S, Virdis A, Ghiadoni L, Sudano I, Salvetti A (2000) Antihypertensive drugs and reversing of endothelial dysfunction in hypertension. Curr Hypertens Rep 2(1): 64-70.
-
James B Meigs, Frank B Hu, Nader Rifai, JoAnn E Manson (2004) Biomarkers of endothelial dysfunction and risk of type 2 diabetes mellitus JAMA 291(16): 1978-1986.
-
Cheung BM, Li C (2012) Diabetes and hypertension: is there a common metabolic pathway? Curr Atheroscler Rep 14(2): 160-166.
-
Sesso HD, Buring JE, Rifai N, Blake GJ, Gaziano JM, et al. (2003) C-reactive protein and the risk of developing hypertension. JAMA 290(22): 2945-2951.
-
Bautista LE, Vera LM, Arenas IA, Gamarra G (2005) Independent association between inflammatory markers (C-reactive protein, interleukin-6, and TNF- alpha) and essential hypertension. J Hum Hypertens 19(2): 149-154.
-
Odegaard AO, Jacobs DR, Sanchez OA, Goff DC, Reiner AP, et al. (2016) Oxidative stress, inflammation, endothelial dysfunction and incidence of type 2 diabetes. Cardiovasc Diabetol 15: 51.
-
Wang F, Han L, Hu D (2017) Fasting insulin, insulin resistance and risk of hypertension in the general population: a meta-analysis. Clin Chim Acta 464: 57-63.
-
David C Goff Jr, Daniel J Zaccaro, Steven M Haffner, Mohammed F Saad (2003) Insulin sensitivity and the risk of incident hypertension: insights from the Insulin Resistance Atherosclerosis Study. Diabetes Care 26(3):805-809.
-
Cheung BM, Li C (2012) Diabetes, and hypertension: is there a common metabolic pathway? Curr Atheroscler Rep 14(2): 160-166.
-
Elliott WJ, Meyer PM (2007) Incident diabetes in clinical trials of antihypertensive drugs: a network meta- analysis. Lancet 369(9557): 201-207.
-
Roumie L, Adriana M Hung, Gregory B Russell, Jan Basile, Kathryn Evans Kreider, et al. (2020) Blood Pressure Control and the Association with Diabetes Mellitus Incidence: Results from SPRINT Randomized Trial. Hypertension 75(2): 331-338.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance