Managing Diabetes and Obesity in COVID-19 among Maori Adults in New Zealand using Non-Pharmacological Interventions
Background: World Health Organisation estimated that diabetes and obesity are responsible for 1.6 million and 4 million mortalities, globally. Likewise, New Zealanders also face the serious consequences of diabetes and obesity mainly impacted Maori due to existence of various health disparities. Presently, researches showed that people with pre-existing diabesity conditions are more susceptible to acquire COVID-19 and resulted in 48% mortality, globally. Aim: This literature review was aimed to identify the effects of Non-Pharmacological (lifestyle) interventions implemented for managing diabetes and obesity among adult Maori in New Zealand especially during COVID-19. Method: To conduct a comprehensive literature review, the universally acclaimed peer-reviewed electronic databases such as PubMed, ProQuest, EIT online and cross-references of included articles were used to discover the most relevant, recent studies on the present topic. Reviewer screened the articles based on inclusion criteria. Electronically available peer-reviewed journal articles which include the interventions on diabetes and obesity for adult Maori of New Zealand and should be conducted between 2015 to 2020 were included. Results: Reviewer searched 35 articles in total. Out of which 07 articles were selected according to inclusion criteria. From total 07, 02 articles included lifestyle interventions exclusively on adult Maori men and 05 studies included adult Maori and other ethnic groups. Findings of the review revealed that non-pharmacological interventions without incentives showed more retention rate of Maori adults as compared to intervention with incentives. All the included articles use Maori culturally acceptable approach in implementing lifestyle interventions for diabetes and obesity prevention. Conclusion: More research needs to be conducted for diabetes and obesity prevention among Maori adults in New Zealand as there is limited literature available which becomes insufficient during special circumstances such as COVID-19 Pandemic.
Introduction
Non-Communicable diseases (NCDs) such as Obesity and diabetes emerge as a biggest burden and concern for public health [1] and these are occurred due to metabolic disorders [2]. Obesity shares a close relationship with the incidence of diabetes because overweight is considered as a major contributory factor in the occurrence of T2DM, hence it was proven that most of the obese people are also suffering from diabetes or at risk of it. Therefore, the association of these two NCDs is called as ‘diabesity’ [3] and cause serious health concerns, globally. Furthermore, NCDs termed as “slow killers” because it causes large mortalities, morbidities and economical losses, globally [4]. Abdelaal [5] mentioned in their article that even 01 kg/m2 surge in Body mass index (BMI) can increase the danger of T2DM by 20% and it will increase up to 100% to 300% if BMI rise from 27.2 to more than 29.4 kg/m2, respectively.
Diabesity becomes a global concern as it was estimated that, there is rapid surge befell in obese and diabetic people which touches 671 million and 463 million, respectively [6]. Additionally, there are 5% world’s population is comprised of Indigenous peoples and it was evaluated that more than 50% of them above the age of 35 years suffer from T2DM which develop as an epidemic, worldwide [7]. About 231 million people globally are ignorant about the fact that they are diabetic because they are under-diagnosed reported by International Diabetes Federation, 2019 [8]. Obese women during pregnancy suffer from Gestational Diabetic Mellitus (GDM) and its prevalence depends on ethnicity and screening tool used for diagnosis, however, estimated figures reported by Europe were 2 to 6%, in US 7% and followed by high- risk groups with 20% which included New Zealand too [9]. In 2016 there were 1.6 million mortalities occurred due to diabetes and it was a 5% rise in premature deaths between 2000 to 2016 [10]. Whereas, increased BMI caused 4 million mortalities, worldwide [2] and if these conditions combined then the situation get worsen [5].
Similarly, New Zealand also showed a high prevalence of Obesity and Diabetes and ranked third in obesity prevalence among adults in all the Economic Co-operation and Development (OECD) nations. In 2016, around 32% of New Zealander adults were overweight, and predictions showed that their mean BMI might increase to 30 and above by 2030. Similarly, the number of diabetics (5.6%) and prediabetes (25.5%) adults is also showing an alarming situation [11]. Out of which, 7.2% were Maori adults and experience 9-year less average life expectancy than non-Maori. Further, literature revealed that there were 2 times and 1.7 times rise in prevalence of diabetes and obesity, respectively among Maori than Non-Maori adults and worsen with the existence of health inequities among Maori [12, 13]. Obesity rates among Maori men and women are surging from 41% to 42% and 40% to 48%, respectively [14]. Besides, the GDM prevalence rate is also on higher side among Maori women for example from total 17% obese pregnant women (BMI> 25), nearly 10% were suffering from GDM and in which 6% were Maori women compared to (5%) European women [9].
A recent study evaluated that obese people are more susceptible to acquire COVID-19 infection and at high risk of (48%) mortality [15]. Similarly, 14% of people who acquired COVID-19 are diabetic and suffer from its complications and deaths, globally [16]. Likewise, the New Zealand Maori are also suffering from pre-existing health conditions such as diabetes and obesity and at high risk of getting Covid-19 infection as compared to other ethnicities [17].
To overcome the epidemic of diabesity World Health Organisation, 2016 [18] set target-7 in SDGs as “halt the rise in diabetes and obesity” and focus on decreasing the T2DM because it is mostly preventable. To manage the epidemic situation, they stressed on intersect oral and community- based approaches to control the incidence of preventable risk factors for example high BMI, obesity, unhealthy eating and sedentary lifestyles. Further, health promotion methods such as improving physical activity and healthy eating options help in reducing obesity and delaying diabetes as these modifications are more effective than prolonged multi-drug therapies. Therefore, the International Diabetes Federation (IDF) prepared a global plan for lifestyle interventions [19]. Similarly, to reduce diabetes and obesity, New Zealand set its target such as 10% reduction of physical inactivity in adults i.e. from present 49% to 44% and consumption of saturated fats in adults from present 13% to 11% [20].
This review will include the studies according to inclusion criteria and will evaluate the various non-pharmacological (dietary modifications, increase physical activity, counselling sessions, lifestyle change, self- management, weight reduction) interventions which are used to reduce obesity and diabetes among adult Maori of New Zealand. Further, provides evidence-based suggestions for future research for managing diabetes and obesity among adult Maori of New Zealand.
Methodology
Search Strategy for Including Studies
The literature review was carried out by using online databases such as PubMed, ProQuest, EIT online, and cross- references of included interventional studies published between 2015 to 2020. The authors used Maori Health review and Ministry of Health websites for data accuracy. The review focuses on intensively searched primarily on Maori, who are “aboriginal people” and have a unique connection with the environment of Aotearoa, New Zealand [21].
Study Selection and Data Extraction with the Synthesis of Articles
07 review articles were selected by using specific keywords such as Maori, Diabetes, obesity, lifestyle interventions, Indigenous people, New Zealand and published between 2015 to 2020. The authors segregated the articles and obtained a synthesis matrix based on the following domains (Table 1)
| Domains | Features |
|---|---|
| Population | Adult Maori both exclusively and in combination with another ethnicity |
| Study Design | Randomised control trial, mixed method, qualitative, quasi-experimental |
| Interventions with duration>4 weeks | Initiatives/program which were used to modify lifestyle such as physical activity, weight reduction, exercise. |
| Non communicable disease | Diabetes or obesity, both |
| Comparison | Type of intervention- Incentive (Yes/no) technological based (mobile) |
| Outcomes | Reduction/positive effects in obesity and diabetic markers, adherence or non-adherence to health lifestyle, culturally acceptable |
Table 1: Review domains and features.
Quality Assessment: Further, the authors extensively assessed the articles for delicacy, chosen according to inclusion and exclusion criteria. The reference lists of all the selected studies were also reviewed to identify additionally available articles.
Inclusion Criteria: The studies were searched through an online database and included according to the following criteria:
- Should include Maori adult of New Zealand
- Should be academic sources such as scientific journals and books
- Full research articles available
- Conducted between 2015 to 2020
- Include interventions (>4 weeks duration) for preventing diabetes/ obesity via lifestyle modifications.
Exclusion Criteria
- Maori not included as participants/group
- Study Intervention not included lifestyle modifications for diabetes/obesity
- Articles full text did not have open access.
Results
Out of 35 searched articles, 07 studies were included in the review after extensive screening, removal of repetitive studies and following inclusion criteria. Selection procedure of 07 studies is explained in (Figure 1).
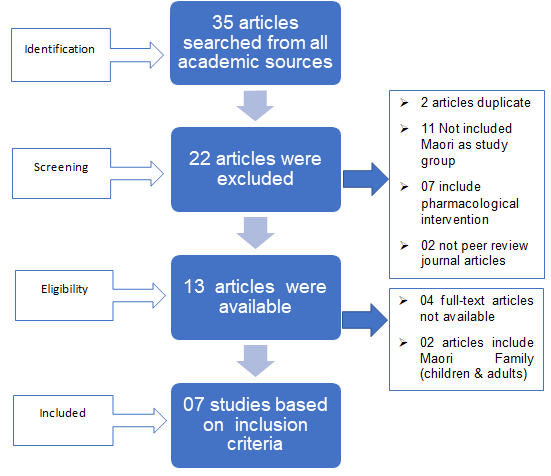
Table 2 showed the selected studies which were chosen from peer-reviewed journals and reference list also reviewed for potential additional articles. Participant’s numbers in chosen articles were ranged between 18 to 726. Additionally, 02 studies were conducted exclusively on Maori adults and remaining 05 comprised other ethnicity also such as Pacific people, European. From the total, 03 and 02 studies provided lifestyle interventions exclusively for obesity and diabetes, respectively. Whereas, 02 studies reflect interventions for both conditions. In 03 intervention studies, there was a provision of some monetary incentives whereas, 04 studies given no incentives to their participants. The mode of delivery was online- internet-based, telephonic and face to face or both types were used by the authors. It was interesting to know that all the studies used culturally based approaches for providing lifestyle interventions to Maori people.
| S. No | Author (Year) | Population (N) | Study Design | Intervention/ Duration | NCD (Diabetes/ Obesity/both) | Comparison/Culturally Designed |
|---|---|---|---|---|---|---|
| 1 | Glover, et al. [22] | 147 intervention & 150 control group (Maori and Pacific) | Quasi- experimental design | Online and community level/ three, 06 months competition | Diabetes and obese/ cardiovascular | Incentives given ($50- $3000)/Culturally suitable team-based competition of weight reduction, |
| 2 | Ni Mhurchu, et al., [13] | Intervention group- 337 Maori (19 clusters) & 389 Pacific people (18 clusters) Control group-320 Māori (15 clusters) & 405 Pasific participants (17 clusters) | Two-arm, cluster- randomised controlled trial | OL@-OR@ mobile health- programme, community involve/12 weeks | Obesity | Incentives given (NZ$500/ cluster)/ Culturally suitable messages send by application on healthy eating, physical activity stress reduction, sleep improvement, and weight management |
| 3 | Glover, et al. [23] | 130 or 19 teams (Maori and Pacific adults) | Qualitative method | Team weight loss competition trial/ daily challenge activity upto 24 weeks | Obesity | Incentive given (Cash)/ Culturally- Te Whare Tapa Wha -a Maori holistic model |
| 4 | Warbrick, et al. [24] | 18 Maori Men | Qualitative study | Promote awareness about physical activity and reduction of weight / 3 focus group discussion prior to 12- week exercise intervention | Obesity | No incentives/ Culturally- included kaupapa (values and principles) of Māori cultural approach |
| 5 | Williams, et al. [25] | 68 (Maori) 70(European New Zealander) | Randomised trial | Green Prescription delivery: face- to-face and telephonic on lifestyle intervention/6 months | Diabetes | No incentives/Cultural suitable approach during recruitment of Maori |
| 6 | Sarfati, et al. [26] | 430 (Maori & Pacific people) | Randomised controlled trial | The BetaMe program Self- management intervention (all-inclusive)/ 12 months | Diabetes and Pre- Diabetes | No incentives/ Culturally- involvement of Maori healthcare providers |
| 7 | Oetzel, et al. [27] | 02 groups Maori Men (8 & 24=32) | Multi-method approach, Qualitative | lifestyle intervention/ 12- week | Obesity and diabetes | No incentives/ Culturally- inclusion of He Pikinga Waiora (HPW) Implementation Framework |
Table 2: Attributes of the included articles of lifestyle interventions for adult Maori of New Zealand.
Discussion
The findings of the present review revealed some of the encouraging facts and culturally acceptable frameworks for reducing the risk of prevalence of diabetes and obesity among adult indigenous people of New Zealand.
Summary of Non-Pharmacological Intervention Studies with Incentives (Table 2 study numbers 1, 2 and 3)
Population: Among the first 03 incentive-based lifestyle intervention studies the number of participants ranged from 130 to 726. All the studies include Maori and Pacific adults above 16 years in age and New Zealand, residents. Eligible participants should have BMI equal to or above 30kg/m2 or at risk of/diagnosed T2DM in two intervention studies but eligible participants of Ni Mhurchu [13] study was to have regular accessibility of internet services and availability of anyone gadget such as laptop, computer, the mobile phone was required. Study Design: First two studies (Table 2) were quasi- experimental and cluster randomised control trial which consists of intervention groups as well as control groups whereas, number 3 article was a qualitative study. Intervention: Intervention provided by Glover [22] in their study was team-based competition using internet delivery for weight reduction, nutrition education, family support, lifestyle changes, total cholesterol and glycated hemoglobin (HbA1c) reduction. It includes incentives as one entry voucher of $50 per region for completing baseline study and followed with each $1000 reward for utmost progress by the regions in 2 months and 4 months. Then, $ 6000 was given to region with the highest progress in 6 months. Another study involves methods of weight reduction, education and support which were culturally appropriate for Maori such as Maori holistic model Te Whare Tapa Wha [23]. However, first two studies (Table 2) involve the community and online delivery of interventions with the use of technological gadgets, mobile application (OL@-OR@) to provide cultural tips for lifestyle modification, education, weight reduction competition. The duration of intervention was ranged from 12 to 24 weeks. Outcomes: According to the first study (Table 2) the weight reduction incentive-based intervention showed positive effects as well as culturally acceptable to Indigenous and Pacific peoples. This initiative also helps in reducing the cost to the healthcare system because of internet-based delivery of lifestyle interventions. However, second and third studies showed non-adherence to lifestyle modifications [13, 22] and an inadequate result occurred due to high attrition rate, respectively among Maori and Pacific groups. Despite the provision of monetary incentives dropout rate was high because of some personal commitments, five participants left due to pregnancy [22].
Summary of Non-Pharmacological Interventions Studies without Incentives (Table 2 study numbers 4, 5, 6 and 7)
Population: The number of participants in studies from 4 to 7 was ranged between 18-430. Study number 4 and 7 were exclusively conducted on Maori men for the prevention of obesity. Whereas, the remaining two studies included diabetes in combination with pre-diabetes or obesity as a chronic condition. Eligibility of participants for studies from 4 to 7 include Maori as one study group, consent for participation, along with correct contact details, not dependent on insulin, dialysis for next one year, no ambulatory issues [25], age criteria (18-72 years), HbA1c (41-70 mmol/mol) range from last two years, internet access (computer/laptop/mobile phone), not on insulin or not a diagnosis for T2DM [26], remaining two studies include exclusively Maori men with BMI>25 or more along with these criteria [24] included the risk of Obesity whereas Oetzel [27] focus on T2DM as well as obesity/CVD risk among participants. Study Design: Two studies (5 & 6) used randomised control trials with intervention and control groups whereas studies (4 and 7) used qualitative or multimethod approach (pre- and post-intervention design).
Intervention: Warbrick [24] conducted a qualitative study on obese adult Maori Men to encourage them for physical activity and motivating for modifying their lifestyle (exercises). Further, a study used internet-based and face to face delivery for a green prescription such as healthy diet, physical activity (swimming, weight training) and motivational support [25]. Another trial included BetaMe interventions which constitute 04 major elements that are health coaching, health literacy, checking goal and peer support to prevent the risk of diabetes and prediabetes and delivered through mobile with internet facility [65]. Furthermore, Oetzel [27] used He Pikinga Waiora (HPW) Implementation Framework for implementing lifestyle interventions (physical activity and diet pattern) and include support from peer or community health worker to prevent diabetes and obesity in Maori Men. The duration of interventions in all the studies without incentives was laid between 3 months to 12 months. Outcome: Warbrick [24] used Kaupapa culturally acceptable approach for Maori and it motivated them to adopt a healthy lifestyle. Further, the green prescription method presented encouraging clinical effects for improving the life of T2DM patients [25]. However, the results of BetaMe intervention are awaited but if it comes positive then it will provide an opportunity to promote self-care among diabetic patients which is also culturally acceptable [26]. Interestingly, Oetzel [27] study showed 88% retention rate of indigenous men and showed a huge positive effect in weight reduction. All these positive results occurred without the provision of incentives.
Overall, review findings suggested that incentive-based interventions showed mixed results as a study showed positive effects because they were designed more culturally and realistic and make it largely acceptable among Maori adults. Further, the delivery of health tip messages through mobile and other internet-based gadgets were effective in weight reduction and cost-effective [22]. However, Ni Mhurchu [13] reflect contrast results as non-adherence to healthy behaviour (healthy diet, physical activity, stress and sleep management) by participants and in another article, despite promising weight reduction strategies, there was a high rate of attrition among Maori people [23].
Contrast, the interventions without incentives showed high retention rate of Maori participants and showing weight reduction up to 4% and positive health effects such as improved eating habits [27]. Similarly, an article which delivers green prescription through mobile phone also showed small clinically positive effects on Maori people suffering from T2DM with a reduction in HbA1c levels by more than 3 mmol/mol and body weight more than 1.5 kg [25]. Whereas one study trail is ongoing, and its result is awaited but the study reflects that if results will be positive then it will provide self-management of diabetes and prediabetic solutions for Maori and Pacific people [26]. Remarkably, the health promotion intervention motivates Maori men towards a physical activity as documented by Warbrick [24].
Furthermore, the present review has some limitations. Firstly, all the articles included in the review were selected from peer-reviewed journals, so it does not provide a broad scenario of non-pharmacological interventions to manage diabetes and obesity among adult Maori. Secondly, due to strict inclusion criteria of review and lack of availability of literature on management of obesity and diabetes among Maori [22], might understate the impact of interventions on adult Maori.
Conclusion
To conclude, review on non-pharmacological intervention with incentives showing not much difference in results than studies without incentive for adult Maori and other ethnic groups. Undoubtedly, all the chosen studies incorporated the Maori cultural framework/approaches in their interventions. However, due to some personal reasons, participants showed a high attrition rate in few studies.
Recommendations
The findings of the review recommend that additional benefits could be introduced among adult indigenous people to encourage healthy behaviour among them such as involvement of whanau in interventions for reducing weight, it inculcates the feeling of belongingness to them, benefits for job hours as compared to monetary aids without working it increases their physical activity, improve health literacy including technical knowledge such as mHealth tools. Undeniably, the inclusion of Maori cultural component is important. Future studies on New Zealand Maori adults need to include more culturally acceptable non-pharmacological interventions with additional benefits for reducing prevalence of obesity and diabetes among them.
Author Contribution
Both authors have contributed equally in the conception and design of the study, acquisition of data, analysis and interpretation of data, drafting the manuscript and revising it critically for important intellectual content, final approval of the version to be submitted.
References
-
Silveira EA, de Souza Rosa LP, de Carvalho Santos ASeA, de Souza Cardoso CK, Noll M (2020) Type 2 Diabetes Mellitus in Class II and III Obesity: Prevalence, Associated Factors, and Correlation between Glycemic Parameters and Body Mass Index. Randomized Controlled Trial 17(11): 3930.
-
Ashkan Afshin, Mohammad H Forouzanfar, Marissa B Reitsma, Patrick Sur, Kara Estep (2015) Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med 377(1): 13-27.
-
Leitner DR, Frühbeck G, Yumuk V, Schindler K, Micic D, et al. (2017) Obesity and Type 2 Diabetes: Two Diseases with a Need for Combined Treatment Strategies - EASO Can Lead the Way. Obes Facts 10(5): 483-492.
-
Bergman M, Jagannathan R, Narayan KMV (2020) Nexus of COVID-19 and diabetes pandemics: Global public health lessons. Diabetes research and clinical practice 164: 108215.
-
Abdelaal M, le Roux CW, Docherty NG (2017) Morbidity and mortality associated with obesity. Ann Transl Med 5(7): 161.
-
Mozaffarian D (2020) Dietary and policy priorities to reduce the global crises of obesity and diabetes. Nature Food 1(1): 38-50.
-
Harris SB, Tompkins JW, TeHiwi B (2017) Call to action: A new path for improving diabetes care for Indigenous peoples, a global review. Diabetes Research and Clinical Practice 123: 120-133.
-
Williams R, Colagiuri S, Chan J, Gregg E, Ke C, et al. (2019) IDF Atlas, 9th (Edn.), International Diabetes Federation.
-
Daly B, Raiman I, Goodson J (2017) Screening for diabetes in pregnancy in a regional area with a high Māori population. The New Zealand medical journal 130(1450): 25-31.
-
WHO (2020) Diabetes. World Health Organisation.
-
De Bruin WE, Stayner C, Lange Md, Taylor RW (2018) Who Are the Key Players Involved with Shaping Public Opinion and Policies on Obesity and Diabetes in New Zealand? Nutrients 10(11): 1592.
-
Atlantis E, Joshy G, Williams M, Simmons D (2017) Diabetes Among Māori and Other Ethnic Groups in New Zealand. In: Dagogo-Jack S, (Ed.), Diabetes Mellitus in Developing Countries and Underserved Communities, Springer, Switzerland, pp: 165-190.
-
Ni Mhurchu C, Te Morenga L, Tupai-Firestone R, Grey J, Jiang Y, et al. (2019) A co-designed mHealth programme to support healthy lifestyles in Maori and Pasifika peoples in New Zealand (OL@-OR@): a cluster- randomised controlled trial. The Lancet Digital Health 1(6): e298-e307.
-
Theodore R, McLean R, TeMorenga L (2015) Challenges to addressing obesity for Māori in Aotearoa/New Zealand. Australian and New Zealand Journal of Public Health 39(6): 509-512.
-
Popkin BM, Du S, Green WD, Beck MA, Algaith T, et al. (2020) Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships 21(11): e13128.
-
Abdi A, Jalilian M, Sarbarzeh PA, Vlaisavljevic Z (2020) Diabetes and COVID-19: A systematic review on the current evidences. Diabetes research and clinical practice 166: 108347.
-
McLeod M, Gurney J, Harris R, Cormack D, King P (2020) COVID-19: we must not forget about Indigenous health and equity. Australian and New Zealand Journal of Public Health 44(4): 253-256.
-
WHO (2016) Global report on diabetes. World Health Organisation, Geneva, Switzerland.
-
Rao G (2018) Epidemic of Obesity and Diabetes: World Diabetes Day-2018. Diabetes Obes Int J 3(4): 000189.
-
Bullen C, Beaglehole R, Daube AO, Devlin G, Hughes S, et al. (2015) Targets and actions for non-communicable disease prevention and control in New Zealand. The New Zealand Medical Journal 128(1427): 55-60.
-
Lockhart C, Houkamau CA, Sibley CG, Osborne D (2019) To Be at One with the Land: Māori Spirituality Predicts Greater Environmental Regard. Religions 10(7): 427.
-
Glover M, Kira A, Kira G, McRobbie H, Breier BH, et al. (2017) An innovative team-based weightloss competition to reduce cardiovascular and diabetes risk among Māori and Pacific people: rationale and method for the study and its evaluation. BMC Nutrition 3(1): 78.
-
Glover M, Nolte M, Wagemakers A, McRobbie H, Kruger R, et al. (2019) Adherence to daily dietary and activity goals set within a Māori and Pacific weight loss competition. BMC Obes 6(1): 6.
-
Warbrick I, Wilson D, Boulton A (2016) Provider, father, and bro-Sedentary Māori men and their thoughts on physical activity. International Journal for Equity in Health 15(1): 22.
-
Williams M, Cairns S, Simmons D, Rush E (2017) Face-to- face versus telephone delivery of the Green Prescription for Māori and New Zealand Europeans with type-2 diabetes mellitus: influence on participation and health outcomes. The New Zealand Medical Journal 130(1465): 71-79.
-
Sarfati D, McLeod M, Stanley J, Signal V, Stairmand J, et al. (2018) Beta Me: impact of a comprehensive digital health programme on HbA1c and weight at 12 months for people with diabetes and pre-diabetes: study protocol for a randomised controlled trial. Trials 19(1): 161.
-
Oetzel J, Rarere M, Wihapi R, Manuel C, Tapsell J (2020) A case study of using the He Pikinga Waiora Implementation Framework: challenges and successes in implementing a twelve-week lifestyle intervention to reduce weight in Māori men at risk of diabetes, cardiovascular disease and obesity. International Journal for Equity in Health 19(1): 103.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance