Is Anti-HBs a Useful, Economic and Neglected Tool in the Hands of Hepatologist? A meta-analysis of Observational Studies of HBv past Infection Reactivation in Patients with Lymphoma
Reactivation of HBV is a well-recognized complication following immunosuppression, also in past HBV infection. Based on scientific literature, antiHBs status in HBsAg negative/anti HBc positive patients undergoing chemotherapy may reduce the risk for HBV reactivation, so antiHBs status should be included in a management alghorithm in patients with past HBV infection prior to starting immunosuppressive therapy.
Introduction
Reactivation of HBV may occur in individuals with past HBV Infection (serological recovery from infection: HbsAg negative, antiHBc positive and/or antiHBs positive). This reactivation (appearance of HbsAg or HBV DNA) is a well- recognized complication following systemic chemotherapy for hematological malignancies. In HBsAg-positive patients who are candidates for chemotherapy or treatment with biologic agents, preemptive treatment with an antiviral agent has become a standard of care, effectively preventing HBV reactivation. Conversely in patients with past HBV Infection the preemptive therapy is not universally accepted, so neither the screening for past HBV infection is routinely performed. The American Society of Clinical Oncology (ASCO) recommends screening using the HBsAg test, and in some cases the anti-HBc test, but does not endorse screening with anti-HBs [1]. The American Association for the Study of Liver Diseases (AASLD) recommends HBsAg and anti-HBc testing in patients who are at high risk of HBV infection prior to initiation of chemotherapy or immunosuppressive therapy. Whereas HBV reactivation in this population is considered as "infrequent", perhaps does not recommend routine prophylaxis for these individuals: These patients should be monitored and antiviral therapy initiated when serum HBV DNA becomes detectable [2]. The European Association for the Study of the Liver (EASL) recommends that HBsAg-negative, anti-HBc positive patients with undetectable serum HBV DNA, regardless of anti-HBs status, who receive chemotherapy and/or immunosuppressant, should be followed carefully by means of ALT and HBV DNA testing and treated with NA therapy upon confirmation of HBV reactivation before ALT elevation [3]. The Italian association for the Study of the Liver (AISF) recommends two different strategies: for mild haematological therapies HBsAg monitoring is advised, whereas in subjects treated with intense immunosuppressant prophylaxis is indicated [4]. However, these recommendations are based on little evidence. In a recent review on management of patients with hepatitis B who require immunosuppressive therapy the authors recommend a prophylactic antiviral therapy in HBsAg negative/anti HBc positive patients at moderate/higt risk of reactivation regarde less the anti HBs status [5]. So we performed a systematic review with the aim to research, at first, the relationship between HBV reactivation in HBsAg negative patients, with various neo plastic diseases of the lymphoid tissue undergoing chemotherapy, with anti-HBc positive OR anti-HBc negative status; and as second outcome the proportion of HBV reactivation in HBsAg negative/anti HBc positive patients with HBsAb positive OR HBsAb negative status.
Materials and Methods
Literature search
A literature search was conducted using Pubmed. The search was based on the following terms: ("HBV" OR "hepatitis b" OR "OBI") AND reactiva*. Titles and/or abstracts were screened by one of us (MF). Published studies from any date up to February 28, 2014 were included. No restriction was applied during the search, but only English language, as full papers, were included in the final review.
Inclusion and exclusion criteria
| Author, Journal, Year | Selection | Comparability | Outcome/Exposure |
|---|---|---|---|
| Masarone M BMC Gastroenterol. 2014 [6] | **** | ** | *** |
| Elkady A, World J Gastroenterol. 2013 [7] | *** | $\cdot$ | ** |
| Hsu C, Hepatology, 2013 [8] | **** | ** | *** |
| Matsui T, J Med Virol. 2013 [9] | *** | $\cdot$ | ** |
| Kim SJ, Eur J Cancer. 2013 [10] | *** | $\cdot$ | $\cdot$ |
| Koo YX, Ann Hematol. 2011 [11] | *** | ** | $\cdot$ |
| Matsue, Cancer 2010 [12] | *** | $\cdot$ | ** |
| Ji Eur J Haematol 2010 [13] | *** | $\cdot$ | ** |
Fiore M. Is Anti-HBs a Useful, Economic and Neglected Tool in the Hands of Hepatologist? A meta-analysis of Observational Studies of HBv Past Infection Reactivation in Patients with Lymphoma. Gastroenterol Hepatol Int J 2016, 1(2): 000108.
Copyright© Fiore M.
| Fukuschima Ann Oncol 2009 [14] | ** | $\cdot$ | |
| Yeo J Clin Oncol 2009 [15] | *** | $\cdot$ | ** |
| Hui, Gastroenterology 2006 [16] | *** | ** | ** |
Table 2: Quality assessment of non-randomized studies in meta-analysis.
Statistical Analysis
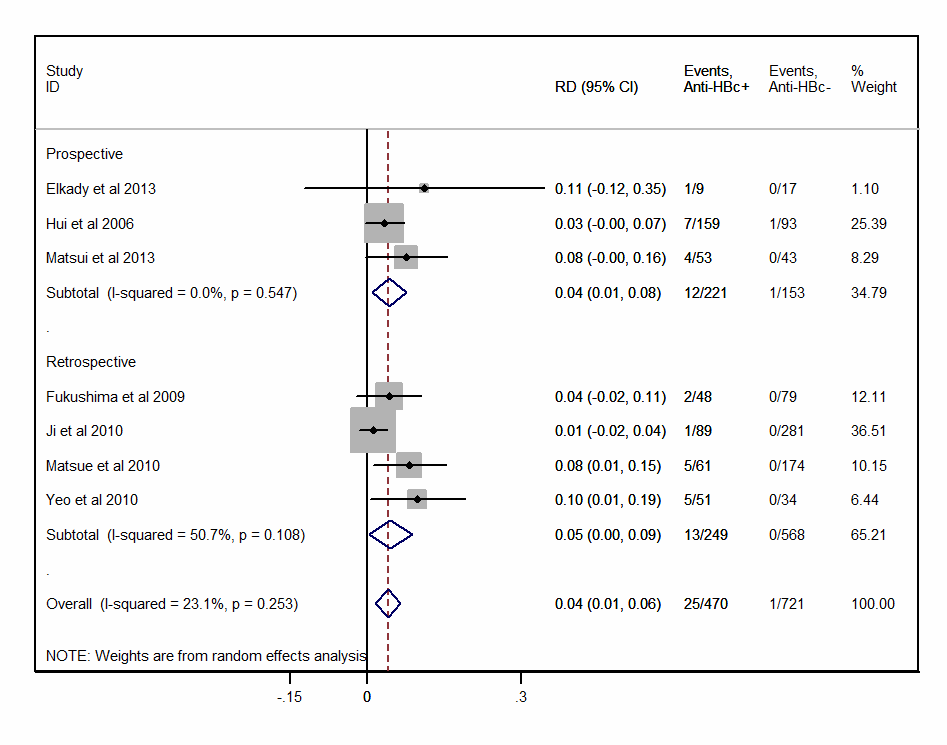
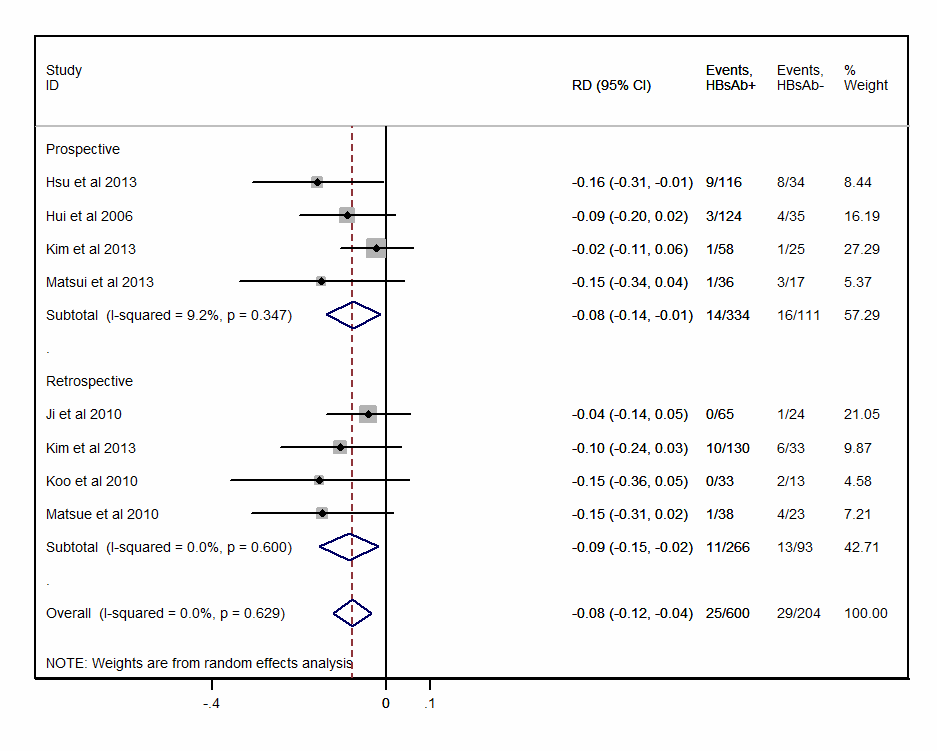
The primary outcome measures were proportions of reactivation in HBsAg negative patients with anti-HBc positive OR anti-HBc negative status. The secondary outcome measures were the proportion of reactivation in HbsAg negative/anti-HBc positive patients with HBsAb positive OR HBsAb negative Status. Analysis was stratified by study design (prospective vs. retrospective). Results were presented as Risk Differences (RDs) with 95% confidence intervals (CI) uses the Der Simonian and Laird random effect model, with the estimate of heterogeneity being taken from the inverse-variance fixed-effect model. The I2 statistic was used. We examined a funnel plot of the standard error of the RDs against the RDs to estimate potential publication bias we performed the Duval and Tweedier nonparametric "trim and fill" method of accounting for publication bias in meta-analysis [17]. The method estimates the number and outcomes of missing studies, and adjusts the meta- analysis to incorporate the theoretical missing studies. Computations were performed using STATA software.
Results
1226 papers were screened and (Figure 1) shows the flow chart. We further scrutinized the reference citations from the retrieved articles in order to avoid any missing data derived from any additional eligible studies that reported the prevalence of HBV reactivation in patients with various neo plastic diseases of the lymphoid tissue who recovered from HBV infection.
| Search in PUBMED: 1200 titles | |
|---|---|
| 350 case reports or case series | |
| 950 titles | |
| 303 letters, commentaries, editorials or reviews | |
| 647 titles | |
| 200 in vitro, conference, no relevant outcome studies | |
| 347 titles | |
| 230 studies on reactivation in HbsAg + patients | |
| 117 titles detailed reviews focused on reactivation in HbsAg – patients | |
| 11 elegible for the final analysis | |
| 1 study retracted | |
| 10 included in final analysis | |
| 7 reactivation in antiHBc+ vs. AntiHBc- | 7 antiHBC+ reactivation in HbsAb+ vs. HBsAb - |
On the basis of publication type 350 papers were excluded as case report or case series, 303 papers were excluded as Letter, comment, editorial or reviews. After Fiore M. Is Anti-HBs a Useful, Economic and Neglected Tool in the Hands of Hepatologist? A meta-analysis of Observational Studies of HBv Past Infection Reactivation in Patients with Lymphoma. Gastroenterol Hepatol Int J 2016, 1(2): 000108.
abstract reading another 200 paper were excluded because In vitro studies, conference abstract or no relevant outcome. After a full text review of 347 studies, Copyright© Fiore M.
230 were excluded because the argument was the HBV reactivation in HBsAg positive patients. Of the 117 titles remained, 11 were eligible for the final analysis but 1 article was retracted, so eleven articles are included in the final analysis [6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16] (Figure 1). Table 2 summarizes study characteristics. Results on the difference in risk of reactivation of past HBV infection in antiHBc positive and antiHBc negative, show a clear and significant increase of 4% (95%CI: 1%−6%, p- value=0.002) in antiHBc positive patients as compared to antiHBc negative patients (Figure 2). The asymmetry of funnel plot in Figure 3 suggests the presence of a publication bias. According to trim & fill analysis, the pooled RD would be reduced to 2.3% (p-value=0.09) As to the secondary endpoint, a statistically significant RD between anti-HBs positive and anti-HBs negative with pooled estimate = -8% (95%CI -12% − - 4%, p- value<0.001) (Figure 4) was found, confirmed by trim & fill method and visual inspection of funnel plot (Figure 5).
| Country | Study design | Reactivation defined as: | N° pz. | N° riactivated | Anti-HBc | Anti-HBc + | |||
|---|---|---|---|---|---|---|---|---|---|
| + | - | HbsAb+ | HBsAb- | ||||||
| Masarone M, BMC Gastroenterol.2014 [6] | Southern Italy | Retrospective | ALT/AST derangement (at least 2x upper normal values) with HBsAg and HBV-DNA detectable in the serum (>2000 UI/mL) | 460 | 10 | 10/86 | 0/364 | 0/30 | 10/56 |
| Elkady A, World J Gastroenterol.2013 [7] | Egypt | Prospective | HBsAg status reversion and/or HBV DNA detectable | 26 | 1 | 1/8 | 0/17 | ||
| Hsu CHepatology 2013 [8] | Taiwan | Prospective | HBV DNA>10-fold baseline level | 150 | 6 | 17 / 133 | 0 / 0 | 9 /107 | 8/26 |
| Matsui T, J Med Virol.2013 [9] | Japan | Prospective | HBV DNA detectable | 96 | 4 | 4/49 | 0/43 | 1/35 | 3/14 |
| Kim SJEur J Cancer.2013 [10] | Sud Est Asia | Retrospective | HBsAg status reversion | 178 | 17 | 17/161 | 0/0 | 10/120 | 6/27 |
| Kim SJEur J Cancer.2013 [10] | Sud Est Asia | Retrospective | HBsAg status reversion | ||||||
| Kim SJEur J Cancer.2013 [10] | Sud Est Asia | Prospective | HBsAg status reversion | 83 | 2 | 2/83 | 0/0 | 1/57 | 1/24 |
| Koo YX Ann Hematol.2011 [11] | Singapore | Retrospective | HBsAg status reversion with HBV DNA >baseline | 62 | 2 | 2/60 | 0/0 | 0/33 | 2/11 |
| Matsue, Cancer 2010 [12] | Japan | Retrospective | HBsAg status reversion with or without HBV DNA >2.6 log copies/ml | 230 | 5 | 5/56 | 0/174 | 1/37 | 4/19 |
| JiEur J Haematol 2010 [13] | China | Retrospective | HBV DNA>10-fold baseline level or HBV | 369 | 1 | 1/88 | 0/281 | 0/65 | 1/23 |
| DNA>10E5 copies | |||||||||
| FukuschimaAnn Oncol 2009 [14] | Japan | Retrospective | HBV DNA>2.6 log copies/ml or HBsAg status reversion | 127 | 2 | 2/46 | 0/79 | ||
| FukuschimaAnn Oncol 2009 [14] | Japan | Prospective | HBV DNA>2.6 log copies/ml or HBsAg status reversion | 24 | 1 | ||||
| Yeo J Clin Oncol 2009 [15] | China | Retrospective | HBsAg status reversion with Increase in HBV DNA level | 80 | 5 | 5/46 | 0/34 | ||
| Hui Gastroenterology 2006 [16] | China | Prospective | HBsAg status reversion HBV DNA>10E5 copies /mL | 244 | 8 | 7/152 | 1/92 | 3/121 | 4/31 |
Table 5: Characteristics of included studies.
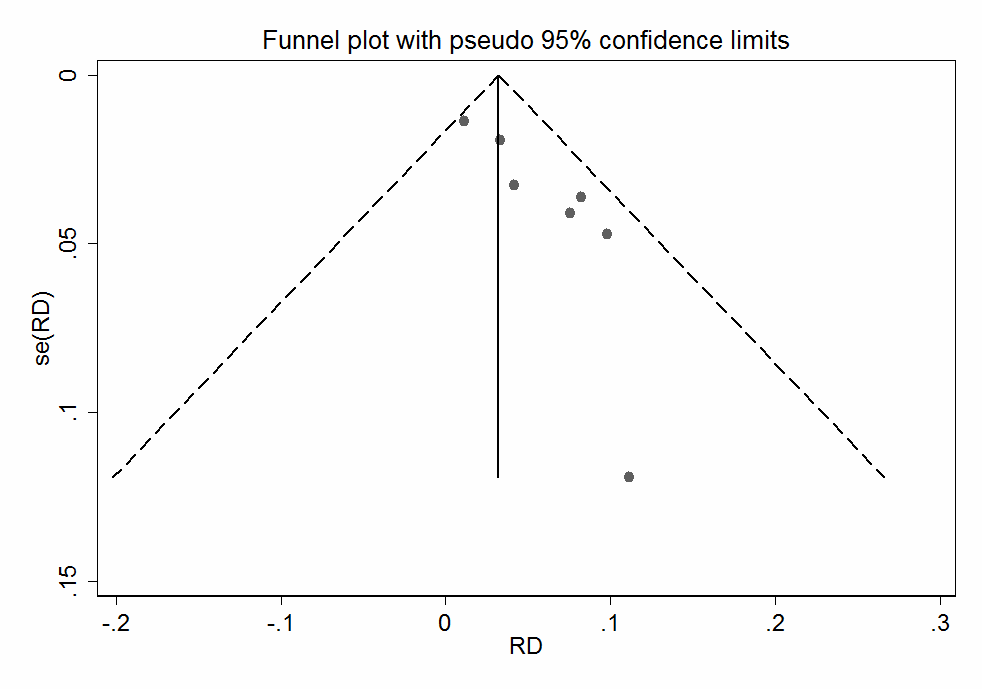
and anti-HBc – patients, comparing risk difference (RD) versus the standard error of RD.
Fiore M. Is Anti-HBs a Useful, Economic and Neglected Tool in the Hands of Hepatologist? A meta-analysis of Observational Studies of HBv Past Infection Reactivation in Patients with Lymphoma. Gastroenterol Hepatol Int J 2016, 1(2): 000108.
Copyright© Fiore M.
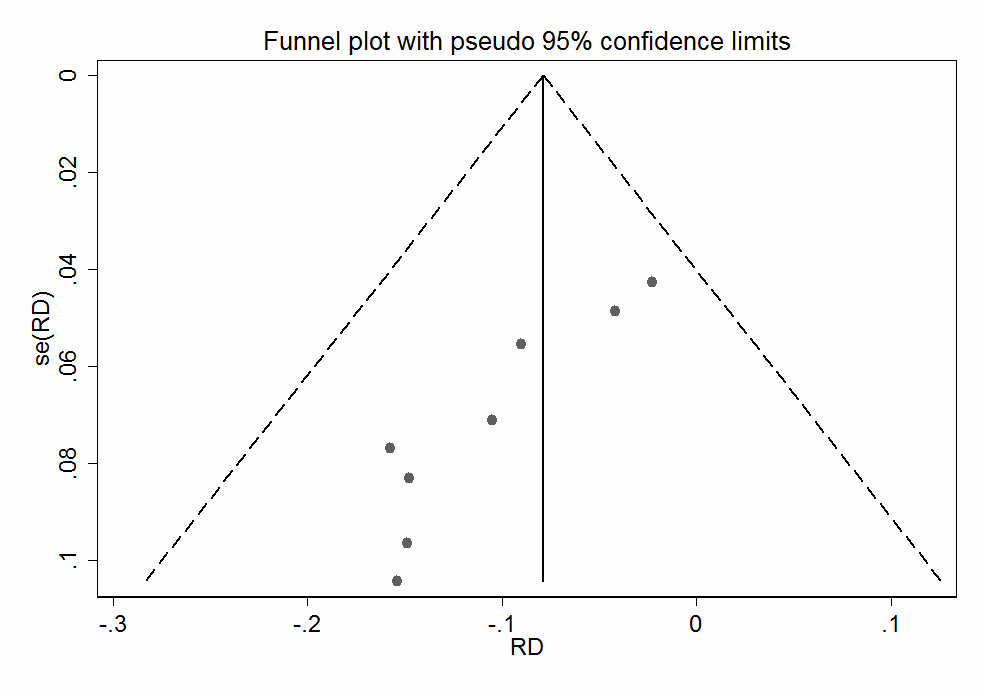
Figure 5: Funnel plot of studies, including anti- HBs + and anti-HBs– patients, comparing Risk Difference (RD) versus the standard error of RD. Discussion This review, carried out on the viable literature, suggests that the presence of antiHBs is a protective factor associated to the risk of HBV reactivation in HBsAg negative patients with lymphoma who undergo immunosuppressant. This seems supported by findings of a recent RCT on the use of prophylaxis [18], where antiHBs negative patients apparently benefit more of the intervention as compared to antiHBs positives (21% vs 13% of reactivations). This opens the question of whether this is the target group. Limitations of our analysis should be noted. First, there is no unambiguous definition of reactivation: we have adopted the definition provided by the authors. Secondly Lastly, only the data of studies published in English language were analyzed so this is another potential bias introduced. So given these limitation, what we have found in this meta-analysis should be interpreted with caution.
Conclusion
In conclusion, based on scientific literature, antiHBs status in HBsAg negative/anti HBc positive patients undergoing chemotherapy may reduce the risk for HBV reactivation and HBV-associated morbidity and mortality. Thus, antiHBs status should be included in a management algorithm for patients with past HBV infection prior to starting immunosuppressive therapy (Table 3).
Fiore M. Is Anti-HBs a Useful, Economic and Neglected Tool in the Hands of Hepatologist? A meta-analysis of Observational Studies of HBv Past Infection Reactivation in Patients with Lymphoma. Gastroenterol Hepatol Int J 2016, 1(2): 000108.
| Reactivation RiskHbsAg - anti HBc + anti HBc + HBV DNA - patients | Hight | anti HBs - | Prophila xis | |
| Reactivation RiskHbsAg - anti HBc + anti HBc + HBV DNA - patients | Hight | anti HBs + | Prophila xis | Prophila xis |
| Reactivation RiskHbsAg - anti HBc + anti HBc + HBV DNA - patients | Moderate | anti HBs - | Prophila xis | Prophila xis |
| Reactivation RiskHbsAg - anti HBc + anti HBc + HBV DNA - patients | Moderate | anti HBs + | Prophila xis | No Prophila xis |
| Reactivation RiskHbsAg - anti HBc + anti HBc + HBV DNA - patients | Low | anti HBs - | No Prophila xis | No Prophila xis |
| anti HBs + | Low | |||
|---|---|---|---|---|
Table 6: A management algorithm for patients with
Acknowledgement
The author thanks Dr. Takeshi Matsui for his personal data.
References
-
Artz AS, Somerfield MR, Feld JJ, Giusti AF, Kramer BS, et al. (2010) American Society of Clinical Oncology provisional clinical opinion: chronic hepatitis B virus infection screening in patients receiving cytotoxic chemotherapy for treatment of malignant diseases. J Clin Oncol 28(19): 3199-3202.
-
Lok AS, McMahon BJ (2009) Chronic hepatitis B: update Hepatology 50(3): 661-662.
-
EASL clinical practice guidelines: (2012) Management of chronic hepatitis B virus infection, J Hepatol 57(1): 167-185.
-
Hwang JP, Lok AS (2014) Management of patients with hepatitis B who require immunosuppressive therapy. Nat Rev Gastroenterol Hepatol Nov 19 [Epub ahead of print] (2013) 11(4): 209-19.
-
Masarone M, BMC Gastroenterol. 2014
-
Elkady A, Aboulfotuh S, Ali EM, Sayed D, Abdel- Aziz NM, et al. (2013) Incidence and characteristics of HBV reactivation in hematological malignant patients in south Egypt. World J Gastroenterol 19(37): 6214- 6220.
-
Hsu C, Tsou HH, Lin SJ, Wang MC, Yao M, et al. (2013) Taiwan Cooperative Oncology Group. Chemotherapy-induced hepatitis B reactivation in lymphoma patients with resolved HBV infection: A prospective study. Hepatology 59(6): 2092-2100. Copyright© Fiore M.
-
Matsui T, Kang JH, Nojima M, Tomonari A, Aoki H, et al. (2013) Reactivation of hepatitis B virus in patients with undetectable HBsAg undergoing chemotherapy for malignant lymphoma or multiple myeloma. J Med Virol 85(11): 1900-1906.
-
Kim SJ, Hsu C, Song YQ, Tay K, Hong XN, et al. (2013) Hepatitis B virus reactivation in B-cell lymphoma patients treated with rituximab: Analysis from the Asia Lymphoma Study Group Eur J Cancer. 49(16): 3486-3496.
-
Koo YX, Tay M, Teh YE, Teng D, Tan DS, et al. (2011) Risk of hepatitis B virus (HBV) reactivation in hepatitis B surface antigen negative/hepatitis B core antibody positive patients receiving rituximab-containing combination chemotherapy without routine antiviral prophylaxis. Ann Hematol 90(10): 1219-1223.
-
Matsue K, Kimura S, Takanashi Y, Iwama K, Fujiwara H, et al. (2010) Reactivation of hepatitis B virus after rituximab-containing treatment in patients with CD20-positive B-cell lymphoma. Cancer 116(20): 4769-4776.
-
Ji D, Cao J, Hong X, Li J, Wang J, et al. (2010) Low incidence of hepatitis B virus reactivation during chemotherapy among diffuse large B- cell lymphomapatients who are HbsAg- negative/ HBcAb-positive: a multicenter retrospective study. Eur J Haematol 85(3): 243- 250. Fiore M. Is Anti-HBs a Useful, Economic and Neglected Tool in the Hands of Hepatologist? A meta-analysis of Observational Studies of HBv Past Infection Reactivation in Patients with Lymphoma. Gastroenterol Hepatol Int J 2016, 1(2): 000108.
-
Fukushima N, Mizuta T, Tanaka M, Yokoo M, Ide M, et al. (2009) Retrospective and prospective studies of hepatitis B virus reactivation in malignant lymphoma with occult HBV carrier. Ann Oncol 20(12): 2013-2017.
-
Yeo W, Chan TC, Leung NW, Lam WY, Mo FK, et al. (2009) Hepatitis B virus reactivation in lymphoma patients with prior resolved hepatitis B undergoing anticancer therapy with or without rituximab. J Clin Oncol 27(4): 605- 611.
-
Hui CK, Cheung WW, Zhang HY, Au WY, Yueng YH, et al. (2006) Kinetics and risk of de novo hepatitis B infection in HBsAg-negative patients undergoing cytotoxic chemotherapy Gastroenterology 131(1): 59-63.
-
Duval S, Tweedie R (2000) Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 56(2): 455-463.
-
Huang YH, Hsiao LT, Hong YC, Chiou TJ, Yu YB, et al. (2013) Randomized controlled trial of entecavir prophylaxis for rituximab-associated hepatitis B virus reactivation in patients with lymphoma and resolved hepatitis B. J Clin Oncol 31(22): 2765-2772. Copyright© Fiore M.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient