Persistent Diarrhea in Childhood: Issues and Concerns
Objective: The comprehensive review is prompted by a scarcity of consolidated information, about persistent diarrhea that is a matter of concern for all involved in child health. Resource and Design: Systematic review of literature augmented with author’s own experience spread over 3 decades. Salient Features: Persistent diarrhea, usually implying persistence of acute diarrhea beyond 2 weeks in an infant or a toddler, is accompanied by failure to thrive or even weight loss, malnutrition, anorexia and superimposed infection(s). Unlike chronic diarrhea, significant malabsorption is not a major issue. Such risk factors as age < 6 months, poor nutritional status, artificial feeding, infection(s), etc predispose to it. Management is primarily through dietary manipulation plus supportive measures. Indications of antimicrobial therapy include identifiable pathogens such as Shigella or E. coli, bloody stools, evidence of systemic infection like sepsis or bacterial overgrowth syndrome and accompanying severe malnutrition. Prognosis is poor if it is undertreated or left untreated with considerable mobidity and mortality. Prompt appropriate therapy leads to good outcome, provided that post-discharge monitoring of nutritional status is continued. Conclusion: Persistent diarrhea in infants and children is better prevented than treated. Attention to risk factors and stress on breast feeding are important constituent of prevention. The mainstay of treatment is dietary manipulation which in severe cases may be in the form of egg-based or chicken-based diet. Poorly treated surviving cases end up with malnutrition and growth failure.
Introduction
Diarrheal disease continues to be among the major causes of morbidity and mortality in children of the resource-limited regions [1, 2, 3, 4, 5]. It is the second leading cause of death in children under five years old, killing around 3 - 5 million infants and young children every year [1].
As a consequence of considerable attention to acute diarrhea, especially use of ORS, morbidity and mortality from this condition has considerable come down. That, however, cannot be said about acute diarrhea persisting beyond 2 weeks, the so-called “persistent diarrhea” [6, 7, 8, 9, 10, 11]. Generally speaking 90% cases are seen < 12 months; majority of them are < 6 months, a large proportion of them succumbing to persistent diarrhea with accompanying malnutrition (both preexisting and consequential) [12]. The survivors usually suffer from a continuum of failure to thrive, nutritional deficiencies and chronic ill health. Though persistent diarrhea accounts for only 10 % of diarrheal episodes, it is responsible for 35 % of deaths from diarrhea in the under 5s. This update, prompted by a scarcity of consolidated information, aims at a comprehensive review of the scattered details about persistent diarrhea that is a matter of concern for all involved in child health.
Definition
Currently, the term, persistent diarrhea, is employed when an episode of acute diarrhea/gastroenteritis (>3loose, liquid motions/24 hr) continues beyond 2 weeks period. According to conservative estimates, some 7 to 25% children in preschool age group who suffer from acute diarrhea/ gastroenteritis may end up with persistent diarrhea in the resource-limited countries such as ours. This replaces the earlier cut-of line of at least 7 days’ diarrhea proposed by Halliday in 1989 to define persistent diarrhea. True, both, chronic diarrhea and persistent diarrhea have minimal cut-off duration of 14 days along with some overlap. Nevertheless, a few differences are noteworthy (Table 1).
| Persistent Diarrhea | Chronic Diarrhea | |
|---|---|---|
| Onset | As an acute episode of infectious diarrhea /gastroenteritis that goes on and on | Insidious; usually secondary to a major malabsorptive state such as celiac disease, cystic fibrosis or endemic tropical sprue |
| Age | Usually around 1 year; invariably < 2 year | No age is a bar |
| Diarrheal dehydration | Frequent | Infrequent |
| Associated malnutrition | Considerable with wasting | Less pronounced; more often growth retardation with stunting |
Table 1: Differences between persistent and chronic diarrhea.
Epidemiology
Peak incidence is around 1 year of age. It contributes considerably to malnutrition. In subjects under 1 year, mortality is particularly high. When persistent diarrhea has its onset before the age of 3
- Age between 6 months to 1 year; after 2 years of age, risk of persistent diarrhea is reduced.
- Low birthweight
- Malnutrition; nutritional deficiency states, especially zinc and vitamin A deficiency.
- Diarrheal episode with blood and mucus such as caused by enteropathogenic or aggregative adherent E. coli, Shigella, Salmonella, Campylobacter jejuni, and rotavirus, especially in infants less than 3 months of age.
- Excessive fluid intake, especially carbonated drinks and fruit juices.
- Artificial feeding.
- Indiscriminate use of ORS, especially with high sugar content.
- Lactose intolerance.
- Systemic infections like septicemia.
- Cow milk protein allergy.
- A preceding diarrheal episode in the recent past may make the child vulnerable to yet another episode that months, it is often termed intractable diarrhea of infancy.
Etiology: Risk Factors
Persistent diarrhea is as yet an entity of obscure etiology. Identifiable risk factors are listed in Table 2.
becomes persistent. The factors that contribute to persistent diarrhea in such a situation include deterioration in nutritional status, damage to small intestinal mucosa, contamination of animal milk and osmotic diarrhea.
- Intestinal parasitosis
- Autoimmune enteropathy
- Chloride diarrhea
- Acrodermatitis enteropathica.
- A comparative listing of risk factors in persistent diarrhea in our own study in India [6] and a study from South Africa is presented in [Table 3].
- Gupte and Pal ( Jammu and
- Kashmir; percentage out of 120
- Risk factor studied cases) [4] of 100 studied cases) [5,13]
- Age: 6 month-12 month
- 72%
- 91%
- 12 month
- 28%
- 7%
- Undertreated/ maltreated/untreated gastroenteritis
- 40%
- 34%
- LBW
- 32%
- 26%
- PEM/nutritional deficiency states
- 90%
- 85%
- Artificial feeding
- 60%
- 52%
- Excessive fluid intake, fruit juice or carbonated drinks
- 22%
- 45%
- ORS indiscriminate use
- 25%
- Not considered
- Lactose intolerance
- 50%
- 55%
- Persistent intestinal infection
- 30%
- 58%
- Systemic infection (sepsis)
- 17%
- 24%
- Cow’s milk-protein (CMP) allergy
- 15%
- 22%
- Protozoal/helminthic infestation
- 30%
- 20%
- Acrodermatitis enteropathics
- 3%
- Nil
- Miscelaneous: autoimmune enteropathy, chloride diarrhea, glucose-galactose
- Nil
- 1% malabsorption
Table 2: Relative incidence of risk factors in an Indian study and a South African study.
Note: In a majority of the cases, more than one factor was present in both series.
Clinical Profile
Two major clinical types are recognized:
- Mild-moderate PD: Subjects with several motions/day but without any adverse fallout on nutritional status and growth and development.
- Severe PD • Subjects with several motions (but without dehydration), and malnutrition and growth retardation • Subjects with several motions and dehydration that is difficult to control with ORS.
In the subjects belonging to the second category, manifestations include progressive weight loss, malnutrition, anorexia, malabsorption and secondary infections.
Diagnosis
Diagnosis is by and large clinical with support from screening laboratory tests. The latter must include • Meticulous stool microscopy, on at least 3 (preferably
6) successive or alternate days for ova and cysts. • A stool culture, if warranted.
Furthermore, additional investigations are dictated by the merit of the individual case (Table 4).
| Clinical Clue | Test |
| Acidic diarrheal stool | Demonstration of reducing substances in stools |
| Highly fatty stool | Fat balance studies/steatocrit test |
| Coexisting recurrent chest infection | Sweat chloride estimation |
| Coexisting skin lesions | Serum zinc estimation |
Table 3: Relative incidence of risk factors in an Indian study and a South African study.
Management
While treating persistent diarrhea, age (whether under 6 months age or beyond) and severity with regard to coexisting dehydration and malnutrition are borne in mind. The central to all therapeutic measures is dietary manipulation and therapy of coexisting deficiency states and dehydration and electrolyte imbalance, if present.
Dietary Manipulation
Dietary manipulation along with rehydration therapy forms the crux of the management of persistent diarrhea. Breastfeeding must continue. Admittedly, diarrhea may persist despite breastfeeding. However, infant’s nutrition remains maintained. In fact, he may even gain some weight [14, 15, 16]. Diet A: In case persistent diarrhea is mild, the infant on artificial feed (Table 5) should be given milk mixed with a cereal or curd rather than milk as such.
| Quantity (g) | |
|---|---|
| Puffed rice | 12.5 |
| Milk | 40 |
| Sugar | 2.25 |
| Oil | 2 |
| Water | To make 100.0 |
| Egg white | 96 Kcal/100g |
| Protein | 10.00% |
| Carbohydrate | 55.87% |
| Lactose | 1.73% |
| Fat | 33.90% |
| Amino acid score | 1.00% |
Table 5: Clinical clues for special investigation.
Diet B: In case persistent diarrhea is severe, as manifested by dehydration, high purge rate (over 7 mg/kg/hour) or very frequent large and watery stools, total milk elimination in an artificially fed infant is needed. The composition of a recommended milk-free, egg-based diet is given in (Table 6).
| Food Ingredient | Quantity (g) | |
|---|---|---|
| Highly fatty stool | Fat balance studies/steatocrit test | |
| Coexisting recurrent chest infection | Sweat chloride estimation | |
| Coexisting skin lesions | Serum zinc estimation |
Table 4: Egg-based diet for moderately severe persistent diarrhea.
Table 6: Egg-based diet for moderately severe persistent diarrhea. Note: Egg white is added to the mixture of weighed rice, sugar and oil. Boiled water is added to make a thick gruel weighing 100 g. Breastfeeding, reduced intake of other milk, or its total withdrawal should be supplemented with enriched gruels like khichri with oil, lentil with oil, mashed potato with oil, curd mixed with mashed potatoes or banana or rice with added sugar Diet C: In cases of severe persistent diarrhea that fails to respond to the dietary management outlined above, intolerance to disaccharides (other than lactose as well) becomes quite likely. Mono or oligosaccharide carbo- hydrates diet is well tolerated by these children. Chicken- based diet for such a persistent diarrhea is appropriate. It is advisable to provide maintenance requirements of vitamins, and trace elements like iron, folate and zinc to infants and children with persistent diarrhea on dietary manipulation. During convalescence, most cases need relatively higher intakes for the catch-up growth (Table 7).
| Food ingredient | Quantity/liter | Kcal (%) | Protein (g%) |
|---|---|---|---|
| $Chicken^{1}$ | $100g | 110 | 26 |
| Glucose^{2}$ | $20-40g | 160 | - |
| Coconut oil^{3}$ | $40-50g | 450 | - |
| KCl (15%) | 7.5ml | - | - |
| NaHCO_{3 (7.5%) | 20-30ml | - | - |
| Total | 1,000ml | 720 | 26 |
Table 6: Chicken-based (monosacharide-based) for severe persistent diarrhea with likelihood of lactose and other disaccharide int
Table 7: Chicken-based (monosacharide-based) for severe persistent diarrhea with likelihood of lactose and other disaccharide intolerance diet. Note:
- it is prepared by grinding the precooked boneless chicken stuff in a mixie. Glucose, oil and some water are added to it and the feed is brought to a boil. Additional water is added to make a final volume of 1 liter. Finally, KCl and NaHCO3 are added. To safeguard against spoilage, it is stored in a refrigerator.
- Glucose is initially added in 2% concentration and then built up to 4% by increasing 1% every alternate day. To reduce osmotic load, a mixture of glucose and sugar may be employed.
- Any vegetable oil may be employed in place of coconut oil Box 1: presents the stepwise dietary manipulation in persistent diarrhea & Stepwise dietary manipulation.
Step 1: Diet A - Reduced Lactose Diet - Milk plus cereals (wheat, rice, khichri) - Milk plus mashed banana - Milk plus soyamilk - Around 70% cases are likely to respond to this treatment with control of diarrhea & maintenance of nutrition & hydration. - The remaining 30% need to be shifted to Step 2 comprising lactose-free diet. Step 2: Diet B - Lactose-free Diet Total elimination of animal milk Energy from cereals Protein from chicken-based or egg-based diet Or Soya milk ( 40% protein) Or Proprietary protein hydoxylate Other 15-20% patients respond to it. If 1-week trial fails to stop diarrhea, shift to Step 3 comprising withdrawal of all starch (disachiradases) . Then, what should be given? Step 3: Diet C - Monosaccharide-based Diet ( No starch diet) Glucose plus egg white -based and/or chicken- based diet. Almost all remaining 10-15% patients are likely to respond to it. If an occasional patient fails to do so, a diagnosis of “glucose malabsorption” is most likely. Such a patient responds to IV glucose.
Parenteral Nutrition
Finally, an occasional case may turn out to be refractory to the aforesaid therapy. Such a case may have a ver high frequency of motions, very high volume motions, intolerance of oral feeds, or - Continuous weight loss. Parenteral nutrition (partial or total) is indicated in such cases.
Micronutrient Supplements
Zinc 10-20 mg/day for at least 2 weeks Vitamin A supplements. A single large dose, 50-200 IU depending on age. 2 lakh IU - > 1 year Children weighing < 8 kg regardless of age: only 1 lakh IU 1 lakh IU – 6 m -1 yr. Multivitamin supplements Mag sulfate IM Potassium PO Folic acid 1 mg/day for 2 wks Iron only after diarrhea is controlled. Elemental copper Drug Therapy Antimicrobial therapy is indicated
- in the presence of identifiable enteric pathogens such as Shigella or E. coli,
- when persistent diarrhea is bloody but culture facilities are not available, or
- When there is evidence of persistent diarrhea being secondary to a systemic infection like septicemia. Parenteral ampicillin plus an aminoglycoside combination is appropriate in most cases. In the so-called “bacterial overgrowth syndrome”, a combination of oral gentamicin (50 mg/kg/day 4 hourly for 3 days) and oral cholestyramine (lg 6 hourly for 5 days) may prove useful. Metronidazole is recommended only for amebiasis, giardiasis, or anaerobic infections. Probiotics are of doubtful value. As yet, only a few studies have been conducted on role of probiotics in persistent diarrhea There is limited evidence that probiotics may decrease the frequency, volume and consistency of stools along with cutting short the hospital stay. All in all, convincing evidence is not yet available about utility of probiotics in persistent diarrhea. Antimotility drugs, kaolin and pectin are best left out.
Box 2: Lists some of the signals of good response. Signals indicating good response to treatment in persistent diarrhea Improvement in frequency and volume of motions Discharge Criteria Successfully management of persistent diarrhea following dietary manipulation plus additional measures should be followed by discharge from the hospital provided that severe malnutrition is not present. A good follow-up is a must to ensure that the child e consumes normal diet appropriate for age. Rationally speaking dietary intake need to more than the average for age to make up for the weight deficit that may have occurred during the course of the disease and/or on top of the preexisting malnutrition [6, 13]. As already emphasized, malnutrition per se is an important risk factor for development of persistent diarrhea.
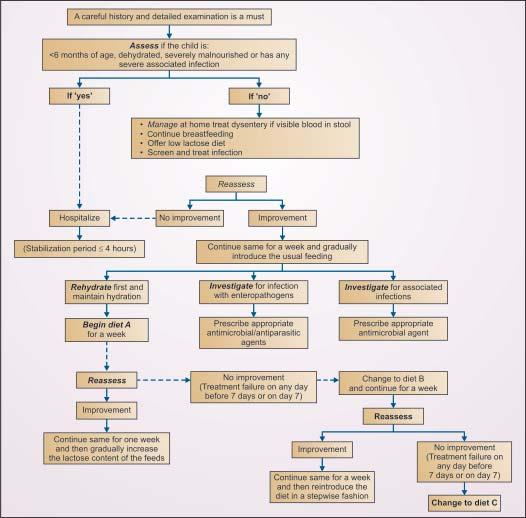
Algorithmic Approach
An algorithmic approach to management of persistent diarrhea is given in the Flow chart (Figure 1).
Prognosis and Outcome
Prognosis is usually good following timely institution of proper therapy (correction of dehydration, antimicrobial agents for infection) with dietary manipulation though monitoring of dietary intake is needed postdischarge as well. Under- treated or untreated persistent diarrhea causes high degree of morbidity and mortality, particularly in infants. Determinants of poor outcome include
- Early months of life, especially age <3 months when dietary manipulation is tough.
- Poor nutritional status
- Severe watery diarrhea
- Moderate to severe dehydration with dyselectrolytemia refractory to correction
- Systemic infections (e.g. sepsis)
- Severe lactose and/or monosaccharide intolerance. Survivors are usually left with moderate to gross malnutrition which may per say contribute to morbidity and mortality.
Prevention
Box 3 lists some the important preventive measures. Preventive measure against persistent diarrhea
- Promotion of breastfeeding and safe weaning (complementary feeding) practices to ensure good diarrhea.
- Avoidance of indiscriminate use of ORS, carbonated drinks and antimicrobial therapy Experience has shown that, persistent diarrhea is virtually absent in infants and toddlers in whom the stated preventive measures are in place [6, 7].
TAKE HOME MESSAGES
- Persistent diarrhea, usually implying persistence of acute diarrhea beyond 2 weeks in an infant or a toddler, is accompanied by failure to thrive or even weight loss, malnutrition, anorexia and superimposed infection(s).
- Such risk factors as poor nutritional status, artificial feeding, infection(s), etc. predispose to it.
- Management is primarily through dietary manipulation plus supportive measures.
- Indications of antimicrobial therapy include identifiable pathogens such as Shigella or E. coli, bloody stools , evidence of systemic infection like sepsis or bacterial overgrowth syndrome and accompanying severe malnutrition.
- Prognosis is poor if it is undertreated or left untreated with considerable mobidity and mortality. Prompt appropriate therapy leads to good outcome, provided that postdischarge monitoring of nutritional status is continued.
- Preventive measures include promotion of breast feeding and safe weaning practices, attention to overall nutrition and prompt treatment of an acute episode of diarrhea with rehydration therapy and administration of zinc for 2 weeks.
Acknowledgment
Thanks are due to the Management and Administration of Mamata Medical College for permission to publish this original review article.
Acknowledgement is also made to the help received from Dr. Gagan Hans, Assistant Professor, NDMC Medical College/Hindu Rao Hospital, New Delhi, India, in preparing the manuscript.
References
-
World Health Organization. Diarrheal disease.
-
Patwari AK, Gupte S, Anderson RA (2016) Pediatric gastroenterology. In: Gupte S (ed): The Short Textbook of Pediatrics, (12th edn.) India: Jaypee 441-480.
-
Medline Plus . Diarrhea: Overview.
-
Gupte S, Pal M (2001) Experience with persistent diarrhea. Eur Bull Pediatr Gastroenterol Nutr 4: 137-142.
-
Hensen AG, Dick P (2011) Persistent diarrhea: Clinical observations. Proceedings, International Symposium on Diarrheal Diseases, Johannesburg Abstract No A-13.
-
Gupte S, Gupte N, Anderson L, Anderson RA (2013) Diarrheal diseases. In: Gupte S, Gupte SB, Gupte M (eds): Recent Advances in Pediatrics (Special Vol 23: Pediatric Gastroenerology, Hepatology and Nutritioin. India: Jaypee 57-81.
-
Gupte S (2016) Persistent diarrhea Keynote address: International Conference of Pediatric Gastroenterology, Hepatology, Transplant and Nutrition, Jaipur 2016.
-
Moore SR. Persistent diarrheain resource-limited countries.
-
Matthai J, Raju B, Bavdekar (2011) A Chronic and persistent diarrhea in infants and young children: Status statement (Pediatric Gastroentereology Chapter, Indian Academy of Pediatrics) Indian Pediatr 48(1): 37-42.
-
Gopalan S (2008) Persistent diarrhea. In: Bavdekar A, Matthai J, Sathiyasekaran M, Yaccha (eds): IAP Speciality Series on Pediatric Gastroenterology. New Delhi: Jaypee.
-
Gupte S, Anderson RA, Gupte N. (2007) Pertsistent diarrhea. Pediatrics Today 11: 23-28.
-
Patwari AK, Sahani (2011) A. Persistent diarrhea. In: Gupte S (ed): Recent Advances in Pediatrics (Special Vol6: Gastroenterology, Hepatology and Nutrition. New Delhi: Jaypee 110-129.
-
Bhutta ZA, Molla AM (1992) Nutritional management of persistent diarrhea: Factors predicting clinical outcome. Acta Pediatr 381 (suppl): 144-148.
-
Bhutta ZA, Bebricks KM (1996) Nutritional management of persistent diarrhea of childhood: A persepective from the developing world. J Pediatr Gastroenterol Nutr 22(1): 17-22.
-
Bhutta ZA, Ghishan F, Lindley K, Memon IA, Mittal S, et al. (2004) Persistent and chronic diarrhea and malabsorption. Working Group report of the second World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition./Commonwealth Association of Pediatric Gastroenterology and Nutrition J Pediatr Gastroenterol Nutr 39 (Suppl 2): S711.
-
Bhutta ZA, Nelson EA, Lee WS, Tarr PI, Zablah R, et al. (2008) Persistent Diarrhea Working Group. Recent advances and evidence gaps in persistent diarrhea. J Pediatr Gastroenterol Nutr 47(2): 260- 265.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient