Dyslipidaemia of Alloxan-Induced Type 1 Diabetes Mellitus in Dogs is attenuated by Ethanolic Extracts of Anogeissus Leiocarpus Stem Bark
Introduction: The effect of ethanolic extract of Anogeissus leiocarpus stem bark on dyslipidaemia induced by diabetes mellitus (DM) was investigated, since enhanced pro-synthetic hypoglycaemic drugs did not effectively control dyslipidemia of DM, apart from causing toxicity and resistance. Materials and Methods: Twelve adult Nigerian indigenous dogs were placed in 4 groups of 3 each, namely non diabetic (ND); diabetic untreated (DU); diabetic treated with insulin (DI) and diabetic treated with extract (DE). Body weights and lipid profiles were measured during a four-week period. Results: Significant percentage body weight decreased in DU (50.21 %) throughout the period of study with continuous increase in body weight in ND (46.96 %). In DI and DE there were initial decreases in body weights (11.08% and 14.54% respectively) which significantly increased (23.53 % and 32.30 % respectively) by the fourth week. Lipid profiles revealed significant (P < 0.002) increases in triglycerides, total cholesterol and low-density lipoproteins (LDL) in DU group when compared with the DE group. There was also a significant (P < 0.002) decrease in high density lipoprotein (HDL) in the DU when compared to DE, DI and ND groups. Conclusion: The ethanolic extract of Anogeissus leiocarpus stem bark attenuated the dyslipidaemia produced in alloxaninduced type 1 diabetes mellitus in Nigerian indigenous dogs.
Introduction
Diabetes mellitus (DM) a metabolic disease, from disorders of carbohydrate, protein and lipid metabolism [1, 2, 3, 4]. DM was the most common noncommunicable disease afflicting over 425 million people worldwide [5, 6] and might become the 7th leading cause of death with worse projections for 2035 [6], making DM a challenging unresolved health problem for the 21st century [7]. The worrisome nature of DM on the national budgets of countries worldwide, was provided by an assessment of outpatient visits between 2007 and 2013 in the United States alone, which showed 785 million people with diabetes [8, 9]. Diabetes became more worrisome due to its risk factor for the progression, prognosis and mortality of COVID-19 [10, 11], in particular, COVID-19 patients with pre-existing type 2 diabetes [12] and the global economic implications.
Obesity, a predisposing factor, amongst others, of diabetes mellitus and the excess body weight with physical inactivity creates long-term damage caused by chronic hyperglycaemia and then dysfunction and failure of various organs, the eyes, nerves, heart, blood vessels and kidneys with diabetic nephropathy being one of the three major microangiopathies of diabetes mellitus which occurred in approximately 30% of type 2 DM (T2DM) patients [13].
The underlying DM disease promoting factors are lack or inherited and/or acquired deficient production of insulin by ß-cells of the pancreas, which is type 1 diabetes mellitus (TIDM) or ineffectiveness, unresponsiveness and/or resistance of the insulin produced by the target organs and tissues [14, 15] which is type 2 diabetes mellitus (T2DM).
The pathophysiological outcome is a derangement of insulin-mediated intracellular glucose transport for energy production and chronic hyperglycaemia develops. Diabetic patients resort to lipid metabolism as an alternative source of energy with occurrence of disorders of lipid and lipoprotein metabolism in diabetic patients [15].
In poorly controlled type 1 diabetes ketoacidosis, hypertriglyceridaemia and reduced high density lipoprotein (HDL) occurred [16]. Defects in insulin action and consequent hyperglycaemia led to changes in plasma levels of lipoproteins in patients with diabetes [17]. These lipid abnormalities arising from insulin resistance increased free fatty acids from the adipose tissue and caused increased hepatic uptake of free fatty acids for increased synthesis of triglycerides, triglycerides synthesis which stimulated the production of very low density lipoproteins (VLDL) and subsequent production of small low density lipoproteins (LDL) [18, 19, 20, 21]. Low-density lipoprotein (LDL)-cholesterol (C) was reported as the most important risk factor for atherosclerotic cardiovascular disease (CVD) such as coronary artery diseases [18]. Good glycemic control had been reported to improve dyslipidaemias in diabetes mellitus [22, 23, 24]. High prevalence of dyslipidaemias in type 1 diabetes was associated with Poor glycemic control [25].
Insulin had long remained a conventional treatment for diabetes mellitus; it is usually injectable and usually its withdrawal causes a rebound hyperglycaemia. This has stimulated numerous researches for a non-conventional treatment for diabetes mellitus.
Sulfoylurea and meglitinides biguanides and thiazolidinediones [26, 27, 28], which are enhanced pro- synthetic hypoglycaemic drugs, used to control DM, did not effectively control hyperlipidaemia and caused toxicity and development of resistance in some individuals [29, 30, 31]. Due to the development of these therapies along allopathy principles, they were often too costly and out of reach of patients from developing countries [32, 33], disadvantages that prompted some patients to abandon these medications [34]. Thiazolidinediones may increase HDL and LDL levels, but the long-term effect of such changes was not known [35]. It was reported that medical interventions targeted at improving glycemia only lowered triglyceride levels modestly and had no effect or minimal effects on HDL levels.
Medicinal plants were more affordable and had less side effects compared with synthetic drugs, and effective in treatment of diabetes mellitus [30, 36]. The effects of medicinal plants on dyslipidaemia of experimentally induced diabetes showed that some medicinal plants including, Veronia amygdalina, Ficus sur, and alfalfa extracts [37, 38, 39] ameliorated the dyslipidaemias in diabetic animals. While probiotics and vitamin C ameliorated dyslipidaemia in alloxan-induced diabetes mellitus in Wistar rats [21], peels of Musa cavendish fruit suppressed dyslipidaemia in alloxan- induced diabetic rats [40] and Tinospora cordifolia sterm bark extract also had antidyslipidaemia effect in alloxan-induced diabetic rats [15]. Anogeissus leiocarpus, a medicinal tree which is widespread in Africa has been reported to possess hypoglycemic effect, stimulating effect on erythropoiesis and protected red blood cell membranes, [41]; and produced numerous healing advantages in alloxan-induced diabetes mellitus in dogs [36]. This study was designed to evaluate the effects of Anogeissus leiocarpus on lipid profiles in experimentally alloxan-induced diabetes mellitus type 1 in Nigerian indigenous dogs, and the antidyslipidaemic effects are reported herein.
Materials and Methods
Experimental Animals
Twelve apparently healthy adult Nigerian indigenous dogs of both sexes were sourced around Zaria and environs were kept in the arthropod-proof Animal Pen (with ambient temperature and humidity) of the Department of Veterinary Parasitology and Entomology Faculty of Veterinary Medicine, Ahmadu Bello University, Zaria. Their standardized dog food was made of 60 % carbohydrate, 25 % protein and 15 % fat; fresh clean water provided ad libitum. The dogs were weighed and colour-coded for easy identification. Endo- and ectoparasites were treated using Prazisam® plus (praziquantel 50 mg, pyrantel pamoate 144 mg and fenbendazole 500 mg. (Vetoquinol India Animal Health Pvt Ltd 801, Sigma, 8th Floor) at an oral dose of 1 tablet per 10 kg body weight orally as recommended by the manufacturers and Ivermectin at a dose of 100 µg/kg body weight subcutaneously. The animals were further screened to eliminate the presence of any disease. They were also vaccinated against rabies using the dog antirabies vaccine obtained from Nigeria Veterinary Research Institute, Vom, Plateau State Nigeria. The dogs were allowed to acclimatize and for a period of one month before commencement of the experiment.
Experimental Dog Groups
The animals were weighed and assigned at random into 4 groups of three dogs each; as described earlier Esievo, et al. [42] and summarized below: Group 1 (ND): Without diabetes, administered normal saline orally at a dose of 2 ml/kg/body weight daily and served as normal control. Group 2 (DU): Diabetes was induced, left untreated and served as negative control. Group 3 (DI): Diabetes induced and insulin-treated at a dose of 0.5 IU/kg body weight, was administered subcutaneously daily and served as positive control. Group 4 (DE): Diabetes induced and crude ethanolic extract of Anogeissus leiocarpus at a dose of 1000 mg/kg body weight was administered orally, daily. The dose of extract was selected based on previous studies by Num, et al. [41].
The crude ethanol extract was reconstituted by dissolving 1 g of extract in 2.5 ml distilled water to obtain a concentration of 400 mg/ml. All administrations were given at 9:00 am daily for three weeks.
Feeding Regime, Measurements of Body Weights and Weight Changes
They were fed on standardized dog food of 60 % carbohydrate, 25 % protein, 15 % fat and provided fresh clean water ad libitum. The dogs were fed once daily at a rate of 300 g per dog in the ND group, 350 g per dog in the DU group, 300 g per dog in the DI group and 250 g per dog in the DE group. Weights were measured at weekly intervals and percentage weight changes were calculated using the formula:
grams lost % wt loss= ×100 starting weight grams gained % wt gain= ×100 starting weight
Evaluation of the Experimental Dogs Pre- induction of Diabetes Mellitus
Five (5) mL of blood samples were collected a day before commencement of the experiment to screen for other diseases and to obtain baseline haematological, serum biochemical and lipid profiles. Intravenous glucose tolerance test was conducted to rule out the possibility of pre-existing diabetes. The dogs were also weighed and the vital parameters including heart rate, respiratory rate and temperature were taken for each animal before commencement of test to ensure they were in apparently healthy condition. Induction of diabetes mellitus with alloxan monohydrate: Diabetes mellitus was induced using alloxan monohydrate (Sigma- AldrichTM) to produce type 1 diabetes. The dogs in groups 2, 3 and 4 were fasted overnight. Blood glucose level was measured at 0 minute using an Accu-Chek® Active portable glucometer and test strip. Alloxan monohydrate was reconstituted in cold normal saline to obtain a concentration of 200 mg/ml and administered rapidly through the saphenous vein at a dose rate of 100 mg/kg body weight. The dogs were maintained on 10 % dextrose to prevent fatal hypoglycaemia and monitored continuously for fatal clinical signs. They were provided with food and water during the whole period. Fasting blood glucose (FBG) were tested 72 hours, 7 and 14 days after the alloxan administration. Dogs having elevated glucose levels (6.3-8.3 mmol/L) were considered diabetic. Collection of serum samples: Five (5) mL of blood Serum samples were collected at 9:00 am at weekly intervals for the haematological and serum biochemical analysis. The area of the saphenous vein was sterilized with 10 % chlorhexidine and 3 ml of the collected blood were dispensed into anticoagulant free vacutainers. The blood was allowed to clot, rimmed and then centrifuged at 1000 x g for 3
minutes to separate the serum. The serum was aspirated into serum tubes and transported immediately to the Chemical Pathology Laboratory of the Ahmadu Bello University, Zaria Teaching Hospital for analysis of the serum biochemical profile. Assay of Serum Total Cholesterol And Triglyceride: Total cholesterol (TC), high-density lipoprotein (HDL) and triglyceride (TG) were determined by colorimetric method [43, 44] using enzymatic diagnostic kits (AGAPPE Diagnostic Switzerland GmbH) as applied by Aluwong, et al. [21]. Low- density lipoprotein (LDL) was calculated using the formula, LDL = Total cholesterol - HDL- triglyceride/s [45]. All these analyses conformed with the various Bayer diagnostic reagents as approved by the International Federation of Clinical Chemistry-IFCC.
Plant Collection and Preparation
The leaves, stem bark and roots of Anogeissus leiocarpus were collected from ‘Area G’ Staff quarters of Ahmadu Bello University (ABU) Samaru Zaria in the month of December, and authenticated in the herbarium of the Department of Botany, Faculty of Life Sciences, Ahmadu Bello University, Zaria, where a voucher sample (number167) was deposited. The stem bark, which was used for the study, it was air dried for about two weeks under shade at room temperature and pulverized using mortar and pestle. Crude Ethanol Extraction of Stem Bark of A. leiocarpus: Crude ethanol extract of the plant was obtained using the cold maceration method with 95 % v/v ethanol as described by Num, et al. [41]. Qualitative Phytochemical Screening of Crude Ethanol Extract of Anogeissus leiocarpus: Standard protocols [46, 47] were used in detecting the presence of different phytochemical constituents in the crude ethanol extract. Quantitative Phytochemical Screening of Crude Ethanol Extract of Anogeissus leiocarpus: The percentage yield of alkaloids, flavonoids, saponins, tannins and phenols in the crude extract were determined using standard procedures as described by Harbone [48], Bohm and Koupai-Abyazani [49], Obadoni and Ochuko [50], and Van-Burden and Robinson [51] respectively.
Statistical Analysis
The data obtained from this study were subjected to student t-test and presented in figure, tables, and means ± SEM and further subjected to ANOVA using the GraphPad Prism® statistical package and Tukey’s post-hoc tests; values of p<0.05 were significant.
Results
The composition of ethanolic extract of A. leiocarpus was reproduceable and adequately presented earlier [36, 41, 42].
The animals did not exhibit any side-effects with the administration of the ethanolic extract of the plant.
The blood glucose values and other clinical biochemical parameters of the treatment group were adequately presented in earlier publications [36, 42].
Effects of Administrations of Insulin and Crude Ethanol Extract of A. leiocarpus on Weights of Alloxan-induced Diabetic Dogs
The results for body weight changes of dogs over a period of four weeks are shown in table 1. In the normal control group (ND), the percentage weight gain increased from by 21.64 % in the first week to 46.96 % by the fourth week, while in the diabetic group (DU) the weights continuously decreased from 16.93 % in the first week to 50.21 % by the fourth week. In the insulin group (DI) and extract group (DE), there was an initial decrease in weights by 11.08 % (DI) and 14.54 % (DE) by the first week respectively but by the fourth week, the weights increased by 23.53% (DI) and 32.30% (DE) respectively.
| ND (kg) | DU(kg) | DI (kg) | DE (kg) | |
|---|---|---|---|---|
| Week 0 | 10.03 | 12.05 | 10.2 | 9.01 |
| Week 1 | 12.20 (21.64%)a | 10.01 (16.93%)a | 9.07 (11.08%)a | 7.7 (14.54%)a |
| Week 2 | 14.25(42.07%)a | 7.03 (41.66%)a | 8.90 (12.75%)b | 6.86 (23.86%)b |
| Week 3 | 14.50 (44.57%)b | 7.01 (41.81%)a | 9.30 (8.2%)b | 8.75 (2.89%)b |
| Week 4 | 14.74(46.96%)a | 6.0 (50.21%)a | 12.60 (23.53%)a | 11.92 (32.30%)a |
| ND | DU | DI | DE | |
| TC (mmol/L) | 3.1 ±0.08 | 6.6 ±0.12 | 3.4 ±0.53 | 3.02 ±0.45 |
| HDL (mmol/L) | 1.2 ±0.01 | 0.2 ±0.17 | 1 ±0.15 | 1.28 ±0.31 |
| LDL (mmol/L) | 2.7 ±0.14 | 5.8 ±0.23 | 2.9 ±0.57 | 1.4 ±0.50 |
| TG (mmol/L) | 1.5 ±0.01 | 3 ±0.29 | 1.8 ±0.40 | 1.54 ±0.38 |
Table 1: Lipid profiles in dogs.
ab= P < 0.05, ND = Non-diabetic (control), DU = Untreated diabetic, DI = Diabetic insulin treated, DE= Diabetic extract treated. Table 1: Percentage weight changes in dogs.
The emphasis on this aspect of obesity is the “percentage weight changes” as the study progressed, in relation and in association with the main issue, the lipid profiles.
ND = Non diabetic, DU= Diabetic untreated, DI = Diabetic insulin treated, DE = Diabetic extract treated, TC = Total cholesterol, HDL = High density lipoprotein, LDL = Low density lipoprotein, TG = Triglyceride. Table 2: Lipid profiles in dogs.
Effects of the Administrations of Insulin and Crude Ethanol Extract of A. leiocarpus on Lipid Profiles in Alloxan-Induced Diabetes Mellitus in Dogs
The effects of the administrations of insulin and crude ethanol extract of A. leiocarpus on lipid metabolism profiles in Alloxan-Induced diabetes mellitus in dogs (Figure 1).
In dogs, there was a significant increase (P < 0.002) in triglycerides, total cholesterol and low density lipoprotein (LDL) in the diabetic untreated group (DU) when compared to the diabetic extract treated group (DE). There was also a significant decrease in high density lipoprotein (HDL) (P < 0.002) in untreated diabetic groups when compared to the control dogs, insulin treated diabetic dogs and the extract treated dogs.
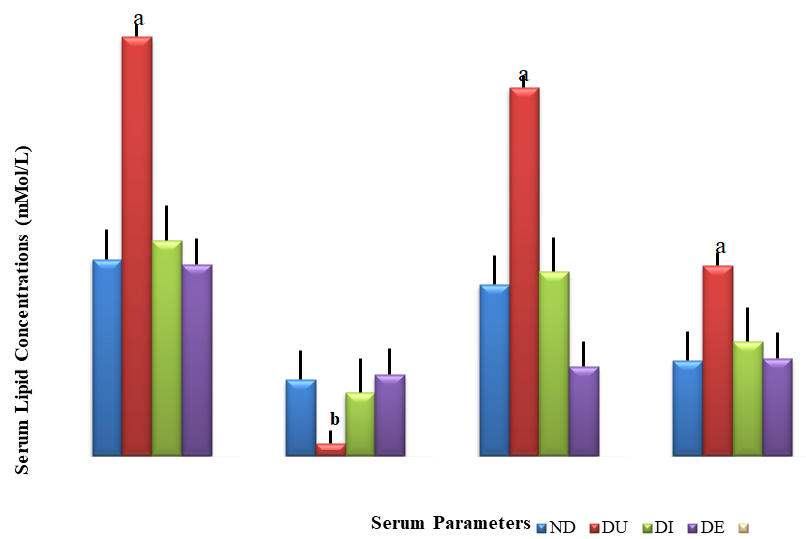
a = P<0.05, b= P<0.002, ND = Non diabetic, DU= Diabetic untreated, DI = Diabetic insulin treated, DE = Diabetic extract treated, TC = Total cholesterol, HDL = High density lipoprotein, LDL = Low density lipoprotein, TG = Triglyceride. Figure 1: Effects of administrations of insulin and crude ethanol extract of A. leiocarpus on lipid profiles of alloxan-induced diabetic dogs.
Discussion
The body weight variations were observed at the beginning and end of the research showed that diabetes mellitus caused decrease in body weights whereas the decrease in body weights initially observed in the DI and DE groups were ameliorated and greatly increased by the fourth week. This increase was even higher in the DE group when compared to DI. Num, et al. [41] reported a higher percentage weight gains in normoglycaemic Wistar rats treated with extracts of A. leiocarpus which was attributed to phytochemicals like flavonoids.
In the current study, there was a significantly higher level of triglycerides, total cholesterol and low density lipoprotein (LDL) in the diabetic untreated group (DU) when compared to the diabetic extract treated group (DE). There was also a significantly lower level of high density lipoprotein (HDL) in untreated diabetic groups when compared to the control group, insulin treated diabetic group and the extract treated groups. This is agreed with the reports of Akah, et al. [37], Akomas, et al. [38], and Farsani, et al. [39] on their similar studies in diabetic rats. Diabetes mellitus was extremely associated with impaired lipid metabolism resulting in high level of total cholesterol, triglycerides and abnormalities in serum lipoproteins [52]. The idea that high cholesterol levels in the blood are the main cause of CVD is debatable because people with low levels become just as atherosclerotic as those with high levels and their risk of suffering from CVD is the same or higher [53]. Hypertriglyceridaemia and reduced HDL commonly occured in type1 diabetes or even ketoacidosis [16, 54]. Factors responsible for dyslipidaemia in diabetes included: insulin’s effects on liver apoprotein B (apoB) production, regulation of lipoprotein lipase (LpL), actions of cholesteryl ester transfer protein (CETP), and peripheral actions of insulin on adipose and muscle [17]. Increase in fatty acid transport to the liver, a common abnormality seen in insulin-resistant diabetes, caused an increase in LDL secretion suggesting that fatty acids modulate liver apoB secretion [55, 56, 57]. Insulin directly increases degradation of newly synthesized apoB [58], therefore, insulin deficiency or hepatic insulin resistance increased the secretion of apoB. Insulin might modulate the production of a number of other proteins that affect circulating levels of lipoproteins. The release of stored fatty acids from adipocytes required conversion of stored triglyceride into fatty acids and monoglycerides that could be transferred across the plasma membrane of the cell. The primary enzyme that is responsible for this is hormone-sensitive lipase (HSSL). HSSL was inhibited by insulin, which decreased phosphorylation of HSSL and its association with the stored lipid droplet [59]. Dyslipidaemia seen in diabetes mellitus was important in terms of explaining the accelerated atherosclerosis and subsequent progression to cardiovascular disease. Jain, et al. [60] observed a progressive increase in the lipid fractions with duration and poor glycaemic control in diabetics and suggested that a good control of hyperglycaemia was important in keeping the lipid levels in near normal range. Goldberg [17] reported that replacement of insulin in insulin dependent diabetic patients might correct these abnormalities, and well controlled diabetics may have increased HDL and lower than average triglyceride levels. Therefore, as observed in the current study, both the insulin treated diabetic groups and extract treated groups showed a decreased level of triglycerides, total cholesterol, and LDL, and increased levels of HDL when compared to the untreated diabetic group which is an indication that both insulin and the extract of A. leiocarpus had the ability to attenuate dyslipidaemia in alloxan-induced diabetes in dogs and rats. This could be due to the anti hyperglycaemic effects of the plant as earlier discussed. It is therefore very reasonable to summarize that this extract of A. leiocarpus could be a very good nonconventional treatment to replace insulin and correct the dyslipidaema towards avoiding atherosclerosis and cardiovascular complications associated with type 1 diabetes mellitus. In addition, withdrawal of the ethanolic extract of A. leiocarpus as treatment of alloxan-induced type 1 DM prevented reversal/reoccurrence of hyperglycaemia [36].
Conclusion
Alloxan monohydrate caused alterations in lipid profiles such as high level of total cholesterol, triglycerides and abnormalities in LDL and HDL. Anogeissus leiocarpus was able to ameliorate the dyslipidaemia thus may be useful in preventing the progression of macrovascular diseases associated with diabetes mellitus like cardiovascular disease.
Data Availability
Data presented in this study are available on request from the corresponding author.
Ethical Approval
All procedures carried out on animals in this study were approved and performed in accordance with the ethical standards of the Ahmadu Bello University Committee on Animal Use and Care, Ahmadu Bello University Zaria.
Author’s Contribution
Num-Adom, SM: Conceptualisation, Investigation &Writing- review. Ogbuagu, NE: Investigation & Editing. Aluwong, T: Conceptualisation, Supervision, Investigation, Writing-review & Editing. Adamu, S: Investigation, Writing-review & Editing. Umar, IA: Conceptualisation, Supervision, Investigation, Writing-review & Editing. Esievo, KAN: Conceptualisation, Supervision, Investigation, Writing-review & Editing.
Acknowledgement
The nutrition laboratory of the Department of Veterinary Medicine ABU Zaria and Department of Chemical Pathology, ABUTH Shika.
References
-
Duckworth WC, McCarren M, Abraira C (2001) Glucose control and cardiovascular complications: the VA diabetes trial. Diabetes Care 24(5): 942-945.
-
Piero MN, Nzaro GM, Njagi JM (2014) Diabetes mellitus – a devastating metabolic disorder. Asian J Biomed Pharm Sci 4(40): 1-7.
-
Punthakee Z, Goldenberg R, Katz P (2018) Definition, classification and diagnosis of diabetes, prediabetes and metabolic syndrome. Can J Diabetes 42(1): S10-S15.
-
Sekiou O, Boumendjel M, Taibi F, Boumendjel A, Messarah M (2019) Mitigating effects of antioxidant properties of Artemisia herba alba aqueous extract on hyperlipidemia and oxidative damage in alloxan-induced diabetic rats. Arch Physiol Biochem 125(2): 163-173.
-
(2017) IDF Diabetes Atlas. 8th (Edn.). International Diabetes Federation.
-
Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U, et al. (2014) Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res Clin pract 103(2): 137-149.
-
Amjad S, Jafri A, Sharma AK, Serajuddin M (2019) A novel strategy of nanotized herbal drugs and their delivery in the treatment of diabetes: Present status and future prospects. J Herb Med 17-18: 100279.
-
Armstrong DG, Boulton AJM, Bus SA (2017) Diabetic foot ulcers and their recurrence. New Eng J Med 376(24): 2367-2375.
-
Skrepnek GH, Mills JL, Lavery LA, Armstrong DG (2017) Health care service and outcomes among an estimated 6.7 million ambulatory care diabetic foot cases in the US. Diabetes Care 40(7): 936-942.
-
Guo W, Li M, Dong Y, Zhou H, Zhang Z, et al. (2020) Diabetes is a risk factor for the progression and prognosis of COVID‐19. Diabetes/Metab Res Rev 36(7): e3319.
-
Hussain A, Bhowmik B, Moreira NC (2020) COVID-19 and diabetes: Knowledge in progress. Diabetes Res Clin Pract 162: 108142.
-
Zhu L, She ZG, Cheng X, Qin JJ, Zhang XJ, et al. (2020) Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell Metab _31_(6): 1068-1077.
-
Kumar V, Ahmed D, Gupta PS, Anwar F, Mujeeb M (2013) Anti-diabetic, anti-oxidant and anti-hyperlipidemic activities of Melastoma malabathricum Linn. leaves in streptozotocin induced diabetic rats. BMC complement Altern Med 13(1): 222.
-
Zhang ZJ, Zheng ZJ, Kan H, Song Y, Cui W, et al. (2011) Reduced risk of colorectal cancer with metformin therapy in patients with type 2 diabetes: a meta- analysis. Diabetes Care 34(10): 2323-2328.
-
Kumar V (2015) Antidyslipidemic and antioxidant activities of _Tinospora cordifolia_ stem extract in alloxan induced diabetic rats. Ind J Clin Biochem 30: 473-478.
-
Ginsberg HN (1996) Diabetic dyslipidemia: basic mechanisms underlying the common hypertriglyceridemia and low HDL cholesterol levels. Diabetes 45(S3): S27-S30.
-
Goldberg IJ (2001) Diabetic dyslipidemia: Causes and consequences. J Clin Endocrinol Metab 86(3): 965-971.
-
Hirano T, Naito H, Kurokawa M, Ebara T, Nagano S, et al. (1996) High prevalence of small LDL particles in non-insulin-dependent diabetic patients with nephropathy. Atherosclerosis 123(1-2): 57-72.
-
Adiels M, Westerbacka J, Soro-Paavonen A, Häkkinen AM, Vehkavaara S, et al. (2007) Acute suppression of VLDL1 secretion rate by insulin is associated with hepatic fat content and insulin resistance. Diabetologia 50(11): 2356-2365.
-
Mooradian AD (2009) Dyslipidemia in type 2 diabetes mellitus. Nature Clin Pract Endocrinol Metab 5(3): 150- 159.
-
Aluwong T, Ayo JO, Kpukple A, Oladipo OO (2016) Amelioration of hyperglycaemia, oxidative stress and dyslipidaemia in alloxan-induced diabetic wistar rats treated with probiotic and vitamin C. Nutrients 8(5): 151.
-
Mullugeta Y, Chawla, R, Kebede T, Worku Y (2012) Dyslipidemia associated with poor glycemic control in type 2 diabetes mellitus and the protective effect of metformin supplementation. Indian J Clin Biochem 27(4): 363-369.
-
Klisic A, Kavaric N, Jovanovic M, Zvrko E, Skerovic V, et al. (2017) Association between unfavorable lipid profile and glycemic control in patients with type 2 diabetes mellitus. J Res Med Sci 22: 122.
-
Yadav NK, Thanpari C, Shrewastwa MK, Mittal RK (2012) Comparison of lipid profile in type-2 obese diabetics and obese non-diabetic individuals. A hospital based study from Western Nepal. Kathmandu Uni Med J 10(39): 44-
-
Zabeen B, Balsa AM, Islam N, Parveen M, Nahar J, et al. (2018) Lipid profile in relation to glycemic control in type 1 diabetes children and adolescents in Bangladesh. Indian J Endocrinol Metabolism 22(1): 89- 92.
-
Hui H, Zhao X, Perfetti R (2005) Structure and function studies of glucagon‐like peptide‐1 (GLP‐1): the designing of a novel pharmacological agent for the treatment of diabetes. Diabetes Metab Res Rev 21(4): 313-331.
-
Bathaie SZ, Mokarizade N, Shirali S (2012) An overview of the mechanisms of plant ingredients in the treatment of diabetes mellitus. J Med Plants 11(44): 1-24.
-
Qureshi M, Gammoh E, Shakil J, Robbins R (2018) Update on management of type 2 diabetes for cardiologists. Methodist DeBakey cardiovascular J 14(4): 273-280.
-
Dey L, Attele AS, Yuan CS (2002) Alternative therapies for type 2 diabetes. Alternative Medicine Review 7(1): 45-58.
-
Kooti W, Farokhipour M, Asadzadeh Z, Ashtary-Larky D, Asadi-Samani M (2016) The role of medicinal plants in the treatment of diabetes: a systematic review. Electron Physician 8(1): 1832-1842.
-
Raj R, Tripathi J, Sahay S (2016) Medications of diabetes mellitus and antidiabetic medicinal plants: A review. Int J Indian Herbs Drugs 1(1):19-28.
-
Balogh E, Toth M, Bölcsházi G, Abonyi-Toth ZS, Kocsis E, et al. (2008) Oral hypoglycaemic drugs in alloxan-induced diabetes mellitus in dogs. Acta Vet Brno 77(3): 363-371.
-
Rao MU, Sreenivasulu M, Chengaiah B, Reddy KJ, Chetty CM (2010) Herbal medicines for diabetes mellitus: a review. Int J PharmTech Res 2(3): 1883-1892.
-
Yagi A, Hegazy S, Kabbash A, Wahab EAE (2009) Possible hypoglycemic effect of Aloe vera L. high molecular weight fractions on type 2 diabetic patients. Saudi Pharm J 17(3): 209-215.
-
American Diabetes Association (2004) Gestational diabetes mellitus. Diabetes care 27(1): s88-s90.
-
Num-Adom SM, Adamu S, Aluwong T, Ogbuagu NE, Umar AI, et al. (2022) Ethanolic extract of Anogeissus leiocarpus ameliorates hyperglycaemia, hepato-renal damage, deranged electrolytes and acid-base balance in alloxan-induced diabetes in dogs. Sci Afr 16: e01183.
-
Akah PA, Alemji JA, Salawu OA, Okoye TC, Offiah NV (2009) Effects of Vernonia amygdalina on biochemical and hematological parameters in diabetic rats 1(3): 108- 113.
-
Akomas SC, Okafor AI, Ijioma SN (2014) Glucose level, haematological parameters and lipid profile in Ficus sur treated diabetic rats. Comparative J Agric Biol Sci 2(1): 5-11.
-
Farsani MK, Amraie E, Kavian P, Keshvari M (2016) Effects of aqueous extract of alfalfa on hyperglycemia and dyslipidemia in alloxan-induced diabetic Wistar rats. Interv Med Appl Sci 8(3): 103-108.
-
Navghare V, Dhawale S (2016) Suppression of Type II diabetes with dyslipidemia and nephropathy by peels of Musa cavendish fruit. Indian Journal of Clinical Biochemistry 31(4): 380-389.
-
Num SM, Oladele SB, Esievo KAN, Useh NM (2014) Some observations in Wistar rats administered ethanol extracts of the stem barks of Anogeissus leiocarpus. Asian J Pharm Toxicol 2(3): 4-10.
-
Esievo KAN, Num-Adom SM, Adamu S, Ogbuagu NE, Aluwong T, et al. (2021) Elevated serum sialic acids, a potent biomarker of alloxan-induced type 1 diabetes in dogs by ethanolic extract of Anogeissus leiocarpus. J Diabetes Metab Disord 20(1): 179-186.
-
Allain CC, Poon LS, Chan CS, Richmond WFPC, Fu PC (1974) Enzymatic determination of total serum cholesterol. Clin Chem 20(4): 470-475.
-
Burstein S, Zamoscianyk H, Kimball HL, Chaudhuri NK, Gut M (1970) Transformation of labeled cholesterol, 20α-hydroxycholesterol, (22R)-22-hydroxycholesterol, and (22R)-20α, 22-dihydroxycholesterol by adrenal acetone-dried preparations from guinea pigs, cattle and man: I. Establishment of radiochemical purity of products. Steroids 15(1): 13-60.
-
Friedewald WT, Levy RI, Fredrickson DS (1972) Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18(6): 499-450.
-
Evans WC (1996) Trease and Evans’ pharmacognosy. 14th (Edn.). WB Saunders, pp: 119-159.
-
Trease K, Evans WC (1996) Textbook of Pharmacognosy. 14th (Edn.). London: Balliere, Tindall.
-
Harbone JB (1973) Phytochemical methods: a guide to modern techniques for plat analysis. 3rd (Edn.). Chapman and Hill. London, pp: 279.
-
Bohm BA, Abyazani RK (1994) Flavonoids and condensed tannins from leaves of Vaccinium raticulatum and Vaccinium calcymium (Ericaceae). University of Hawaii Press 48(4): 458-463.
-
Obadoni B, Ochuko PO (2001) Phytochemical studies and comparative efficacy of the crude extract of some homeostatic plants in Edo, Delta States of Nigeria. Glob J Pure Appl Sci 8(2): 230-208.
-
Burden JPV, Robinson WC (1969) Formatin of complexes between protein and tannic acids. J Agric Food Chem 17(4): 772-777.
-
Erejuwa OO, Sulaiman SA, Ab Wahab MS (2012) Honey- a novel antidiabetic agent. International Journal of Biological Science 8(6): 913-934.
-
Vega GL, Grundy SM (2019) Current trends in non-HDL cholesterol and LDL cholesterol levels in adults with atherosclerotic cardiovascular disease. J Clin Lipidol 13: 563-567.
-
Shivananda RH, Shedthi S, Shetty SK, Jeppu AK (2012) Comparison between lipid profile and atherogenic index of plasma (AIP) in alcoholic and non-alcoholic diabetic patients in Mangalore, Southern India.
-
Dixon JL, Furukawa S, Ginsberg HN (1991) Oleate stimulates secretion of apolipoprotein B-containing lipoproteins from Hep G2 cells by inhibiting early intracellular degradation of apolipoprotein B. J Biol Chem 266(8): 5080-5086.
-
Lewis GF, Uffelman KD, Szeto LW, Weller B, Steiner G (1995) Interaction between free fatty acids and insulin in the acute control of very low density lipoprotein production in humans. J Clin investig 95(1): 158-166.
-
Taghibiglou C, Carpentier A, Van Iderstine SC, Chen B, Rudy D, ET AL. (2000) Mechanisms of hepatic very low density lipoprotein overproduction in insulin resistance: evidence for enhanced lipoprotein assembly, reduced intracellular ApoB degradation, and increased microsomal triglyceride transfer protein in a fructose- fed hamster model. J Biol Chem 275(12): 8416-8425.
-
Sparks JD, Sparks CE (1990) Insulin modulation of hepatic synthesis and secretion of apolipoprotein B by rat hepatocytes. J Bio Chem 265(15): 8854-8862.
-
Stralfors P, Honnor RC (1989) Insulin-induced dephosphorylation of hormone-sensitive lipase. Correlation with lipolysis and cAMP-dependent protein kinase activity. European J Biochem 182(2): 379-385.
-
Jain HR, Shetty V, Singh GS, Shetty S (2016) A study of lipid profile in diabetes mellitus. Int J Sci study 4(9): 55- 60.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance