Macrosomia: A Serious Complication of Diabetes in Pregnancy
Gestational diabetes mellitus (GDM) and its associated complication, macrosomia, pose significant challenges during pregnancy. This review explores the epidemiological aspects, pathophysiology, complications, and long-term consequences of these conditions, with a focus on the need for early detection and advanced management strategies. The prevalence of GDM varies globally, with particular attention to India, where the correlation between macrosomia and GDM is evident. Early prenatal monitoring and glycemic control have been identified as effective strategies to reduce macrosomia incidence. Understanding the pathophysiology of GDM reveals a complex interplay of β-cell dysfunction and chronic insulin resistance, resulting in elevated blood sugar levels. This disruption contributes to macrosomia, characterized by the birth of abnormally large infants. Complications associated with macrosomia are not limited to childbirth; mothers may experience protracted labor, uterine atony, and an increased risk of tears, while newborns face the challenge of shoulder dystocia and neonatal jaundice. Additionally, the enduring significance of exposure to GDM in utero is concerning, with evidence linking it to childhood obesity and metabolic syndrome. The review also discusses promising research directions. The study of glycation markers aims to improve macrosomia prediction, enabling better management and care for affected pregnancies. Moreover, the integration of mobile technology, such as the GDm health smartphone solution, offers remote monitoring of blood glucose levels and tailored feedback, potentially revolutionizing GDM management. In tackling the challenges presented by GDM and macrosomia, a multifaceted approach is essential. Early and effective prenatal care, coupled with vigilant glycemic control, is critical for the well-being of both mothers and their infants. Continued research into innovative screening and management methods will further enhance pregnancy outcomes and long-term health. Healthcare professionals, armed with a comprehensive understanding of these conditions and their extensive effects, play a pivotal role in supporting expectant mothers and ensuring a brighter and healthier future for both mother and child.
Introduction
GDM is a significant complication that can develop during pregnancy, affecting many expectant mothers. Its
prevalence varies across different countries, ranging from 5.4% to 25.1% [1]. It is characterized by the inception of glucose intolerance in pregnancy or the first recognition of such intolerance in an individual. Macrosomia, often associated with GDM, is distinct as a birth weight greater than 4,000 grams or exceeding the 90th percentile for gestational age [2]. In pregnancies affected by diabetes, macrosomic fetuses exhibit a distinct form of overgrowth, particularly relating to the vital accumulation of hypodermal fat in the interscapular and abdominal regions [3]. This results in thicker upper-extremity skinfolds, larger upper-extremity circumferences, smaller head-to-shoulder ratios, larger shoulder and extremity circumferences, and overall increased extremity dimensions. Macrosomia is associated with higher neonatal morbidity rates. Compared to newborns of mothers without diabetes, macrosomic neonates are five times more likely to experience severe hypoglycemia and have a twofold rise in neonatal jaundice [4]. While some research suggests a link between maternal glucose intolerance and the increased chance of macrosomia, other studies have found that maternal obesity and extreme weight increase during pregnancy have a more significant impact on the development of a large-for-gestational-age (LGA) fetus [5]. It’s vital to notice that obese mothers may give birth to babies who are at higher risk of obesity, creating a potential cycle of obesity that extends into childhood [6]. In this review, we will delve into the impact of maternal diabetes during pregnancy on both embryonic and fetal health, as well as the subsequent health of the newborn infant. We will explore the various ways in which maternal diabetes can influence these aspects. It’s important to note, however, that a comprehensive examination of the intricate mechanisms and pathogenesis of diabetic embryopathy, as well as a detailed analysis of treatment optimization strategies, goes beyond the scope of this clinical review.
Epidemiological Aspects of GDM Leading to the Occurrence of Macrosomia
The epidemiology of diabetes, particularly when exacerbated by macrosomia (the condition of giving birth to a larger-than-average baby), is not well understood in India. However, available research suggests a significant correlation between macrosomia and gestational diabetes GDM. In India, the prevalence of macrosomia varies widely, ranging from 0.5% to as high as 15-45% [7]. Some studies have shed light on potential strategies to reduce the incidence of macrosomia. Strengthening prenatal monitoring has been identified as a valuable approach. For example, a study conducted in rural Haryana, India, found that enhancing prenatal care and monitoring could effectively lower the occurrence of macrosomia [8]. Additionally, maintaining good glycemic control among pregnant women is another essential factor in addressing macrosomia. Research indicates that proper management of blood sugar levels during pregnancy can contribute to a reduced prevalence of macrosomia [9].
Pathophysiology of GDM
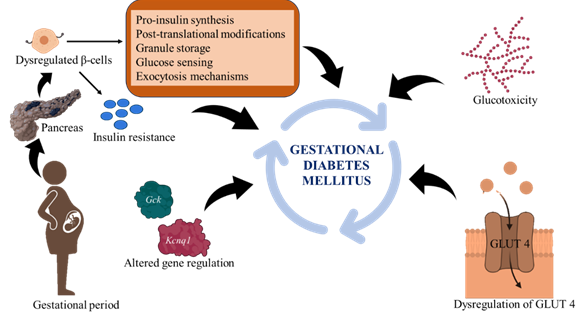
As GDM is typically caused by chronic insulin resistance during pregnancy, it involves both insulin resistance in the tissues and defective beta cells. β-Cell Dysfunction: The disruption of β-cells is a critical factor in the advancement of diseases like GDM. The main part of these cells is to collect and release insulin in reply to blood glucose levels. It is believed that chronic excess fuel- induced elevated insulin production may be a contributing factor to β-cell dysfunction over an extended period [10]. This dysfunction can manifest at various stages of the insulin production and secretion process, including post- translational modifications, granule storage, pro-insulin synthesis, exocytosis mechanisms, and glucose sensing. Genetic susceptibility plays a role in β-cell dysfunction, with genes like Kcnq1 and Gck being associated with GDM. Minor defects in the β-cell mechanism may become evident during metabolic stress, like pregnancy, highlighting the complexity of this condition’s underlying mechanisms [11]. Insulin resistance increases the dysfunction of β-cells by reducing the uptake of glucose stimulated by insulin, which results in hyperglycemia. This puts stress on β-cells and makes them produce more insulin than usual. Glucotoxicity, the harmful effects of high blood sugar worsen β-cell function and initiates a malicious cycle of hyperglycemia, insulin resistance, and progressively worsening β-cell degeneration [12].
Chronic Insulin Resistance
A condition known as insulin resistance occurs when cells are unable to react to insulin as well. Insulin resistance usually results from a malfunction in the signaling pathways that insulin triggers at the molecular level. The glucose transporter 4 (GLUT4) is not adequately transported to the cell’s plasma membrane as a result of this breakdown. The rate at which insulin promotes the uptake of glucose is significantly reduced when it comes to GLUT4, a critical protein that is in charge of delivering glucose into the cell where it can be used for energy production. More precisely, compared to a normal pregnancy, there is a 54% decrease in the effectiveness of insulin in GDM in promoting the entry of glucose into cells [13]. The pathophysiology of GDM caused by β-cells dysregulation and chronic insulin resistance is illustrated in Figure 1.
Pathophysiology of Macrosomia in GDM
Pedersen’s hypothesis, a well-accepted explanation for the pathophysiology of macrosomia [14], revolves around the development of gestational diabetes in some pregnant women. This condition is characterized by elevated blood sugar levels, primarily attributed to two main factors: insulin resistance and poor glucose metabolism during pregnancy. In response to the increased maternal blood sugar levels, the fetal pancreas can produce excessive amounts of insulin. Insulin is a vital hormone responsible for regulating blood sugar levels [15]. The elevated insulin levels in fetal circulation play a vital role in promoting the uptake and utilization of glucose. This essentially means that the fetus absorbs more glucose from the mother’s bloodstream, potentially providing an increased energy source for fetal growth and development [16]. However, excess glucose that the fetus doesn’t immediately use for energy is stored as fat tissue. Therefore, the heightened glucose utilization resulting from fetal hyperinsulinemia can lead to the accumulation of fat tissue in the fetus, ultimately resulting in macrosomia [17]. This condition refers to the birth of an abnormally large infant.
Complications Associated with Macrosomia
Complications for Mothers: Extra-large babies can present more complicated challenges for a vaginal birth. There is a higher chance of protracted labor, in which the baby can become lodged in the birth canal and may need to be extracted using a vacuum or forceps. An unscheduled or emergency cesarean section might be required in certain circumstances. In addition, compared to deliveries of average size babies, there is an increased risk of tears and abrasions to the vaginal tissue during the birthing process. Additionally, there’s an increased chance of the muscle separating the anus from the vagina [18]. In addition, there is a higher risk of uterine atony, a condition in which the uterine muscle may not contract normally, followed by severe bleeding and hemorrhage after delivery. Studies indicate that macrosomic deliveries carry a 3–5 times higher risk of genital tract injury and postpartum hemorrhage [19]. Additionally, there is a high risk of uterine tears along the scar line from the previous surgery if the mother has had a caesarean section.
Issues with the Fetus
Shoulder Dystocia: One of the most significant complications associated with macrosomic babies is shoulder dystocia. It happens when the baby’s head has passed through the birth canal, but one or both shoulders may jam beside the mother’s pelvic bone. This can create a critical situation during delivery, as it can obstruct the baby’s progress down the birth canal [20]. The brachial plexus is a network of nerves that control the actions and sensations of the shoulder, arm, and hand. When a baby experiences shoulder dystocia, the pressure and stretching exerted on the brachial plexus nerves can lead to injury. This injury is known as a brachial plexus injury. The risk of such an injury is much higher in macrosomic babies, according to some estimates, the risk increases by about 20 times when the birth weight exceeds 4,500 grams [21].
Jaundice in Newborns: Newborn jaundice, also known as neonatal jaundice, is a general aspect where a baby’s skin and eyes develop a yellowish hue. This discoloration occurs due to elevated levels of bilirubin in the blood, which is a yellow pigment produced when red blood cells break down. While mild jaundice is frequently observed in newborns, especially in the first few days of life, it can be more prevalent in high birth weight infants, often referred to as macrosomic babies.
One potential reason for the higher occurrence of jaundice in macrosomic babies is their increased need for oxygen. This heightened oxygen demand might trigger the body to stimulate the production of more red blood cells, a process known as erythropoiesis. This is the body’s way of trying to meet the increased oxygen requirements. However, an unintended consequence of this heightened erythropoiesis is the development of polycythemia. An excessive number of red blood cells circulates in the bloodstream of a newborn with polycythemia [22].
Later Complications: Childhood Metabolic Syndrome and Obesity. Numerous research indicates that GDM may be a contributing factor in childhood obesity. There has been proof that prenatal exposure to diabetes can program an offspring’s later development of obesity. When compared to the offspring of prediabetic or nondiabetic women, the offspring of Pima Indian women with type II diabetes and GDM at birth were greater for gestational age at birth and heavier later about five years of age [23]. According to the 6 to 13-year-old multiethnic kids in the Exploring Perinatal Outcomes among Children (EPOCH) trial, revelation to maternal GDM was linked to greater BMI, a larger waist perimeter, more instinctive and hypodermal adipose tissue, and a more unified fat dispersal pattern [24]. Additionally, children and adolescents exposed to maternal GDM in utero showed greater average BMI rises from 27 months to 13 years of age, as well as greater BMI growth velocity beginning at 10–13 years of age. These results imply that the long-term significance of being exposed to GDM in utero may not necessarily be noticeable in the initial years but slightly manifest at puberty, which is another susceptible time for the cause of obesity. Children of diabetic moms are also more likely to develop metabolic syndromes, which raise the risk of stroke, diabetes, and heart disease by coexisting with elevated blood pressure, obesity, hyperglycemia, and abnormal cholesterol levels [25].
Future Aspects: According to a 2022 study, pregnant women with GDM who are insulin-resistant may experience varied pregnancy outcomes, such as macrosomia [26]. A significant increase in macrosomia in the offspring of mothers with GDM has been demonstrated in several studies [27]. According to a study published in 2023, high HbA1c levels are significantly related to macrosomia during GDM pregnancies [28]. New glycation markers are being studied in a clinical trial to potentially predict macrosomia and GDM. The purpose of this trial is to create novel screening methods for macrosomia associated with GDM [29]. A real-time smartphone solution called GDM Health has been developed using mobile technologies to manage women with GDM. With the use of this technology, blood glucose levels may be remotely monitored, and patients can receive tailored feedback [30].
Conclusion
To sum up, pregnant women face numerous difficulties due to GDM and macrosomia, a condition that is linked to the disease. The epidemiological features of macrosomia and GDM differ throughout the world, however, India has a significant prevalence and may be able to lower it. A complicated interaction between chronic insulin resistance and -cell dysfunction, which results in high blood sugar levels, underlies the pathogenesis of GDM. As a result of this disturbance, macrosomia, which is characterized by the birth of abnormally big children, might develop. Prolonged labour, uterine atony, shoulder dystocia, brachial plexus injuries, and a higher risk of neonatal jaundice are just a few of the issues that can arise from macrosomia in women and babies.
Moreover, childhood obesity and metabolic syndrome are at an elevated risk due to the effects of maternal diabetes. The enduring effects of foetal GDM exposure highlight the significance of early detection and treatment. Prospective research directions centre on glycation indicators and mobile technology, to enhance macrosomia prediction and management. A multifaceted strategy comprising early and effective prenatal care, glycemic control, and ongoing research into cutting-edge screening and management methods is essential in tackling the problems presented by GDM and macrosomia. Healthcare professionals may better support expecting moms and their newborns by being aware of the intricacies of these diseases and their wide-ranging effects. This will help to enhance pregnancy results and the enduring health of both the mother and the child.
Acknowledgment
The authors thank the Chettinad Academy of Research and Education for their support and encouragement.
References
-
Gao C, Sun X, Lu L, Liu F, Yuan J (2019) Prevalence of gestational diabetes mellitus in mainland China: a systematic review and meta‐analysis. J Diabetes Investig 10(1): 154-162.
-
Collier A, Abraham EC, Armstrong J, Godwin J, Monteath K, et al. (2017) Reported prevalence of gestational diabetes in Scotland: The relationship with obesity, age, socioeconomic status, smoking and macrosomia, and how many are we missing. J Diabetes Investig 8(2): 161- 167.
-
McFarland MB, Trylovich CG, Langer O (1998) Anthropometric differences in macrosomic infants of diabetic and nondiabetic mothers. J Matern Fetal Med 7(6): 292-295.
-
Mitanchez D, Yzydorczyk C, Simeoni U (2015) What neonatal complications should the pediatrician be aware of in case of maternal gestational diabetes. World J Diabetes 6(5): 734-743.
-
Akanmode AM, Mahdy H (2020) Macrosomia. StatPearls: Content is Kind.
-
Herring SJ, Oken E (2011) Obesity and diabetes in mothers and their children: can we stop the intergenerational cycle. Curr Diab Rep 11(1): 20-27.
-
Kamana KC, Shakya S, Zhang H (2015) Gestational diabetes mellitus and macrosomia: a literature review. Ann Nutr Metab 66(2) 14-20.
-
Malik M, Khanna P, Verma R (2018) The association of maternal risk factors to macrosomia in rural areas of Haryana, India: a community based study. Int j community med public health 5(9): 3842-3846.
-
Maheshwari Anuj (2013) macrosomia in India: is glycemic control the key determinant. J Adv Res 5: 303- 306.
-
Weir GC, Laybutt DR, Kaneto H, Bonner Weir S, Sharma A (2001) Beta-cell adaptation and decompensation during the progression of diabetes. Diabetes 50(1): 154-159.
-
Prentki M, Nolan CJ (2006) Islet β cell failure in type 2 diabetes. J Clin Invest 116(7): 1802-1812.
-
Ashcroft FM, Rohm M, Clark A, Brereton MF (2017) Is type 2 diabetes a glycogen storage disease of pancreatic β cells. Cell Metab 26(1): 17-23.
-
Plows JF, Stanley JL, Baker PN, Reynolds CM, Vickers MH (2018) The pathophysiology of gestational diabetes mellitus. Int J Mol Sci 19(11): 3342.
-
Catalano PM, Mouzon SHD (2011) Is it time to revisit the Pedersen hypothesis in the face of the obesity epidemic. Am J Obstet Gynecol 204(6): 479-487.
-
Farrar D (2016) Hyperglycemia in pregnancy: prevalence, impact, and management challenges. Int J Womens Health 8: 519-527.
-
Hay WW (2006) Placental-fetal glucose exchange and fetal glucose metabolism. Trans Am Clin Climatol Assoc 117: 321-340.
-
Ornoy A, Becker M, Weinstein Fudim L, Ergaz Z (2021) Diabetes during pregnancy: A maternal disease complicating the course of pregnancy with long-term deleterious effects on the offspring. a clinical review. Int J Mol Sci 22(6): 2965.
-
Ali U. A, Norwitz ER (2009) Vacuum-assisted vaginal delivery. Rev Obstet Gynecol 2(1): 5-17.
-
Nuwagaba J, Dave D (2022) Management of neonatal complications of macrosomia: A case report at a tertiary hospital in a developing country. Clin Case Rep 10(1): e05298.
-
Hill MG, Cohen WR (2016) Shoulder dystocia: prediction and management. Womens Health (Lond) 12(2): 251- 261.
-
Turkmen S, Johansson S, Dahmoun M (2018) Foetal macrosomia and foetal-maternal outcomes at birth. J Pregnancy 2018: 4790136.
-
Ansong Assoku B, Shah SD, Adnan M, Ankola PA (2018) Neonatal jaundice. StatPearls Publishing, Book.
-
Pettitt DJ, Nelson RG, Saad MF, Bennett PH, Knowler WC (1993) Diabetes and obesity in the offspring of Pima Indian women with diabetes during pregnancy. Diabetes care 16(1): 310-314.
-
Crume TL, Ogden L, West NA, Vehik KS, Scherzinger A, et al. (2011) Association of exposure to diabetes in utero with adiposity and fat distribution in a multiethnic population of youth: the Exploring Perinatal Outcomes among Children (EPOCH) Study. Diabetologia 54(1): 87- 92.
-
Crume TL, Ogden L, Daniels S, Hamman RF, Norris JM, et al. (2011) The impact of in utero exposure to diabetes on childhood body mass index growth trajectories: the EPOCH study. J Pediatr 158(6): 941-946.
-
Bernea EG, Uyy E, Mihai DA, Ceausu I, Ionescu Tirgoviste C, et al. (2022) New born macrosomia in gestational diabetes mellitus. Exp Ther Med 24(6): 710.
-
Yuan Y, Zhu Q, Yao X, Shi Z, Wen J (2023) Maternal circulating metabolic biomarkers and their prediction performance for gestational diabetes mellitus related macrosomia. BMC Pregnancy Childbirth 23(1): 113.
-
Mou SS, Gillies C, Hu J, Danielli M, Al Wattar BH, et al. (2023) Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women. J Clin Med 12(11): 3852.
-
Nahavandi S, Seah JM, Shub A, Houlihan C, Ekinci EI (2018) Biomarkers for Macrosomia Prediction in Pregnancies Affected by Diabetes. Front Endocrinol (Lausanne) 9: 407.
-
Garg N, Arunan SK, Arora S, Kaur K (2022) Application of Mobile Technology for Disease and Treatment Monitoring of Gestational Diabetes Mellitus Among Pregnant Women: A Systematic Review. J Diabetes Sci Technol 16(2): 491-497.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance