Tailored Dietary Plan to Sustain Healthy Lifestyle of Adults with Restrained Mobility
Background and Objectives: Globesity - the epidemic of obesity - contributes significantly to NCDs, the impairment of cognition and memory, reduction in quality of life and increased health-care costs. Changes in dietary patterns (i.e., chronic excess intake) aligned with physical inactivity (reduced energy expenditure) increase the positive energy balance and fuel the obesity prevalence. As prevention is better than cure, hence formulating a diet plan associated with regular physical activity regimen may offer a sustainable healthy lifestyle to adults with restrained mobility. Methods: This article portrays the cognitive-behavioural therapy for obesity together with the role of common nutraceuticals, phytochemicals that regulate hormonal levels to achieve optimum health. Results: The outlined nutritional interventions that obese individuals may adapt have been considered to modulate the utilisation of nutrients and impact major physiological processes. Nonetheless, responsibility of tackling obesity rests with individuals and their own practices and actions. Conclusion: Governments should recognize that they have important roles to play in addressing the obesity epidemic such as investments in resources and recreational facilities like parks to sensitize the public regarding the importance of physical exercise and healthy diets. With the help of different stakeholders executing their responsibilities, the globe will certainly make faster progress in its ‘war’ against obesity and sedentary lifestyles.
Jomana Khawandanah1,2*, Dina Khawandanah3, Sundus Tewfik4 and Ihab Tewfik5
Pro Opio Melano Cortin; CART: Cocaine and Amphetamine- Regulated Transcript; PYY: Peptide Tyrosine Tyrosine; GLP- 1: Glucagon-Like Peptide-1.
Introduction
Today more than ever, protecting public health is key goal that governments across the globe are striving to achieve. The coronavirus pandemic has fiercely shaken the world, imposing guidelines on social distancing and movements restrictions. All gains that are being made in these campaigns to contain the spread illustrate the crucial role that interventions play in securing public health and wellbeing.
The purpose of this article is to explore an intelligible diet regimen to manage excessive body weight during such unprecedent circumstances as part of efforts to modulate its metabolic co-morbidities. The article also outlines tailored diet to its nutraceutical contents that sustains wellbeing among individuals with sedentary lifestyles. Furthermore, the article reviews the knowledge and speculated links between the endocrine signaling and physiological process associated to sedentary behaviour.
The Globesity Pandemic
According to the Centers for Disease Control and Prevention (CDC), obesity has emerged as the most pressing healthcare challenges that plague today’s world. Such Physical changes Adverse outcomes Comorbidities Adipose Inflammatory response increase is worrying and underscores the need for urgent and aggressive solutions [1].
Obesity is also linked to some of the most common causes of global mortality, including diabetes, heart disease, stroke, and certain forms of cancer [2].
Since 1975 obesity rates have almost tripled in different parts of the world. In 2016, 39% of adults who were 18 years and above were overweight and 13% were obese. In the same year, nearly 340 million children and adolescents aged 5-19 years old were overweight or obese. Most recently, in 2020, 39 million children under the age of five were overweight or obese [3].
A recent investigation of the database of 400,000 UK residents during the time of March to April 2020 reported that 8.6% of COVID-19 hospitalisations were related to inadequate physical activity, and 29.5% due to overweight and obesity [4].
In large number of countries including the UK, overweight and/or obesity has been linked to an increased incidence of severe COVID-19 symptoms and patients were at higher risk to be admitted to intensive care unit (Figure 1) [5].
Metabolic changes OBESITY + COVID19
In the UK, it is estimated that at least one in four adults is afflicted with obesity. The large number of children and adults who are now obese have ignited calls from healthcare and child welfare experts who are urging authorities to move with speed to address this looming health crisis. Scholars are also challenging the government to work tirelessly toward reversing the alarming and sharp rise in the prevalence of obesity in the country [6].
While it is true that the US and UK have some of the highest obesity rates, this problem is of a global scale. Across the world, a sharp and sustained increase in the number of new diabetes cases is being reported. In fact, recently, it was determined that the rate of obesity and overweight is now higher than malnutrition rates [3]. Malnutrition is causing a double burden to the community in various low- and middle-income countries. As these countries not only at risk of undernutrition, but they are also experiencing a rapid increase in non-communicable disease risk factors particularly obesity and overweight, specifically in urban areas [3].
To fully understand the role that healthy diet and lifestyle modification can play in the lives of individuals who lead sedentary lives, there is a need to examine the risk factors for obesity as shown in Figure 2. Screens are taking up greater portion of the time that individuals spend on different matters, concurrent with physical inactivity which has been identified as the main risk factors [7, 8].
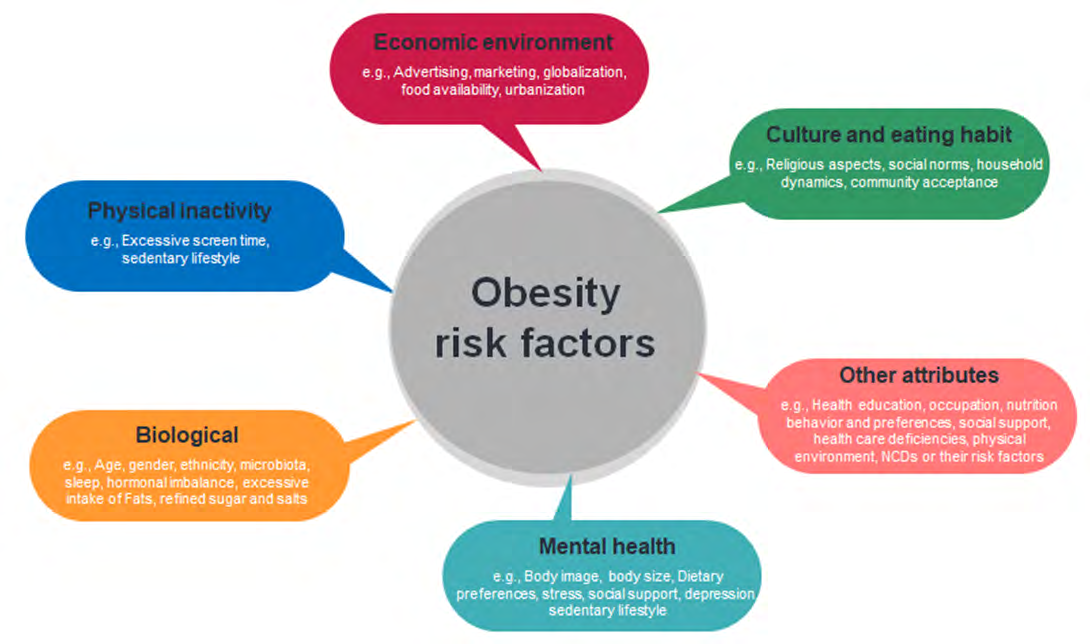
Hence, the latter has become an essential target that should be addressed if the obesity rates are to be lowered. The bright side is when engaging in minimal physical activity [e.g., daily 30 minutes of moderate intensity], individuals may increase their likelihood to combat weight gain.
Imbalanced nutrition is yet another factor that has been linked to obesity. Scholars agree that when diets are comprised primarily of energy-dense foods that are high in fat, sugar and salts, the probability of obesity rises substantially [9, 10].
Comorbidities and Medical Complications as Consequence of Obesity
What make obesity particularly worrying are the complications with which this condition has been associated. Obese individuals are more likely to develop such disorders and diseases as type 2 diabetes, heart disease, high blood pressure, certain type of cancers and gallbladder disease [1, 11] (Figure 3).
![Figure 2: Screens are taking up greater portion of the time that individuals spend on different matters, concurrent with physical inactivity which has been identified as the main risk factors [7,8].](/fulltextimages/9551/fig_2.png)
Tackling obesity is among the preventive measures that individuals can adopt. As will be shown in the discussions below, nutritional, and physical interventions are some of the safest, simplest and most effective solutions for reducing the risk of obesity and associated complications. Therefore, individuals are strongly encouraged towards changing behaviours, modifying their diet and incorporating physical exercise into their daily routine as part of their bid to lead fuller and healthier lives.
The Challenge of Behaviour Modification
Cognitive-behavioural therapy for obesity (CBT-OB) is relatively new personalised treatment that combines the traditional actions of standard behavioural therapy for obesity with a series of cognitive strategies and procedures. Such customised therapy assists the patient’s specific needs and addresses the cognitive processes by enhancing the treatment continuation and sustain weight loss. Moreover, the therapy can potentially progress on the outcomes reachable by traditional lifestyle-modification of long-term weight-loss treatments. Thus, CBT-OB has proven to be more effective approach than the standard weight-loss lifestyle- changes [12]. The goals of CBT-OB were based on a philosophy that patients are more motivated to achieve healthy weight loss, by agreeing lifestyle changes that promotes weight control and sustain ‘weight control mindset’. In essence, the CBT-OB is delivered over three levels of care: Outpatients, day hospital and residential. The CBT-OB curriculum is formed of six (6) modules delivered by health professionals and tailored to cater for morbidly obese patient’s needs, as part of their personalised therapeutic strategy [12].
Tailored Nutritional Interventions
As indicated above, healthier diets are among the tools that individuals can harness as they seek to reduce their risk of obesity and related complications. Some of the foods that help individuals to attain healthy weights are reviewed. The following sections highlight the endocrinal and nutraceutical roles of selected foods which have shown to affect the hormone balance, metabolic and physiological characteristics of obese individual.
Sex Hormones and Fertility
Obesity triggers endocrine changes that have adverse impacts on the health of individuals. For example, various scholars reported that obese individuals tend to experience hormonal imbalances which manifest by creating fertility problems [13]. Obesity has been associated to female infertility through multiple and complex mechanisms. In summary, adipose tissue, through the production of many factors such as leptin, free fatty acids (FFA), and cytokines, may affect both ovarian and endometrium functions, resulting in a change in oocyte maturation and endometrial epithelium receptivity [14]. The American Society for Reproductive Medicine has identified obesity among the leading drivers of infertility in women [15]. Obesity disrupts the endocrinal processes that underlie the storage of sex hormones. Thus, dietary modification can alleviate the likelihood of this issue among women.
Fortunately, there are many different foods and diets that have been demonstrated to alleviate the infertility issues that have been blamed on obesity.
This article outlines diets that are healthy and balanced such as DASH and or Mediterranean diets combined with physical activity regimen. Reduced fats dairy products and folic acid rich foods (Table 1) are among the recommended menus. While these foods are particularly beneficial for obese women, they also improve outcomes for women with healthy weight who wish to increase the chances of successful pregnancies [16]. The daily recommended intake of folic acid is shown in Table 2.
| Food | Serving | Micrograms (mcg) |
|---|---|---|
| Beef liver, braised, | 3 ounces | 215 |
| Spinach, boiled | ½ cup | 131 |
| Black-eyed peas (cowpeas), boiled, | ½ cup | 105 |
| Breakfast cereals, fortified | ½ cup | 100 |
| Rice, white, medium grain, cooked | ½ cup | 90 |
| Asparagus, boiled | 4 spears | 89 |
| Brussels sprouts, frozen, boiled | ½ cup | 78 |
| Spaghetti, cooked, enriched | ½ cup | 74 |
| Lettuce, romaine, shredded | 1 cup | 64 |
| Avocado, raw, sliced | ½ cup | 59 |
| Spinach, raw | 1 cup | 58 |
| Broccoli, chopped, frozen, cooked | ½ cup | 52 |
| Mustard greens, chopped, frozen, boiled | ½ cup | 52 |
| Bread, white | 1 slice | 50 |
| Green peas, frozen, boiled | ½ cup | 47 |
| Kidney beans, canned | ½ cup | 46 |
| Wheat germ | 2 tablespoons | 40 |
| Tomato juice, canned | ¾ cup | 36 |
| Crab, Dungeness | 3 ounces | 36 |
| Orange juice | ¾ cup | 35 |
| Turnip greens, frozen, boiled | ½ cup | 32 |
| Peanuts, dry roasted | 1 ounce | 27 |
| Orange, fresh | 1 small | 29 |
| Papaya, raw, cubed | ½ cup | 27 |
| Banana | 1 medium | 24 |
| Yeast, baker’s | ¼ teaspoon | 23 |
Table 1: List of food containing Folic acid per serving (National Institute of Health, 2021).
| Daily recommended Dose in Micro Grams (mcg) | |
|---|---|
| Adult/children > 11Years | 200 μg (From Food) |
| Women Considering Pregnancy | 200 μg (From Food) + 400 μg Supplement |
| Pregnant Women | 300 μg (From Food) + 400 μg Supplement |
| Pregnant Women | (First 12 Weeks of pregnancy) |
| Lactating Women | 260 μg (From Food) |
Table 2: Daily recommendation of Folic acid (vitamin B9).
On the other hand, alcohol, caffeine, and red meat are part of food quality that aggravate infertility associated to obesity [17]. These foods should therefore be avoided and substituted with healthier alternatives. For instance, women who are struggling to get pregnant can expect to enhance their fertility by adopting a diet that is high in protein with minimal fat and carbohydrate contents [18] for list of food containing hormones see Table 5.
Intermittent Fasting [IF]
Studies have demonstrated that insulin sensitivity increases and insulin levels decrease after a fasting phase [e.g. fasting for 16 hours and restricting the daily eating window to roughly 8 hours; or alternate-day fasting (ADF), which involves restringing food every other day, either by fasting the whole day or by consuming a few hundred calories [19], resulting in an improvement in fasting and postprandial glucose levels, however this requires further research [20]. Other studies reported that when standard calorie restriction and intermittent fasting were compared, fasting insulin, insulin resistance and visceral fat mass, were all reduced to matching levels, suggesting that intermittent fasting helps reduce the risk of type 2 diabetes in overweight and obese individuals [21].
The Interplay Between Gut Hormones and Appetite Control
Food intake is regulated by gut hormones which play crucial role in conveying signals of nutrition and energy status from the gut to the central nervous system and also to maintain energy homeostasis [22].
Several studies outlined the biochemical pathways modulating gut hormones and established the interrelation between food reward behaviour mechanisms and appetite regulation [22, 23].
Inside the hypothalamic arcuate nucleus (ARC), expressing two vital neurons with different effects on food intake, neuropeptide Y (NPY) and agouti-related peptide (AgRP) which trigger to increase food intake/ appetite and stimulate weight gain, and the other neurons (or neuropeptide mediators) proopiomelanocortin (POMC) and cocaine- and amphetamine-regulated transcript (CART) decrease food intake and supress appetite and can facilitate weight loss [22, 24]. These hormones will be discussed here as peptide tyrosine–tyrosine (PYY), glucagon-like peptide-1 (GLP-1), ghrelin, leptin and insulin influence the function of brain regions involved in appetite and satiety regulation [25]. Satiety signals peptide YY (PYY), glucagon-like peptide- 1(glp-1) reduce appetite while ghrelin (hunger hormone) stimulates food intake.
Food promotes the release of nutrient-activated anorexigenic hormones, including peptide YY (PYY) and glucagon-like peptide-1 (GLP-1), from enteroendocrine L cells in the gut, enhancing feelings of satiety [26]. Long-term energy balance is regulated by adiposity signals insulin and leptin hormones which are released in direct proportion to body fat mass [22, 27].
PYY is secreted by neuroendocrine L-cells in the distal gut. During fasting state, circulated PYY levels are low and increase rapidly after a meal with 1-2 hours peak and stay raised for several hours. PYY could affect food intake by increasing energy expenditure, delay gastric emptying, and decrease acid. Furthermore, PYY may modulate weight management which is stimulated by the fat content of food compared with protein or carbohydrate [22].
The incretin glucagon-like peptide 1 (GLP-1), also released from the neuroendocrine L-cell in small intestine, which has been shown to supress appetite and decrease body weight, delay gastric emptying, stimulate gastric acid inhibition. Circulating levels of GLP-1 rise following a meal in proportion to energy intake and are low in the fasted state can also improve glycaemic control by acting as an incretin hormone that triggers pancreatic β-cells to secrete insulin in a glucose-dependent manner [22, 26].
Ghrelin is an orexigenic peptide released by the stomach, which act as a meal initiator. Increase appetite and food intake in both lean and obese individuals, it also stimulates the release of growth hormone. Circulating ghrelin concentrations are increased by fasting and decreased after a meal [26].
Leptin a satiety hormone released from adipose tissue, helps in regulating food intake (inhibiting hunger) and energy expenditure. Leptin aids in regulation of energy balance, food intake suppression and thus inducing weight loss. It also stimulates the anorexigenic POMC-expressing neurons, within the hypothalamic ARC. Nonetheless, leptin has been shown to inhibit the orexigenic NPY/AgRP co-expressing neurons [26, 28]. Insulin is secreted from beta cell in pancreas, stimulates glucose homeostasis and can decrease food reward [23]. Insulin may have an anorectic action along with its hypoglycaemic effects, also Insulin is considered to work in the ARC by inhibiting NPY/AgRP co-expressing neurons. Increased adiposity, like leptin, can contribute to a reduction in insulin sensitivity and a condition of insulin resistance [22, 26].
While women bear the brunt of obesity-related fertility issues, this problem afflicts obese men as well [29]. Men who are grappling with this challenge, there are some foods which have been shown to bolster fertility by improving sperm count. Lycopene, a phytochemical that is known for its antioxidant property is abundant in tomatoes and watermelon. The latter is one of the foods that help to boost fertility among obese males [30]. Lycopene has also proven to be vastly effective than such other nutrients in Moringa. Moringa oleifera is another plant that is traditionally used as part of male fertility treatment [30]. Therefore, obese men should seriously consider including nutrient-dense functional foods into their diets. On the other hand, vitamins play an essential role in improving the fertility of men who are struggling with obesity. Vitamin D has proven particularly vital in improving sperm count [31, 32]. Oily fish, egg yolks, and some fortified food varieties [e.g., breakfast cereals] are among the rich sources of Vitamin D [33].
It is true that obese individuals should give particular attention to the nutritional content of the foods they consume. However, they should also recognize the crucial role that caloric composition [including portion size] plays in influencing their fertility and overall health. Experts strongly advise that obese individuals, women in particular, who wish to create families should focus their efforts on lowering the consumptions of high carbohydrate and fat content foods [34]. (The recommended daily carbohydrate intake for adults in the UK is 260g [35].
This measure functions to improve fertility by helping the individuals to reduce their weight in a safe, sustainable, and healthy manner.
It should be noted that the foods listed above do not necessarily guarantee successful pregnancies among obese women. Research evidence showed that being obese undermines the effectiveness of the different solutions that are administered onto women with the goal of improving pregnancy outcomes or enhancing reproductivity [36]. The dietary modifications should therefore be combined with other solutions that allow these women to achieve healthier body weights. As will be discussed in later section, physical activity and exercise are among the measures that amplify the beneficial impacts of dietary modification.
Testosterone Balance
Obesity goes beyond merely altering the storage and production of the sex hormones that are vital for fertility. This condition has been cited among the key drivers of drop in testosterone level among men. Essentially, since men usually have high fat percentages (>25% in males) [37], obese men metabolise testosterone by their fat cells that then create estrogen [38]. For obese men with low testosterone levels (< 8.7 nmol/L) [39], a number of undesirable and adverse outcomes are common, e.g., low sex drive, body hair loss, lean muscle mass loss, depression, obesity, and fatigue, to mention a few [40]. These negative outcomes will undoubtedly impact the quality of life of obese men whose lifestyles are largely sedentary. Dietary modification is regarded as the ultimate solution that improves their testosterone levels.
There is a wide range of foods that serve crucial functions in increasing the amount of testosterone for example, oysters, oily fish (e.g., salmon), crab, lobster, and beans, are among the rich sources [41], also Ashwagandha root, fenugreek seed extracts, Tribulus terrestris [42]. Furthermore, leafy vegetables like kale, extra virgin olive oil, onions, ginger are also believed to address low testosterone levels [43]. Conversely, excessive alcohol intake, canned, fried and processed foods can undermine efforts of obese men to increase their testosterone levels and should therefore be avoided [44, 45].
While obese individuals should regard foods as their first line for boosting testosterone, they may also turn to other remedies that deliver comparable benefits. Herbs are among some of the ingredients that play an essential role in ameliorating low testosterone levels. Ashwagandha root and fenugreek seed extracts are herbs that increase testosterone levels [42]. However, these herbs should be consumed with extreme caution since few numbers of research that have been conducted to determine their safe limits. Hence, before using the herbs, obese men should consult their practitioners to eliminate any risk of exacerbating existing medical conditions. Tribulus terrestris and longjack root are herbs that are believed to increase testosterone levels among men [46, 47].
On the other hand, supplements that purport to boost testosterone concentrations are not problems-free. Despite their popularity, there is little evidence confirming that supplements are effective and perhaps not posing any serious threat to public health. In fact, the few studies that have examined the efficacy and safety of the supplements have determined that in addition to being potentially dangerous, they are also ineffective, and should therefore be avoided whenever possible [48]. Among the key components that make up these supplements include vitamin B5 and B3, zinc, and magnesium. The following table summarise different sources of testosterone that obese men can rely upon to improve their sexual health, fertility, and overall wellness.
Estrogen Imbalance
Men are not the only group that experiences endocrinal disruptions that obesity is known to trigger. Women suffer as well. Unlike men whose testosterone levels have been shown to drop when they become obese, women health status is influenced by the positive relationship between estrogen and obesity. Experts believe that estrogen level serves as crucial function in increasing the risk of becoming obese among women [49].
Estrogen imbalances can lead to several debilitating health outcomes. A higher risk of contracting urinary tract infection, breast tenderness, mood swings, hot flashes, depression, fatigue, and migraines are some of the negative symptoms that low estrogen levels may trigger [50], (Table 3) Left unaddressed, these conditions and symptoms can fester and become more serious. Therefore, as they strive to lead healthier lives, obese women should leverage the power of adequate nutrition to ensure balance in their estrogen levels.
| For premenopausal females (pg/mL) | For postmenopausal females (pg/mL) | For males (pg/mL) | |
|---|---|---|---|
| Normal Estradiol levels | 30 - 400 | 0 - 30 | Oct-50 |
Table 3: Normal ranges of human Estradiol [51].
It should be noted that age plays a significant role in influencing the relationship between estrogen and obesity. As noted above, generally, estrogen increases the likelihood of obesity. The situation is different among older women. For example, as they enter menopause, women have been observed to experience a dip in their estrogen levels [52]. As
a result, their risk of becoming obese rises sharply. For these women, foods that increase estrogen levels are essential and should therefore form a significant part of their diet.
There are numerous foods that contain nutrients which can help older obese women to increase their estrogen levels. For instance, plant-based diets have been shown to be particularly high in phytoestrogens compounds that serve an essential function in boosting estrogen. Some of the sources of these compounds include grape skin, citrus fruits, parsley, celery, kale, broccoli, onions, lettuce, tomatoes, green tea, chocolate, berries, apricots, soybeans, alfalfa, Edamame, pumpkin seeds, and tofu, among many others [53], (Table 4).
| Food | Estrogens (μg/100g) | Estrogens μg/Serving | |
|---|---|---|---|
| Serving Size | μg | ||
| Butter | 0.029 | 1tbsp | 0.0041 |
| Chicken | 0.0004-<0.005 | 3oz | 0.0003-0.0043 |
| Eggs | n.d.-0.14 | 50g | n.d.-0.07 |
| Fish (Herring, Crab) | <0.005 | 3Oz | <0.0043 |
| Meat/Beef | <0.005 | 3Oz | <0.0043 |
| Milk | 0.004-0.015 | 1cup | 0.009-0.0366 |
| Potatoes (White) | <0.005 | 1medium | <0.0055 |
| Soya been/Product | <0.012 | 3oz | <0.00102 |
| Turkey | 0.0004-0.003 | 3oz | 0.0000-0.0003 |
| Wheat | <0.012 | 45g | <0.0054 |
| Yogurt | 0.018 | 6oz | 0.0306 |
| Oil (Olive) | 0.005 | - | 0.00072 |
Table 4: Level of Estrogen hormone in common foods.
Moreover, the benefits of the phytoestrogens extend beyond merely boosting estrogen levels. Evidence shows that these nutrients help to alleviate symptoms of ailments that accompany menopause, play an important role in the prevention of osteoporosis and improve cardiovascular health [53]. However, obese women who turn to these nutrients for relief should be wary of some adverse impacts. For example, researchers reported that phytoestrogens may increase risk of developing breast cancer in women especially in Western countries compared to Far-East countries [53].
Phytoestrogens occur in two primary varieties: lignans and isoflavones. On the one hand, lignans encompass the enterodiol and enterolactone metabolites. In addition to increasing estrogen concentrations, foods that contain these compounds have also been credited with having antitumor and antioxidant properties [54]. Nuts, wholegrains, and fruits are some examples of lignans-rich foods. These foods are particularly popular in Western nations where they are available in abundant supply and contribute as significant element of the diet. On the other hand, isoflavones encompass such food classes as genistein and daidzein and are contained in foods like tofu and beans [55]. Unlike lignans which are particularly consumed in the West, the isoflavones have formed part of Eastern diets for many generations.
For the most part, the foods outlined above are safe and facilitate the balance of estrogen. However, non-Asian women who consume these foods should exercise caution and understand that foods may carry some risk of adverse outcomes. For example, there is evidence that soya disrupts the normal and proper functioning of thyroid hormones [56]. Furthermore, while it can mimic the impact of estrogen, soya has been blamed for disturbing the menstrual age of women in some parts of the globe. Given the potential negative effects associated with soya, women are advised to consider obtaining their estrogen-balancing nutrients from other sources as outlined in Table 3.
Combating Aging
Accelerated aging is among the many negative outcomes of obesity. Research has established that by compromising the immune system, reducing telomere length, and exposing individuals to a higher risk of developing age-related ailments, obesity fast-tracks the aging process [57]. The latter is defined as the gradual aging which is a continuous process of natural change that begins in early adulthood. During early middle age, many bodily functions begin to gradually decline. People do not become old or elderly at any specific age. Traditionally, age 65 has been designated as the beginning of old age [58].
Fortunately, for obese men and women, there are some nutritional solutions that they can adopt to decelerate aging. The Mediterranean diet which is discussed in greater detail in a later section is comprised of foods that have been demonstrated to slow down the aging process [59].
Another important aspect of aging is the fact that as individuals approach older adulthood, they are more prone to experiencing hormonal imbalances and disorders. For example, in addition to reducing levels of such hormones as estrogen, testosterone, growth hormones, and melatonin, aging also decreases amounts of cortisol, insulin, and thyroid hormones [60]. Older obese adults (aged 65 years or over) should consume foods that allow them to restore balance in the levels of these hormones. Table 5 below summarizes some of the foods that can help to regulate and balance the hormones.
| Hormone | Food Sources |
|---|---|
| Estrogen | Grape skin, citrus fruits, parsley, celery, kale, broccoli, onions, lettuce, tomatoes, green tea, chocolate, berries, apricots, soybeans, alfalfa, Edamame, pumpkin seeds, and tofu [53]. |
| Testosterone | Oysters, such oily fish as salmon, crab, lobster, and beans [41]. |
| Melatonin | Salmon, chicken, eggs, dairy products [61]. |
| Cortisol | Bananas, green or black tea, probiotics found in foods like yoghurt [62]. |
| Insulin | Non-starchy vegetables, whole-grain foods, healthy fats found in avocadoes, olive oil, and canola oil [63]. |
| Thyroid hormones | Nuts, whole-grain foods, vegetables, fish, beans, healthy oils e.g., olive oil [64]. |
Table 5: List of food-containing metabolic hormone.
The Role of Calories
Earlier, it was made clear that even as they obsess over the type of foods that they consume, obese individuals should pay particular attention to their caloric intakes and expenditure. For many obese men and women, the calories that they consume are consistently higher than those that they expend through physical activity. While consuming nutrient-deficient foods [e.g., food rich in high fat, sugar and or salt] is among the key drivers of obesity, experts concur that an overall caloric surplus also contributes to the development of this condition [65]. Obese individuals should attempt to monitor their caloric intake and output. Today, there are countless applications that can be installed on smart mobile devices that help with this function. However, research has established that these programmes are largely ineffective and that obese individuals who are desperate to lose weight should turn to their friends and families for motivation [66].
Weight loss or weight gain can be thought of in strict relation to caloric balance. If you eat more calories than you burn, you gain weight and vice versa for losing it. This has recently led to the rise in fad diets whose claims take advantage of caloric intake to allow you to continue to eat unhealthy food while losing weight, just because these diets can be effective in helping you lose weight does not mean they are healthy. Therefore, some individuals would follow trending fad diets for fast weight loss despite the unstainable and temporary results, and it could deteriorate their health status [67].
Therefore, to successfully intercept obesity, individuals should be prepared to combine tuned nutritional intake to their requirements with lifestyle modifications and abandoning sedentary lifestyles in favour of physical activity. A recommended exercise duration of 150 minutes per week (moderate intensity as in Table 6) can aid in preventing and reducing obesity [68].
| VO2 max (%) | Heart rate max (%) | |
|---|---|---|
| Low | 20 - 39 | 50 - 63 |
| Moderate | 40 - 59 | 64 - 76 |
| Vigorous | 60 - 84 | 77 - 93 |
Table 6: Physical activity intensity with its relative heart rate categories [69].
Mediterranean and DASH Diets
A clearer understanding of the role that nutrition plays in the prevention and management of obesity can be gained by deeply exploring some diets that have proven tremendously popular and are quickly gaining traction. The Mediterranean and the DASH diets are among these.
Mediterranean Diet
As indicated above, the Mediterranean diets are among the food movements that are sweeping the globe today. Essentially, this diet is comprised of vegetables, legumes, beans, grains, cereals, unsaturated oils, and fish, among other healthy choices [70]. Mediterranean diet pyramid comprises of daily intake of non-refined cereals, whole grain foods, vegetables (2-3 servings) and fruits (4-6 servings) [71, 72]. The benefits of this diet are varied and numerous. For example, experts have determined that the Mediterranean diet helps to prevent cardiovascular diseases, promotes healthy aging, and increases one’s lifespan [73]. While it is largely beneficial, the Mediterranean diet presents some significant risks and pitfalls of which obese individuals who wish to adopt it should be cautious. Despite these adverse impacts, overall, the Mediterranean diet is beneficial and obese individuals are strongly advised to consider incorporating it into their lifestyles.
DASH Diet
Apart from the Mediterranean diet, obese individuals may also turn to the DASH diet as part of their efforts to shed weight and lead healthier lives. Spelt out as Dietary Approaches to Stop Hypertension, as this name suggests, the DASH diet is essentially a plan that was originally developed with the goal of helping hypertensive individuals to manage their symptoms. In addition to advising individuals on the foods to include in their diets, the DASH plan also provides guidelines regarding portion sizes, which represents a starting point to those who wish to lose some kilograms of their body weight to improve their hypertension and overall health status. Vegetables, whole grains, fruits, low-fat dairy products, beans, vegetables, nuts, and poultry are some of the foods that make up the DASH diet [74]. Table 7 illustrates the respective portion sizes and servings for the different foods. Multiple studies have concluded that both the DASH and Mediterranean diets support healthy sustainable lifestyles, including physical and nutritional health.
| Food | Daily servings |
| Grains | 8-Jun |
| Meats, poultry, and fish | 6 or less |
| Vegetables | 5-Apr |
| Fruits | 5-Apr |
| Low-fat or fat-free dairy products | 3-Feb |
| Fats and oils | 3-Feb |
| Sodium | 2,300 mg |
Table 7: Selected common food items shown in DASH diet as well as Medi diet.
For the most part, the foods recommended in the discussion this far are safe and effective for a large majority of the adult obese population. However, for certain vulnerable groups, modifications and considerations need to be made. Among these groups are individuals living with such conditions as diabetes and hypertension. For this group of individuals, the various diets that are normally safe should be fine-tuned to minimize the risk of adverse outcomes. Diabetic individuals are strongly urged to adopt diets rich in vegetables, fruits (berries, apples, melons, tomatoes, peppers), grains (oats, cornmeal, quinoa, wheat), protein (lean meat, nuts, fish, chicken, tofu), and dairy products (yoghurt, cheese, milk) [75]. These patients should minimize their consumption of foods that are high in unhealthy saturated fats and refined carbohydrates. On the other hand, for those with hypertension, it is recommended that their diets should be composed of foods like skimmed milk, lean meat, cooked cereal, plain rice, breads, skinless chicken and turkey, vegetables, and fruits.
Portion Size Control
When consumed in excessive amounts, even foods that should be healthy can have negative impacts and exacerbate obesity. For this reason, it is important for individuals to control their portion sizes. Portion control has emerged among the most effective strategies for weight management [76]. As part of their efforts to limit their portion sizes, obese individuals can institute such simple and practical measures as weighing their food or using smaller plates.
Lifestyle Interventions
The first part of this article described the nutritional measures that obese individuals with sedentary lifestyles can adopt. At this point, the article shifts focus toward some of the lifestyle nutrition interventions that are available to sedentary, obese individuals to practice. Some of these measures are outlined in Table 8 and discussed below.
| Omnivores/ *Vegetarian and Vegan | |
|---|---|
| Food groups | servings per day |
| Protein | ≤ 6 (6 ορ λεσσ) |
| Carbs/grains | 8-Jun |
| Fat/oils | 3-Feb |
| Veggies | 5-Apr |
| Fruits | 5-Apr |
| Dairy* (Low fat preferable) | 3 |
| Nuts/seeds/olives | 2-Jan |
| Sodium | 2.300mg |
| 1.500 mg (better for reducing blood pressure) | |
| Sugar/sweets (substituted with min dried fruits) | 2 or less weekly |
| Target calorific value | For males: 2100-2300 calories |
| For females: 1700-1900 calories | |
| Physical Activity recommendations | 150 minutes per week (moderate intensity exercise)** |
| Blue exercise | Natural Aquatic/ marine environment: Swimming, surfing, rowing, sailing, and canoeing, kayaking, rafting |
| Green Exercise | Outdoor in nature, parks, garden Walking, running |
Table 8: Proposed meal planning that emphasising ranges of daily servings and sizes of different food preferences integrated w
* Vegetarian and vegan milk replacement/plant-based milks could be: almond, soy, oat, coconut See (Table 6) above the intensity of physical activity Table 8:** Proposed meal planning that emphasising ranges of daily servings and sizes of different food preferences integrated with physical activity guidelines.
Physical Activity
There are ample of evidence that physical activity is among the simplest and most sustainable solutions that obese individuals may implement [77]. For those whose lifestyles are rather sedentary, physical exercise offers a platform to escape obesity. Even a limited amount of physical engagement can present tremendous benefits. Physical activity primarily helps in the prevention and the management of obesity, it has been linked to numerous other positive outcomes. For example, individuals who take part in some form of physical activity lower their risk of heart attacks, make better progress in managing their weight, report significant reduction of cholesterol levels, record lower blood pressure, and reduce the likelihood of suffering from osteoporosis, one of the conditions that often afflicts obese adults [78]. Therefore, as part of their weight management and health improvement programs, obese adults should consider embracing physical activity. According to WHO (2020), the latest physical activity guidelines for individuals aged between 18-64 years old is to engage in at least 150–300 minutes of moderate-intensity aerobic exercise [79].
Today, there are many avenues and resources that individuals can exploit as part of their efforts to lose weight. For example, authorities are constructing parks and other public spaces with the goal of encouraging their citizens to increase their engagement in physical activity. Essentially, obese individuals have a wide array of platforms and tools that they can exploit. However, as noted earlier, during the pandemic, these resources are in limited use, hence for obese individuals working out from the comfort of their homes could be a more convenient and affordable alternative to joining gyms. Moreover, there are many different applications that individuals can install on their mobile devices. In addition to providing motivation, these applications offer clear guidelines and milestones that could help obese individuals to achieve their target body weight and general health goals.
Accounting for the Impact of Genetics
As made clear above, physical activity and exercise is an effective approach for obese individuals who are keen on losing weight. However, there is a need to understand that the outcomes of physical exercise vary from one person to the other, depending on their genetic makeup.
Nutrigenetics and nutrigenomics are branches of knowledge that provide information on mechanisms of nutrient and gene interactions in both health and disease required for personalized nutrition to the public [80, 81].
Nutrigenomics explores the interaction between nutrients and genes and their outcomes on human health, while Nutrigenetics looks how genes impact to the dietary response [81, 82]. Many foods and different dietary patterns have been studied in nutrigenetics and nutrigenomics data for example the Mediterranean diet pattern, there are plenty of research demonstrate that the Mediterranean diet can have genome interaction therefore lowering the disease risk and having a protective effect among individuals who are genetically susceptible [83].
Genetics is among the factors that explains this variability. For example, by shaping one’s cardiorespiratory fitness and their metabolic response, genetics heavily determines whether physical exercise results in any significant weight loss [84]. Therefore, obese individuals who begin to engage in physical exercise should measure their expectations and understand that impressive results are not guaranteed. It is also crucial for these individuals to exhibit patience and recognize that positive outcomes require persistence and consistently committing time and effort to exercising.
Dietary Modifications Combined with Physical Exercise
On its own, physical exercise may not be enough to generate significant declines in the weights of individuals struggling with obesity. In fact, a recent study revealed that without corresponding dietary changes, individuals should not expect to experience any meaningful weight loss [85]. Spices like ginger mix, chilipeppers, cayenne pepper, coffee, tea, cocoa, apple cider vinegar, seaweed, are other foods that can improve physical exercise by boosting metabolism and fat oxidation [86]. Thus, as part of their exercise and weight- loss programs, obese adults who currently lead sedentary lifestyles should consider incorporating these foods into their diets
Pharmaceutical Interventions
Physical exercise and nutrition should be the first- line solutions for weight management among obese adults (BMI > 40 Kg/m2) with sedentary lifestyles. However, it is possible that these interventions may not be enough to guarantee weight loss. When physical exercise and dieting prove ineffective, the individuals may be forced to resort to pharmaceutical approaches. At present, there are several medications that healthcare practitioners may prescribe as a last resort. They include Orlistat, Lorcaserin, Phentermine- topiramate, Naltrexone-bupropion, and Liraglutide, among others [87]. These drugs function primarily by suppressing appetite. While they can have some benefit, the medications should be taken alongside nutritional modifications as well as physical activity for their impact to be sustained over the long-term.
Surgical procedures are also available for adults for whom the other solutions have proven not conclusive. For example, bariatric surgery is gaining popularity globally. In addition to helping individuals to lose weight, bariatric surgery has also been associated with reduced likelihood of developing cardiovascular disease and enhanced metabolic, respiratory, and musculoskeletal processes [88]. However, bariatric surgery may cause serious complications that can even result in death. Therefore, this option should only be reserved for patients who have not experienced any real benefit from dietary modification, physical activity, and medications.
Factors Impacting Effectiveness of Interventions
The implementation of the different interventions discussed above does not occur in a vacuum. There are various factors that influence whether these solutions achieve their intended purpose. Cost-benefits is among these factors. Naturally, the more cost-effective measures like dietary modifications are easier to incorporate into one’s lifestyle. On the other hand, the pharmaceutical solutions could be prohibitively costly and are therefore more difficult to adopt. The availability of the different strategies is yet another issue that determines their outcomes. For instance, the physical environment: Individuals in areas where healthy foods are in abundant supply are better positioned to make wise choices about their health. In contrast, those in food deserts are essentially forced to consume empty calories [i.e., energy-dense] foods that are available in greater quantities. The support system to modify behaviour that one has in place heavily shapes the results of such strategies as physical exercises. For the best outcomes, obese individuals should turn to their social circles for encouragement and motivation. When implemented properly, the different interventions can deliver tremendous results. However, none of these solutions can function properly unless accompanied by drive and motivation. Obese adults must make the decision to eat healthier foods, begin involvement in physical exercises, and if necessary, seeking treatment for their condition.
Conclusion
Obesity continues to plague the world, recording sharp rises in the prevalence of obese populations. What is particularly worrying is that in addition to affecting adults, obesity now afflicts millions of children across the globe. This condition presents a real danger to public health. In addition to limiting, one’s quality of life, being obese also increases an individual’s risk of developing a wide range of conditions that include type 2 diabetes and heart disease. There is a clear and urgent need for nations to work together in addressing obesity.
Healthier diets [Mediterranean and DASH] have consistently been shown to be among the solutions that can help to reduce the rate of obesity. Balanced nutrient intake tackles obesity through several mechanisms. In addition to restoring hormonal balance, healthier selection of nutraceutical foods plays crucial role in slowing down the rate of aging. Furthermore, when substituting unhealthy foods with healthier options, obese individuals spare themselves the high cost of treatment that they otherwise require when their obesity gives rise to complications.
Nutrition intervention is just one of several strategies that obese adults with sedentary lifestyles can use to improve their condition. Physical exercise is another instrument that has proven tremendously effective in tackling obesity. However, on its own, physical activity may not be enough. It should be implemented together with nutritional and behavioural modifications. When these solutions fail, obese adults may resort to medications and surgery.
The responsibility of tackling obesity rests with individuals and their own practices and actions. However, governments should recognize that they have important roles to play in addressing the obesity epidemic such as investments in resources and recreational facilities like parks to sensitize the public regarding the importance of physical exercise and healthy diets. With the help of different stakeholders executing their responsibilities, the globe will certainly make faster progress in its ‘war’ against obesity and sedentary lifestyles.
References
-
Centers for Disease Control and Prevention (CDC) (2020) The health effects of overweight and obesity.
-
Centers for Disease Control and Prevention (CDC) (2021) Adult Obesity Causes & Consequences.
-
World Health Organization (WHO) (2021) Obesity and overweight key facts.
-
Hamer M, Gale CR, Kivimaki M, Batty GD (2020) Overweight, obesity, and risk of hospitalization for COVID-19: A community-based cohort study of adults in the United Kingdom. Proc Natl Acad Sci U S A 117(35): 21011-21013.
-
Hippisley-Cox J, Young D, Coupland C, Channon KM, Tan PS, et al. (2020) Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: cohort study including 8.3 million people. Heart 106(19): 1503- 1511.
-
Niehoff V (2009) Childhood Obesity: A Call to Action. Bariatric Nursing and Surgical Patient Care 4(1): 17-23.
-
Gray CL, Messer LC, Rappazzo KM, Jagai JS, Grabich SC, et al. (2018) The association between physical inactivity and obesity is modified by five domains of environmental quality in U.S. adults: A cross-sectional study. PLoS One 13(8): e0203301.
-
Ten Hacken NH (2009) Physical inactivity and obesity: relation to asthma and chronic obstructive pulmonary disease? Proc Am Thorac Soc 6(8): 663-667.
-
Kuźbicka K, Rachon D (2013) Bad eating habits as the main cause of obesity among children. Pediatr Endocrinol Diabetes Metab 19(3): 106-110.
-
Rush EC, Yan MR (2017) Evolution not Revolution: Nutrition and Obesity. Nutrients 9(5): 519.
-
Segula D (2014) Complications of obesity in adults: a short review of the literature. Malawi Med J 26(1): 20-
-
Dalle Grave R, Sartirana M, Calugi S (2020) Personalized cognitive-behavioural therapy for obesity (CBT-OB): theory, strategies and procedures. Biopsychosoc Med 14: 5.
-
Seth B, Arora S, Singh R (2013) Association of obesity with hormonal imbalance in infertility: a cross-sectional study in north Indian women. Indian J Clin Biochem 28(4): 342-347.
-
Gambineri A, Laudisio D, Marocco C, Radellini S, Colao A, et al. (2019) Female infertility: which role for obesity? Int J Obes Suppl 9(1): 65-72.
-
Panth N, Gavarkovs A, Tamez M, Mattei J (2018) The Influence of Diet on Fertility and the Implications for Public Health Nutrition in the United States. Front Public Health 6: 211.
-
Practice Committee of the American Society for Reproductive Medicine (2015) Obesity and reproduction: a committee opinion. Fertil Steril 104(5): 1116-1126.
-
Nazni P (2014) Association of western diet & lifestyle with decreased fertility. Indian J Med Res 140: S78-S81.
-
Szokan N (2015) Can a high-protein, low-carb diet increase fertility in women? The Washington Post, USA.
-
Gunnars K (2021) Pros and Cons of 5 Intermittent Fasting Methods. Healthline.
-
Grajower MM, Horne BD (2019) Clinical Management of Intermittent Fasting in Patients with Diabetes Mellitus. Nutrients 11(4): 873.
-
Barnosky AR, Hoddy KK, Unterman TG, Varady KA (2014) Intermittent fasting vs daily calorie restriction for type 2 diabetes prevention: a review of human findings. Transl Res 164(4): 302-311.
-
Suzuki K, Jayasena CN, Bloom SR (2011) The gut hormones in appetite regulation. J Obes 2011: 528401.
-
Figlewicz DP (2015) Modulation of Food Reward by Endocrine and Environmental Factors: Update and Perspective. Psychosom Med 77(6): 664-670.
-
Murphy KG, Bloom SR (2006) Gut hormones and the regulation of energy homeostasis. Nature 444: 854-859.
-
Zanchi D, Depoorter A, Egloff L, Haller S, Mahlmann L, et al. (2017) The impact of gut hormones on the neural circuit of appetite and satiety: A systematic review. Neurosci Biobehav Rev 80: 457-75.
-
Perry B, Wang Y (2012) Appetite regulation and weight control: the role of gut hormones. Nutr Diabetes 2(1): e26.
-
Williams DL (2014) Neural integration of satiation and food reward: role of GLP-1 and orexin pathways. Physiol Behav 136: 194-199.
-
Klok MD, Jakobsdottir S, Drent ML (2007) The role of leptin and ghrelin in the regulation of food intake and body weight in humans: a review. Obes Rev 8(1): 21-34.
-
Sermondade N, Faure C, Fezeu L, Levy R, Czernichow S, et al. (2012) Obesity and increased risk for oligozoospermia and azoospermia. Arch Intern Med 172(5): 440-442.
-
Greish SM, Abdel Kader GS, Abdelaziz EZ, Eltamany DA, Sallam HS, et al. (2021) Lycopene is superior to moringa in improving fertility markers in diet-induced obesity male rats. Saudi J Biol Sci 28(5): 2956-2963.
-
Arab A, Hadi A, Moosavian SP, Askari G, Nasirian M (2019) The association between serum vitamin D, fertility and semen quality: A systematic review and meta-analysis. Int J Surg 71: 101-109.
-
Cito G, Cocci A, Micelli E, Gabutti A, Russo GI, et al. (2020) Vitamin D and Male Fertility: An Updated Review. World J Mens Health 38(2): 164-177.
-
National Health Service (NHS) (2020) Vitamin D. England, UK.
-
Best D, Avenell A, Bhattacharya S (2017) How effective are weight-loss interventions for improving fertility in women and men who are overweight or obese? A systematic review and meta-analysis of the evidence. Hum Reprod Update 23(6): 681-705.
-
National Health Service (NHS) (2020) Reference intakes explained-Eat well, Carbohydrate. England, UK.
-
Silvestris E, Lovero D, Palmirotta R (2019) Nutrition and Female Fertility: An Interdependent Correlation. Front Endocrinol Lausanne 10: 346.
-
ACE (2009) What are the guidelines for percentage of body fat loss? American Council on Exercise, San Diego, California, USA.
-
Fui MN, Dupuis P, Grossmann M (2014) Lowered testosterone in male obesity: mechanisms, morbidity and management. Asian J Androl 16(2): 223-231.
-
National Health Service (NHS) (2021) Testosterone. NHS North Bristol, Bristol, UK.
-
Urology Care Foundation (UCF) (2021) What is low testosterone? American urological Association.
-
Levine D (2021) Foods that raise testosterone levels. US News (Food).
-
Smith SJ, Lopresti AL, Teo SYM, Fairchild TJ (2021) Examining the Effects of Herbs on Testosterone Concentrations in Men: A Systematic Review. Adv Nutr 12(3): 744-765.
-
Butler N, Leonard J (2020) Best foods for increasing low testosterone. Medical News Today.
-
Vignera SL, Condorelli RA, Balercia G, Vicari E, Calogero AE (2013) Does alcohol have any effect on male reproductive function? A review of literature. Asian J Androl 15(2): 221-225.
-
Kurniawan AL, Hsu CY, Rau HH, Lin LY, Chao JC (2019) Dietary patterns in relation to testosterone levels and severity of impaired kidney function among middle- aged and elderly men in Taiwan: a cross-sectional study. Nutr J 18(1): 42.
-
Pokrywka A, Obminski Z, Malczewska-Lenczowska J, Fijalek Z, Turek-Lepa E, et al. (2014) Insights into Supplements with Tribulus Terrestris used by Athletes. J Hum Kinet 41: 99-105.
-
Gunnels TA, Bloomer RJ (2014) Increasing Circulating Testosterone: Impact of Herbal Dietary Supplements. J Plant Biochem Physiol 2(2): 130.
-
Clemesha CG, Thaker H, Samplaski MK (2020) ‘Testosterone Boosting’ Supplements Composition and Claims Are not Supported by the Academic Literature. World J Mens Health 38(1): 115-122.
-
Leeners B, Geary N, Tobler PN, Asarian L (2017) Ovarian hormones and obesity. Hum Reprod Update 23(3): 300- 321.
-
Sullivan D (2018) What are the symptoms of low estrogen in women and how are they treated? Health line.
-
UOF (2021) Estradiol (Blood). University of Rochester, Rochester, New York.
-
Lizcano F, Guzman G (2014) Estrogen Deficiency and the Origin of Obesity during Menopause. Biomed Res Int 2014: 757461.
-
Patisaul HB, Jefferson W (2010) The pros and cons of phytoestrogens. Front Neuroendocrinol 31(4): 400-419.
-
Li X, Yuan JP, Liu X, Wang JH (2006) Lignan: an important natural estrogen from plants. Zhongguo Zhong Yao Za Zhi 31(24): 2021-2025,2093.
-
Hui E, Henning SM, Park N, Heber D, Liang V, et al. (2001) Genistein and Daidzein/Glycitein Content in Tofu. Journal of Food Composition and Analysis 14(2): 199-206.
-
Messina M, Redmond G (2006) Effects of soy protein and soybean isoflavones on thyroid function in healthy adults and hypothyroid patients: a review of the relevant literature. Thyroid 16(3): 249-258.
-
Tam BT, Morais JA, Santosa S (2020) Obesity and ageing: Two sides of the same coin. Obesity Reviews 21(4): e12991.
-
Besdine RW (2019) Overview of Aging. MSD, Canada, US.
-
Capurso C, Bellanti F, Buglio AL, Vendemiale G (2019) The Mediterranean Diet Slows Down the Progression of Aging and Helps to Prevent the Onset of Frailty: A Narrative Review. Nutrients 12(1): 35.
-
Morley JE (2020) Effects of aging on the endocrine system. MSD Manual, Canada, US.
-
Meng X, Li Y, Li S, Zhou Y, Gan RY, et al. (2017) Dietary Sources and Bioactivities of Melatonin. Nutrients. 9(4): 367.
-
Murrell D (2020) How to remove cortisol from the body naturally. Medical News Today, Brighton, East Sussex.
-
Marengo K (2019) Which foods help stabilize insulin and blood sugar? Medical News Today, Brighton, East Sussex.
-
Harvard Medical School (HMS) (2017) Healthy eating for a healthy thyroid. Boston, MA.
-
Taubes G (2013) What makes you fat: Too many calories, or the wrong carbohydrates? Scientific American.
-
Solbrig L, Jones R, Kavanagh D, May J, Parkin T, et al. (2017) People trying to lose weight dislike calorie counting apps and want motivational support to help them achieve their goals. Internet Interv 7: 23-31.
-
Khawandanah J, Tewfik I (2016) Fad Diets: Lifestyle Promises and Health Challenges. Journal of Food Research 5(6): 80-94.
-
NICE Guidelines (2013) Obesity recommendations.
-
American College of Sports Medicine (ACSM) (2014) ACSM’s Guidelines for Exercise Testing and Prescription. J Can Chiropr Assoc 58(3): 328.
-
National Health Service (NHS) (2020) What is a Mediterranean diet? Dietetics.
-
Willett WC, Sacks F, Trichopoulou A, Drescher G, Ferro- Luzzi A, et al. (1995) Mediterranean diet pyramid: a cultural model for healthy eating. Am J Clin Nutr 61(Suppl 6): 1402S-1046S.
-
Panagiotakos DB, Pitsavos C, Stefanadis C (2006) Dietary patterns: a Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr Metab Cardiovasc Dis 16(8): 559-568.
-
Tosti V, Bertozzi B, Fontana L (2018) Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J Gerontol A Biol Sci Med Sci 73(3): 318- 326.
-
National Heart Lung and Blood Institute, NIH (2021) DASH eating plan. USA.
-
National Institute of Diabetes and Digestive and Kidney Diseases, NIH (2016) Diabetes diet, eating & physical activity. USA.
-
Rolls BJ (2014) What is the role of portion control in weight management? Int J Obes Lond 38(Suppl 1): S1-S8.
-
Kim BY, Choi DH, Jung CH, Kang SK, Mok JO, et al. (2017) Obesity and Physical Activity. J Obes Metab Syndr 26(1): 15-22.
-
Better Health Channel (BHC) (2018) Physical activity- it’s important. Victoria State Government.
-
World Health Organization (WHO) (2020) Physical activity. USA.
-
Simopoulos AP (2010) Nutrigenetics/Nutrigenomics. Annu Rev Public Health 31: 53-68.
-
Fenech M, El-Sohemy A, Cahill L, Ferguson LR, French TA, et al. (2011) Nutrigenetics and nutrigenomics: viewpoints on the current status and applications in nutrition research and practice. J Nutrigenet Nutrigenomics 4(2): 69-89.
-
Farhud D, Yeganeh MZ, Yeganeh MZ (2010) Nutrigenomics and Nutrigenetics. Iran J Public Health. 39(4): 1-14.
-
Corella D, Barragan R, Ordovas JM, Coltell O (2018) Nutrigenetics, nutrigenomics and Mediterranean diet: a new vision for gastronomy. Nutr Hosp 35(Spec No4): 19-27.
-
Bouchard C, Rankinen T, Timmons JA (2011) Genomics and genetics in the biology of adaptation to exercise. Compr Physiol 1(3): 1603-1648.
-
Belluz J, Zarrcina J (2017) Why you shouldn’t exercise to lose weight, explained with 60+ studies. Vox.
-
Petre A, Kubala J (2021) The 12 Best Foods to Boost Your Metabolism. Nutrition.
-
National Institute of Diabetes and Digestive and Kidney Diseases (2016) Prescription medications to treat overweight and obesity.
-
Panagiotou OA, Markozannes G, Adam GP, Kowalski R, Gazula A, et al. (2018) Comparative Effectiveness and Safety of Bariatric Procedures in Medicare-Eligible Patients: A Systematic Review. JAMA Surg 153(11): e183326.
- The Role of Podocyte Apoptosis and the Involvement of SIRT1 in Diabetic Nephropathy
- Dealcoholization of Beer by Osmotic Distillation for the Beverage Industry
- Biopolymer-Based Edible Packaging- Biomaterials, Methods, and Applications in Food Industry: An Updated Review
- Influence of Bioprocessing Methods on 'China Rice' (Gawal R1), and Soyabean Supplementation on the Quality of Complementary Food
- Cassava (Manihot esculenta) Varietal Growth, Yield and Cyanide Content Performance in Three Sites in the South- Eastern Semi Arid Regions of Kenya
- Food Waste Treatment, Recycling, Management and Production of Value-Products-An Update on Methodologies and Current Trends