Diabetic Awareness Study and Factors affecting it, in Diabetic Patients in Hospital Nakfa, Rural Eritrea
Background: Diabetes mellitus is becoming the most prevailing non-communicable disease creating a burden to the health care system. The objective of this study was to assess awareness regarding diabetes mellitus and factors affecting the awareness levels. Methodology: A Hospital based cross-sectional study was conducted among all diabetic patients in follow-up of Nakfa Hospital. Interviewer administered questionnaire was used as data collection tool. Frequency distribution and tables were used and Independent sample t-tests and one way ANOVA of post hoc tests were used for data analysis. Results: A total of Ninety-two diabetic patients participated in this study. More than half (66.3%) were males with a mean age of 44.5±18.2. Nearly half (47.8%) of them were illiterate and 77.2% were unemployed. The mean scores on general knowledge, diabetic complication knowledge and self-care practice were observed to be 75.4%. Poor score was observed regarding general knowledge and self-care practice, 70.5% and 73.4% respectively. High mean score was observed in complication knowledge, 90.6%. Although being female, illiterate and short duration of illness was associated with low scores but it was not statistically significant. Conclusions: patients showed high mean score in complication knowledge and low scores on general knowledge and self-care practice. Frequent health education programs needs to be increased for better control of the disease and its complications. These results could help the policy makers to implement preventive strategies to prevent the complications and enhance the general knowledge of patients on Diabetes mellitus.
Introduction
Diabetes mellitus is a major clinical and public health problem accounting for 4.6 million deaths annually world- wide [1]. According to the International Diabetes Federation, around 366 million people globally are currently estimated to have diabetes, of which 80% live in low and middle income countries [1]. The more worrisome fact is that about
50% of those with diabetes remain undiagnosed [2, 3]. Education is one of the key components in ensuring better treatment and control of diabetes. There is also evidence to show that increasing knowledge regarding diabetes and its complications has significant benefits including increase in compliance to treatment, thereby decreasing the complications associated with diabetes [4, 5]. If health care providers are aware of the level of awareness in community they can plan their preventive measures accordingly.
Type 2 diabetes mellitus is a global clinical and public health problem with high morbidity and mortality rates, presenting in patients of whom the majority are still economically active. The growing incidence and health implications for those affected make Type 2 diabetes mellitus a major public health issue not only globally, but also in Africa [6].
It is commonly accepted that being knowledgeable, having a positive attitude and following good practices result in the successful management of Type 2 diabetes mellitus. However, Ajzenl, et al. [7] have argued that knowledge is no guarantee for healthy behavior, nor is ignorance necessarily the main cause of unhealthy behavior. Furthermore, knowledge alone is not adequate to bring about behavior change, and various determinants that are often hard and difficult to change influence health behavior [7]. Globally, knowledge related to diabetes management has been found to be insufficient, despite the fact that it is a critical aspect of this condition. In addition, the Knowledge, Attitude and Practice of patients with Type 2 diabetes mellitus have been reported to be poor in areas where the incidence of Type 2 diabetes mellitus is high [8].
To our knowledge there are no studies done on the subject of diabetes awareness in Eritrea. This article focuses on the baseline level of awareness of diabetes mellitus (irrespective of type I and type II) in rural community of Nakfa, Northern Read sea zone, Eritrea. Eritrea as many developing countries of the world is facing the burden of non-communicable diseases as a result of the current epidemiological and nutritional transitions [9, 10]. According to National Health Information System of Eritrea, diabetes mellitus is one of the leading causes of morbidity and mortality mainly in adults; a total of 78,686 new cases and 926 deaths of Diabetes Mellitus were reported from hospitals and health centers in the years 1998 - 2012 [11]. Moreover, 695 amputations due to Diabetes Mellitus were also reported between 2006- 2012 indicating that it is not only leading cause of morbidity but also a cause of disability [12]. The disease leads to high levels of morbidity and mortality and has huge financial impact on individuals and national budgets [13]. Intangible costs (pain, anxiety, inconvenience and generally lower quality of life etc.) also have great impact on the lives of patients and their families and are the most difficult to quantify [2]. It is believed that patient’s knowledge of self-care is the key to achieving therapeutic goals in ambulatory care [14]. Being aware of various aspects of the disease is the first step for primary and secondary prevention. If the health care providers are aware of the level of awareness in community they can plan their preventive measures accordingly [13].
With this background, the current study was planned with the objective of assessing level of awareness regarding various aspects (Knowledge, Self-care practices and Complications) of diabetes mellitus, irrespective of type I or type II, and to assess the factors affecting this level of awareness.
Materials and Methods
A Hospital based cross-sectional study was used to assess the level of awareness among diabetic patients in Nakfa Hospital. All diabetic patients of type I and type II, who attend the diabetic follow-up and agreed to be a part of the study, were included. Awareness regarding diabetes was judged for general knowledge, self-care practices and complications using interviewer administered structured questionnaire. A 23 item questionnaire was adopted, with some modifications, from awareness study conducted by Ashock, et al. [13]. The questionnaire included demographic variables like age, sex, marital status, educational level, occupation, duration of illness, family history of Diabetes Mellitus etc.
Nakfa subzone is one of the most rural parts of Eritrea about 230km north east from the capital city, Asmara. It is a highland area, about 2300kms above sea level; most of its land is covered by mountains. Its population size reaches about 45,000 [source: Nakfa administration, 2017], most of them live by livestock breeding and has nomadic life style. There is one Hospital and two health stations in Nakfa subzone. There were 106 diabetic patients who were in regular follow up in the hospital, but 14 patients had lost from follow up during the data collection time_._ The study was carried out from January to October 2017. Ethical approval was obtained from the Research Review and Ethical Clearance Committee of the Ministry of Health of Eritrea. Written informed consent of 92 diabetic patients was taken before starting the research. The time taken to complete each questionnaire ranges 15 to 20 minutes and the responses were in the format of Yes, No, and don’t know. These were analyzed as correct, don’t know and wrong, and were scored as 2, 1, 0 points respectively. Frequency distribution and tables to see the scores against the variables and cross-tabulation analysis to determine the factors affecting the scores were used. Data was analyzed using SPSS
version 20. Independent sample t-tests and one way ANOVA of post hoc tests were used for data analysis. P-value <0.05 was considered as significance level.
Results
A total of Ninety-two diabetic patients participated in this study. More than half (66.3%) were males and the mean age of the participants was 44.5±18.2 years. Nearly half (47.8%) of the participants have not attended any formal educational and three-fourth (77.2%) of them were unemployed.
The mean scores on all three aspects (diabetic knowledge, self-care practice and diabetic complication knowledge) were observed to be 75.4%. Poor score was observed regarding general knowledge and self-care practice, 70.5% and 73.4% respectively. While Awareness about HbA1c and importance of physical exercise and diet was observed to be low, only 29(31.5%) of them were aware about HbA1c and only 15((16.3%) knows that physical exercise and diet is as important as the diabetic medications. Some of responses to selected questions are discussed below (Table 1).
| Questions | Yes (%) | No (%) | I don’t Know (%) | |
|---|---|---|---|---|
| 1 | Are you aware about HbA1c? | 29(31.5) | 37(40.2) | 26(28.3) |
| 2 | A fasting blood sugar level of 210 is too high? | 75(81.5) | 4(4.3) | 13(14.1) |
| 3 | Diabetes can be cured? | 18(19.6) | 59(64.1) | 15(16.3) |
| 4 | Tight elastic shoes or socks are not good for diabetics? | 80(87) | 4(4.3) | 8(6.7) |
| 5 | Have you ever forgotten to take your medication? | 15(16.3) | 76(82.6) | 1(1.1) |
| 6 | Do you do regular physical exercise? | 55(59.8) | 37(40.2) | |
| 7 | Medication is more important than diet and exercise to control my diabetes? | 63(68.5) | 15(16.3) | 14(15.2) |
| 8 | Unmanaged diabetes can cause eye problems? | 81(88) | 8(8.7) | 3(3.3) |
| 9 | Poorly controlled diabetes can affect your kidneys? | 80(87) | 4(4.3) | 8(8.7) |
| 10 | Unmanaged diabetes can cause heart diseases? | 78(84.8) | 0(0) | 14(15.2) |
Table 1: Responses to selected questions from the questionnaire (n=92).
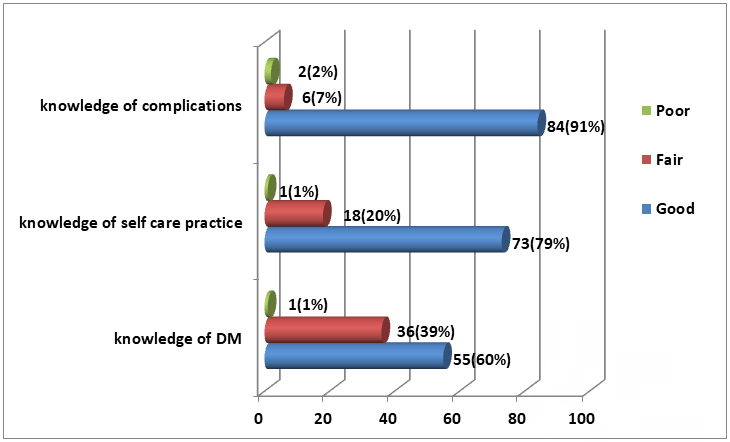
Awareness scores based on correct responses on various aspects of Diabetes Mellitus and the details of the scoring system and distribution of the respondents according to it is shown on the table 2. Out of the total 92 diabetic patients,
55(59.8%) had good knowledge of Diabetes Mellitus, 73 (79%) were well aware of self-care practices and 84(91.3%) knew about the complications (Table 2).
| Category | No(%) n=92 | |
|---|---|---|
| Knowledge of diabetes among study group | Good (Score 14-20) | 55(59.8%) |
| Knowledge of diabetes among study group | Fair (Score 7-13) | 36(39.1%) |
| Knowledge of diabetes among study group | Poor (Score 0-6) | 1(1.1%) |
| Knowledge of self-care practice | Good (Score 12-18) | 73(79%) |
| Knowledge of self-care practice | Fair (Score 6-11) | 18(19.6%) |
| Knowledge of self-care practice | Poor (Score 0-5) | 1(1.1%) |
| Knowledge of Complications | Good (Score 6-8) | 84(91.3%) |
| Knowledge of Complications | Fair (Score 3-5) | 6(6.5%) |
| Knowledge of Complications | Poor (Score 0-2) | 2(2.2%) |
Table 2: Distribution of respondents according awareness score.
Comparison of Awareness Score with Demographic Variables
Those who didn’t have health education in the last 3 months and those who are single had significantly lower overall scores (t= 2.69, p= 0.008) and (F= 3.77, P= 0.027) respectively. Although being female, illiterate and short duration of illness was associated with low scores but it was not statistically significant (p= 0.08, p= 0.81, p=0.79) respectively. Age and type of diabetes has no association in the score (Table 3).
| Characteristics | Category | Frequency (%) | Mean Score SD | |
|---|---|---|---|---|
| 1 | Age (years) | <30 | 24 (26.1) | 26.91±5.45 |
| 1 | Age (years) | 30-45 | 22 (23.9) | 27.22±4.46 |
| 1 | Age (years) | 46-60 | 27 (29.3) | 27.37±4.28 |
| 1 | Age (years) | >60 | 19 (20.7) | 27.36±3.70 |
| F= 0.75, P= 0.53 (One way ANOVA) | ||||
| 2 | Sex | Male | 61(66.3) | 27.34±4.26 |
| 2 | Sex | Female | 31(33.7) | 25.58±4.88 |
| t= 1.78, p= 0.08 (independent sample t-test) | ||||
| 3 | Marital Status | Single | 18(19.5) | 24.22±5.30 |
| 3 | Marital Status | Married | 67(72.8) | 27.30±4.12 |
| 3 | Marital Status | Divorced | 7(7.6) | 28.00±4.62 |
| F= 3.77, P= 0.027 (One way ANOVA)* | ||||
| 4 | Occupation | Employed | 21(22.8) | 27.05±3.54 |
| 4 | Occupation | Unemployed | 71(77.2) | 26.66±4.81 |
| t= 0.34, p= 0.73 (independent sample t-test) | ||||
| 5 | Educational Level | Illiterate | 44(47.8) | 26.43±4.31 |
| 5 | Educational Level | Elementary | 20(21.7) | 27.15±5.25 |
| 5 | Educational Level | Junior and Above | 28(30.4) | 26.96±4.46 |
Table 3: comparison of awareness score with demographic variables. * = p<0.05
- F= 0.21, P= 0.81 (One way ANOVA)
- 6
- Family History of Diabetes
- Yes
- 21(22.8)
- 28.05 ± 4.10
- No
- 71(77.2)
- 26.37 ± 4.61 t= 1.50, p= 0.14 (independent sample t-test)
- 1-5 years
- 46(50)
- 25.83 ± 4.25
- 5-10 years
- 18(19.6)
- 27.50 ± 4.57
- > 10 years
- 20(21.7)
- 28.70 ± 4.53
- F= 2.33, P= 0.79 (One way ANOVA)
- 7
- Duration of Illness
- 8
- Health Education in the last 3months yes
- 50(54.3)
- 28.09 ± 4.02
- No
- 42(45.7)
- 25.62 ± 4.67 t= 2.69, p= 0.008 (independent sample t-test)*
- 9
- DM Type
- Type I DM
- 36(39.1)
- 26.83 ± 5.06
- Type II DM
- 56(60.9)
- 26.69 ± 4.21 t=.14, p= 0.889 (independent sample t-test)
Table 4: comparison of awareness score with demographic variables.
Discussions
The mean scores on all three aspects were observed to be 75.4%. Poor score was observed regarding general knowledge and self-care practice, 70.5% and 73.4% respectively. High mean score was observed in complication knowledge, 90.6%. Similar to study done in India by Ashock, et al. awareness regarding foot care, ophthalmic, renal and cardiac complications was observed to be high 90.2%, 89.1%, 87%, 85.1% respectively [13].
Despite the rising epidemic of diabetes mellitus and other non-communicable diseases [15], the study shows that there is a decreased awareness regarding all the aspects of diabetes mellitus, especially regarding the general knowledge (59.8%). This study results were almost similar to other studies that 62% [16], 61.41% [17] and 52.5% [18] had a good knowledge respectively, and composite knowledge score was (56.5-70.1%) [19]. But the study results was lower when compared studies in Ethiopia (93.7%) [20] and India (71.9%) [21]. Moreover; this finding was higher to studies in Ethiopia (49%) [22], Sudan (15%) [23] and Malaysia (41.9%) [24].
This result could be explained that patients may not get appropriate health education during their regular follow up by the health professionals and; other social factors as their level of education may have a contributing factor for the low knowledge score; thus community awareness campaigns are highly essential to control the increasing burden of the disease. Most patients (60.9%) had type two diabetes mellitus. This also coincides with their poor knowledge score that they may not apply the preventive measures of the risk factors for diabetes mellitus type two. This needs to aware the community about the risk factors and life style modification to prevent further burden of the disease in the population.
The composite score of Self-care practice was slightly low (79%). This finding was lower compared to the studies conducted in South Africa (99%) [25], and almost similar to 74.4% showed good practice towards glycemic control [16]. Compared to other studies, this was higher to study in Harar, Ethiopia, in which 39.2% had good self-care practice [26] and the levels of patients’ good practice were 52.23% [17]. About 48.4% of the diabetic respondents were not aware of self-care in diabetes [27]. Study by Kaur in Chandigarh observed that 63.3% of them were poor in practicing foot care [28]. Even though patients have low knowledge score they had higher score on self-care practices mainly due to the input of the physicians was high on preventing complications and educating patients on self-care practices.
This study also showed that a high score (91.3%) was observed about the complications of Diabetes mellitus. This was higher to other studies that, 72.7% diabetic population knew that diabetes could affect other organs [19] and 74.2% of diabetics were aware of the complications [27]. Deepa Mohan, et al. in Chennai observed that even among self-reported diabetic subjects, knowledge about diabetes including awareness of complications of diabetes was poor [2]. This result showed that the focus of health education of the health professionals were mainly on the diabetic complications.
Scores of those who had diabetic health education in the last 3months was significantly higher than the others, and those who didn’t have health education in the last 3 months and those who are single had significantly lower overall scores. In similar study conducted in Saudi Arabia, health education and age were found to be the most important predictors of knowledge [29]. This brings to attention the role of health care providers in health education of their patients and the general community, about diabetes and other chronic diseases.
The study was not without limitations. Study participants number was very small; in addition to this medication knowledge and usage was not assessed.
Conclusion
This study showed that patients reported high mean score in complication knowledge but low scores on general knowledge and self-care practice. Most of the patients had type two diabetes mellitus which overlaps with their poor knowledge score. Majority of the patients were illiterate and unemployed which could have an impact in the low knowledge score results.
Enhancing awareness of diabetes will play a great cost effective role in prevention and control of the disease. To raise the awareness of diabetes, a formal, structured approach should be designed to deliver the necessary educational information to diabetic patients and the general population, through mass media and outreach health education programs. Our current educational system mostly focuses on the complications of diabetes, knowing the complications will not stop it from happening. Special emphasis should be given to the areas of low scores; these are general knowledge and self-care practice.
Declarations
Acknowledgment
Authors are thankful to all data collectors and participants for their interest to participate in the study.
Funding
There was no any source of funding for this research
Conflicting Interests
The authors declared that they had no conflicts of interests to disclose.
Availability of Data and Material
Supplementary materials can be requested from the corresponding author if needed
Consent to Participate
Study participants have signed written consent before participation in the study
Consent for Publication
All authors have approved the manuscript for publication, but consent was not applicable
Ethical Approval
Ethical approval was obtained from the Ministry of Health Research ethical and clearance Review Committee of Eritrea and written informed consent was obtained from the study participants. Personal information data of patients was kept secured.
Authors’ Contribution
YK and BT designed the study. All authors reviewed the protocol and YK, BT, and MY finalized the draft data collection tools. All authors participated in the data collection and data entry. AK designed the data entry tools and analyzed the data. All authors contributed in analysis and writing the manuscript and the last version of the manuscript was done by YK and BT. Finally, all authors reviewed and approved the final manuscript.
References
-
Unwin N, Whiting D, Guariguata L, Ghyoot G, Gan D (2011) Diabetes Atlas. 5th (Edn.), Brussels, Belgium: International Diabetes Federation, pp: 11-74.
-
Mohan D, Raj D, Shanthirani CS, Datta M, Unwin NC, et al. (2005) Awareness and knowledge of diabetes in Chennai – The Chennai Urban Rural Epidemiology Study [CURES-9]. J Assoc Physicians India 53: 283-287.
-
Harris MI, Eastman RC (2000) Early detection of undiagnosed diabetes mellitus: A US perspective. Diabetes Metab Res Rev 16(4): 230-236.
-
Visser A, Snoek F (2004) Perspectives on education and counseling for diabetes patients. Patient Educ Couns 53(3): 251-255.
-
Rani PK, Raman R, Subramani S, Perumal G, Kumaramanickavel G, et al. (2008) Knowledge of diabetes and diabetic retinopathy among rural populations in India, and the influence of knowledge of diabetic retinopathy on attitude and practice. Rural Remote Health 8(3): 838.
-
Roux ML, Walsh C, Reid M, Raubenheimer J (2019) Diabetes-related knowledge, attitude and practices (KAP) of adult patients with type 2 diabetes mellitus in the Free State province, South Africa. South African Journal of Clinical Nutrition 32(4): 83-90.
-
Ajzen I, Joyce N, Sheikh S, Cote NG (2011) Knowledge and the prediction of behavior: the role of information accuracy in the theory of planned behavior. Basic ApplSoc Psych 33(2): 101-117.
-
Upadhay DK, Palaian S, Shankar PR, Mishra P (2007) Knowledge, attitude and practice about diabetes among diabetes patients in Western Nepal. Rawal Med J 33(1): 1-9.
-
Mufunda J, Nyarango P, Kosia A, Obgamariam A, Mebrahtu G, et al. (2005) Noncommunicable diseases in Africa: a silent hypertension epidemic in Eritrea, J Hum Hypertens 19(3): 255-256.
-
Usman A, Mebrahtu G, Mufunda J, Nyarango P, Hagos G, et al. (2006) Prevalence of non-communicable disease risk factors in Eritrea, Ethnicity and disease 16(2): 542- 546.
-
Adgoy ET, Seyoum Y, Andemariam Z, Habtemariam R, Gebremichael H (2016) Diabetic complications among adult diabetic patients; Halibet regional referral hospital ZobaMaekel, Asmara, Eritrea. International Journal of Medicine and Health Profession Research 3(2): 82-91.
-
Ministry of Health Eritrea M (2012) National STEPS Survey for Chronic Non Communicable Diseases and their Risk Factors. DPC/NCD.
-
Vankudre AJ, Padhyegurjar MS, Jennifer HG, Padhyegurjar SB (2013) A study to assess awareness regarding Diabetes Mellitus and factors affecting it, in a tertiary care hospital in Kancheepurum District healthlinep 4(2): 44-49.
-
Adibe MO, Aguwa CN, Ukwe CV, Okon JM, Udeogaranya OP (2009) Diabetes self-knowledge among type 2 diabetic Outpatients in south-eastern nigeria. Int J Drug Dev & Res 1(1): 85-104.
-
Dalal S, Beunza JJ, Volmink J, Adebamowo C, Bajunirwe F, et al. (2011) Non-communicable diseases in sub-Saharan Africa: what we know now. International Journal of Epidemiology 40(4): 885-901.
-
Asmelash D, Abdu N, Tefera S, Baynes HW, Derbew C (2019) Knowledge, Attitude, and Practice towards Glycemic Control and Its Associated Factors among Diabetes Mellitus Patients. Journal of Diabetes Research 2019: 2593684.
-
Niroomand M, Ghasemi SN, Sari HK, Ardebili SK, Amiri P, et al. (2016) Diabetes knowledge, attitude and practice (KAP) study among Iranian in-patients with type- 2 diabetes: A cross-sectional study. Diabetes Metab Syndrome 10(1): S114-S119.
-
Kassahun CW, Mekonen AG (2017) Knowledge, attitude, practices and their associated factors towards diabetes mellitus among non-diabetes community members of Bale Zone administrative towns, South East Ethiopia. A cross-sectional study. PLoS One 12(2): e0170040.
-
Deepa M, Bhansali A, Anjana RM, Pradeepa R, Joshi SR, et al. (2014) Knowledge and awareness of diabetes in urban and rural India: The Indian Council of Medical Research India Diabetes Study (Phase I): Indian Council of Medical Research India Diabetes. Indian J Endocrinol Metab 18(3): 379-385.
-
Berhe K, Gebru H, Kahsay H, Kahsay A (2014) Assessment of diabetes knowledge and its associated factors among type 2 diabetic patients in Mekelle and Ayder Referral Hospitals, Ethiopia. Journal of Diabetes & Metabolism 5(5): 1000378.
-
Saadia Z, Rushdi S, Alsheha M, Saeed H, Rajab M (2010) A study of knowledge attitude and practices of Saudi women towards diabetes mellitus. A (KAP) study in Al- Qassim region. The Internet Journal of Health 11(2): 1-7.
-
Asmamaw A, Asres G, Negese D, Fekadu A, Assefa G (2015) Knowledge and attitude about diabetes mellitus and its associated factors among people in DebreTabor town, Northwest Ethiopia: cross sectional study. Science Journal of Public Health 3(2): 199-209.
-
Balla SA, Ahmed HA, Awadelkareem MA (2014) Prevalence of diabetes, knowledge, and attitude of rural, population towards diabetes and hypoglycaemic event, Sudan 2013. American Journal of Health Research 2(6): 356-360.
-
Minhat HS, Hamedon TR (2014) Understanding towards diabetes mellitus among rural adult community in Malaysia. World Journal of Medical Sciences 11(2): 217- 221.
-
Ikombele B (2011) Knowledge, attitudes and practices regarding lifestyle modifications among type 2 diabetic patients attending Mamelodi Hospital, Pretoria, South Africa. University of Limpopo, Medunsa Campus.
-
Ayele K, Tesfa B, Abebe L, Tilahun T, Girma E (2012) Self- care behavior among patients with diabetes in Harari, Eastern Ethiopia: the health belief model perspective. PLoS One 7(4): e35515.
-
Muninarayana C, Balachandra G, Hiremath SG, Iyengar K (2010) Prevalence and awareness regarding diabetes mellitus in rural Tamaka, Kolar. Int J Diabetes Dev Ctries 30(1): 18-21.
-
Kaur K, Singh MM, Kumar, Walia I (1998) Knowledge and self-care practices of diabetics in a resettlement colony of Chandigarh. Indian J Med Sci 52(8): 341-347.
-
Aljoudi AS, Taha AZ (2009) Knowledge of diabetes risk factors and preventive measures among attendees of a primary care center in eastern Saudi Arabia, Ann Saudi Med 29(1): 15-19.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance