Gastrointestinal Angiodysplasia: Report of Two Cases in Pediatrics
Intestinal angiodysplasia is a vascular abnormality where blood vessels are ectatic, tortuous with minimal muscle lining, being able to affect any segment of the gastrointestinal tract, showing single or multiple lesions at different sites, with the left hemicolon the most frequent location in children. The pathophysiological mechanism that originates it is still unknown, as is the epidemiology of this condition. The spectrum of clinical manifestations is wide, being able to debut and recur at any time in life with hemorrhage of varying intensity. Endoscopic and radiological tools are used for diagnosis. Treatment options include pharmacological, endoscopic therapies and surgical resection. In this article we describe two pediatric cases (6 months and 7 years respectively) which presented with recurrent gastrointestinal bleeding in need of transfusion therapy, in whom it was not possible to identify the origin of the disease until later, with adequate control of symptoms. After definitive treatment, which in one of them was total gastrectomy.
Introduction
Gastrointestinal bleeding (GIB) is considered a frequent condition in the pediatric population, being able to affect any segment of the digestive tract and manifest itself in different ways. An approximate incidence of 6.4% has been reported and the causes to be taken into account differ according to the patient's age [1]. Intestinal angiodysplasia is a vascular abnormality of unclear cause, not associated with skin lesions, systemic vascular disease or family syndrome, since it is not a common etiology of GIB, it is a diagnostic challenge and its prevalence and incidence in the child population are unknown to date [2]. The purpose of this publication is to present two cases of secondary gastrointestinal bleeding to gastrointestinal angiodysplasia managed in a pediatric referral hospital and review the literature.
Case 1
A 6-month-old boy with a history of arthrogryposis who has had episodes of hematemesis of postprandial predominance with secondary anemia since one month of life. He was evaluated by a Pediatric Gastroenterologist who performed upper digestive endoscopy which was normal, with no evidence of signs of old or recent bleeding (Figure 1). Initially eosinophilic gastropathy was suspected, he was discharged with breastfeeding with a dairy-free diet to the mother.
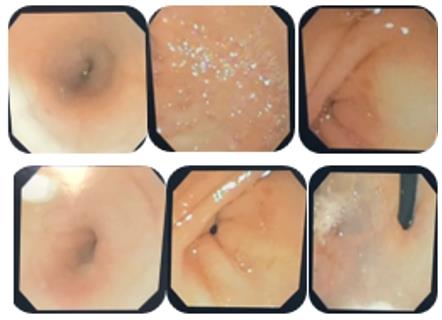
He remained asymptomatic for 2 weeks. After this time, he reentered with hematemesis, melena and anemia. New endoscopy and diagnostic laparoscopy were scheduled in search of intestinal duplication, which was normal. On endoscopy (Figure 2), a clot adhered to fundus was observed, which was removed with washing, leaving bleeding that subsequently gave way spontaneously.
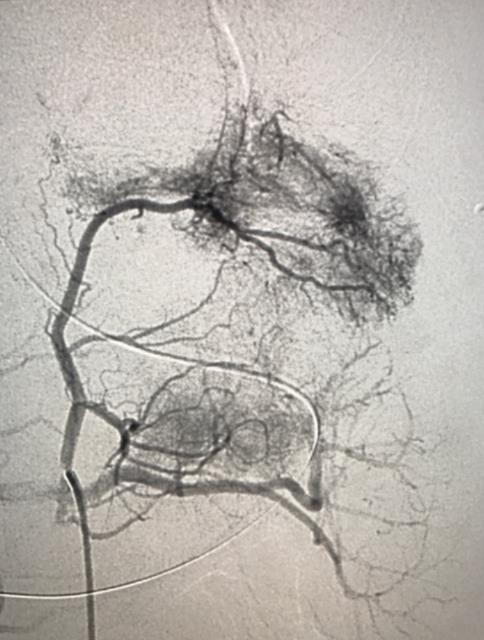
Abdominal vessel arteriography reported multiple aberrant branches of the left gastric artery (Figure 3). They were embolized twice by interventional radiology.
The patient persisted with melenas, requiring transfusions with red blood cells every 48 hours. It was considered to perform a new digestive endoscopy evidencing flat ulcerated lesion with signs of recent bleeding in the subcardial region on the minor curvature and mucosa of the gastric body with easy bleeding on contact with the equipment, producing linear erosions. Endoscopic therapy with argon plasma was performed.
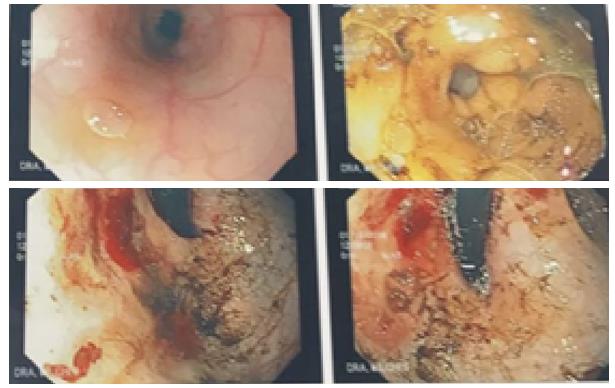
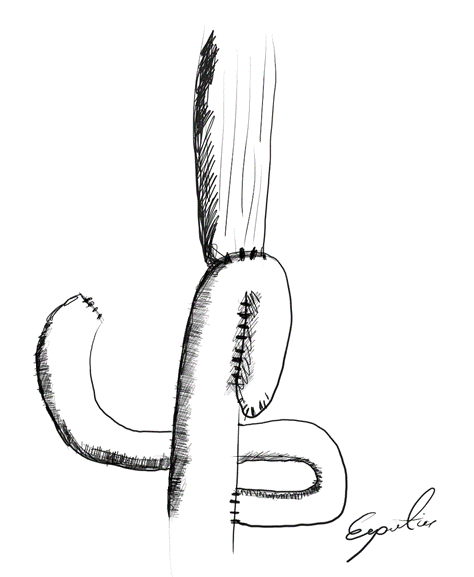
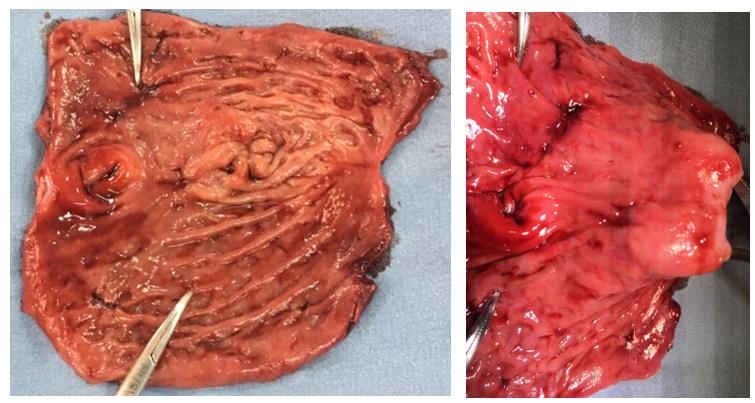
Anemization persisted, hypotension and continuous transfusion requirement, it was decided jointly with pediatric surgery to perform total gastrectomy and Roux Y esophagojejunostomy (Figure 4). In a surgical piece, multifocal lesions with bleeding stigmas were observed (Figure 5). The histopathological study reported stomach with transmural vascular congestion and multiple lesions compatible with angiodysplasia, without suggestive findings of metaplasia, dysplasia or malignancy. Currently without recurrence of bleeding, without anemia, feeding orally with special nutritional plan, supplementation with vitamin B12 and folic acid.
Case 2
A 7-year-old girl with a history of intermittent rectorrhage since age of 4. On 2 occasions she required transfusion of red blood cells (RBC) due to anemia with hemodynamic compromise. A total colonoscopy was performed, showing proctitis in the middle and distal third of the petechial aspect and rectal hemangioma (Figure 6) as well as contrasted pelvic resonance that showed diffuse thickening of the rectum wall that started 10 centimeters (cms) from the anal margin with submucosal thickening, corresponding to a nodular vascular lesion greater than 1.5 cms. Together with interventional radiology, it was decided to perform angiography where rectal angiodysplasia (Figure 7) was found fed by the superior hemorrhoidal artery that was embolized with polyvinyl alcohol particles (PVA embolization) with rectorragia resolution. In clinical follow-up two years later, without recurrence of bleeding.


Discussion
GI angiodysplasia can be defined as the finding of abnormal, ectatic, dilated, tortuous and usually small (less than 10 mm) blood vessels visualized between the mucous and submucosal layers of any segment of the gastrointestinal tract. Histologically, the affected vessels are only covered by endothelium with minimal or non- existent smooth muscle [3, 4].
It is considered one of the causes of digestive bleeding, being found more frequently in adults, while in children it is a rare pathology [5]. So far, there are no studies of prevalence in the child population. Cases have been reported in children from the neonatal period to adolescence, with predominance in males and an average age at diagnosis of 7.1 years [5, 6, 7].
Approximately 40-60% of patients with angiodysplasia have more than one lesion, which are usually located in the same part of the GI tract and up to 20% of patients may have synchronous lesions in other sites, which highlights the importance of assessing both the lower and upper GI tract in patients with symptomatic angiodysplasia [3].
The pathophysiology of angiodysplasia in children is not clear, but it is believed that the origin is completely different from that of adults. In the latter, the most accepted pathophysiological theory is partial, intermittent and gradual obstruction (Boley's theory) at the site where the submucosal veins cross the muscular layer causing dilation and tortuosity in the veins, venules and capillaries of the mucosa and submucosa due to increased pressure secondary to repetitive spasmodic contractions [1].
Among the most common clinical manifestations is GI bleeding that can start at any time in life, be recurrent and of varying intensity. In some individuals, these episodes may develop anemic symptoms (94.4% of cases) with transfusion requirements in 61.1% of children, while in others the diagnosis may be incidental; In addition, abdominal pain (55.6%) and hematoquezia / melenas (50%) may occur [5, 8, 9].
In children, the most frequent location is the left hemicolon (rectosigmoid) while in adults it tends to involve the cecum and right colon [9]. Recent evidence shows that up to 10% of patients evaluated by endoscopy, endoscopic capsule and colonoscopy can have angiodysplastic lesions in the small intestine (50%
duodenum, 37% jejunum, 15% ileum) and stomach (50%) [10].
There is no gold standard test for diagnosis. Arteriography and endoscopic studies are considered studies of great value for confirmation. The sensitivity and specificity reports of the latter are 80% and 90% respectively; however, a normal result does not rule out the pathology [5].
Angiotomography is a sensitive and specific study for diagnosis. Junquera, et al. [11] reported a sensitivity, specificity and positive predictive value of 70, 100 and 100% respectively. This makes it an appropriate diagnostic alternative in the study of GI bleeding when with endoscopic studies, the bleeding site is not established, avoiding the use of techniques with higher radiation such as standard angiography [7, 11]. To date there are no data on the diagnostic accuracy of magnetic resonance imaging, which was a useful tool in the diagnosis of one of our patients. On the other hand, angiography is reserved for patients in whom other diagnostic modalities have failed to identify the source of bleeding or in those with severe bleeding and hemodynamic instability [11].
There is no defined treatment protocol and decisions regarding this are made based on previous experience and the information presented in the case reports. Among the treatment modalities are:
Endoscopic therapy (coagulation with argon plasma, application of mechanical clips, multipolar electrocoagulation and laser photoablation), which is considered effective but the rates of recurrence of bleeding are high especially in those located in the small intestine [4].
With respect to electrocoagulation with argon plasma, this has become the most commonly used method with the advantage of being highly specific and the damage of the surrounding tissue to the angiodysplastic lesion is limited. It is considered a safe, easy and cost-effective technique, particularly recommended for lesions of more than 10 mm in the right colon where the intestinal wall is thinner [4].
Superselective transcatheter embolization has proven effective in 80-90% of patients and has the advantage of being able to be used if the bleeding recurs. Complications secondary to this treatment include hematomas, intestinal infarction, arterial dissection, thrombosis and pseudoaneurysms, which occur in up to 9% of patients and the serious being less than 2% [4].
Other treatment options include somatostatin analogs that produce their effect by multiple mechanisms including inhibition of angiogenesis, decreased splanchnic and duodenal blood flow, increased vascular resistance, increased platelet aggregation and decreased mesenteric and portal blood flow. Junquera et al. [11] demonstrated the efficacy of octreotide in preventing recurrence of bleeding (23% vs. 48% placebo) at one year of follow-up of patients [4].
It has been speculated that blocking vascular endothelial growth factor (VEGF) could reduce or prevent the development of these vascular lesions. For this reason, the use of antiangiogenic agents such as thalidomide that blocks their biological expression and therapy such as Bevacizumab (Avastin) has been proposed, which is a humanized recombinant monoclonal antibody that binds to VEGF by inhibiting its action [4, 12, 13]. In a study that included 3 patients with bleeding secondary to angiodysplasia who did not respond to endoscopic therapy, there was an improvement in hemoglobin levels (17.6% increase), decrease in the number of transfusions and in the frequency of hospitalizations during 4.5 months of follow-up: however, this medication can cause severe and even fatal adverse reactions, in addition to being able to cross the placental barrier and induce severe malformations in fetuses [4, 7].
Finally, surgical resection, which is a curative option, is aimed at the areas of angiodysplasia and is reserved for bleeding patients where the other alternatives are not effective as in the case of the first patient [4, 7].
Unlike adults, the need for a total gastrectomy for the management of digestive hemorrhage is rare in children and has been described in some cases of gastric volvulus necrosis. Therefore, there is limited literature on gastric reconstruction in children [14].
Several gastric substitutes have been described in adult patients, mostly using the Roux Y principle. The J- bag from Hunt-Lawrence, which was first described by Hunt. The jejunum is divided between 10 and 15 cm of the Treitz ligament between the third and fourth vascular arches. The distal end is closed and an enteroenteric anastomosis is performed. The pouch is anastomosed to the esophagus to achieve continuity of the GI tract [15, 16, 17].
The creation of a pouch during gastric replacement provides several advantages, such as better food intake, a slower passage of food, less postprandial symptoms, less weight loss and probably a better quality of life in adults undergoing total gastrectomy due to cancer [15]. Despite the lack of controlled studies, it is suggested that physical growth appears to be within normal limits, and the pouch procedure is well tolerated by children in light of other reports [16, 17, 18]. However, due to insufficient or absent intrinsic factor production, vitamin B12 deficiency may develop and, therefore, a monthly replacement for life is required [16, 17, 18].
Conclusions
GI angiodysplasia is a rare cause of gastrointestinal bleeding in children; however, it is important to take it into account in differential diagnoses, especially when the child has recurrent bleeding. This abnormality can simultaneously affect different places of the digestive tract and, although in adults it is considered a pathology secondary to aging, in children its origin is not well clarified. Often there is a delay in its diagnosis and although there is no gold standard test, endoscopic and radiological studies can help us. With respect to the latter, angiotomography and angiography are very sensitive and specific, but they have the disadvantage of exposure to ionizing radiation, which is why angioresonance could be taken into account as a diagnostic alternative. Finally, within the therapeutic options we find endoscopic therapy, transcatheter embolization, surgery and some medications such as somatostatin analogues and thalidomide; However, their choice depends on the patient's clinical status, the availability of the therapies and the experience of the multidisciplinary treatment group. Conflicts of interest: None
References
-
Romano C, Oliva S, Martellossi S, Miele E, Arrigo S, et al. (2017) Pediatric gastrointestinal bleeding: Perspectives from the Italian Society of Pediatric Gastroenterology. World J Gastroenterol 23(8): 1328- 1337.
-
Saudi A, Al-Mehaidib A, Alnassar S, Alshamrani AS (2009) Gastrointestinal angiodysplasia in three Saudi children. Departments of Pediatrics 29(3).
-
Sami SS, Al-Araji SA, Ragunath K (2014) Review article: Gastrointestinal angiodysplasia-pathogenesis, diagnosis and management. Aliment Pharmacol Ther 39(1): 15-34.
-
Jackson CS, Strong R (2017) Gastrointestinal Angiodysplasia: Diagnosis and Management. Gastrointest Endosc Clin N Am 27(1): 51-62.
-
Abdoon H (2010) Angiodysplasia in a child as a cause of lower gi bleeding: Case report and literature review. Oman Med J 25(1): 49-50.
-
Kimpton JA, Bowen JC, Craigie RJ (2012) Paediatric angiodysplasia of the jejunum: A case report and review of the literature. Scott Med J 57(4): 1-3.
-
Chuang FJ, Lin JS, Yeung CY, Chan WT, Jiang C Bin, et al. (2011) Intestinal angiodysplasia: An uncommon cause of gastrointestinal bleeding in children. Pediatr Neonatol 52(4): 214-218.
-
Boyle JT (2008) Gastrointestinal Bleeding in Infants and Children Determining Severity of Gastrointestinal (GI) Bleeding. Pediatr Rev 29: 39-52.
-
De Diego JA, Molina LM, Diez M, Delgado I, Moreno A, et al. (1988) Intestinal angiodysplasia: retrospective study of 18 cases. Hepatogastroenterology 35(5): 255-259.
-
DeBenedet AT, Saini SD, Takami M, Fisher LR (2011) Do clinical characteristics predict the presence of small bowel angioectasias on capsule endoscopy? Dig Dis Sci 56(6): 1776-1781.
-
Junquera F, Quiroga S, Saperas E, Pérez-Lafuente M, Videla S, et al. (2000) Accuracy of helical computed tomographic angiography for the diagnosis of colonic angiodysplasia. Gastroenterology 119(2): 293-299.
-
Bauditz J (2016) Effective treatment of gastrointestinal bleeding with thalidomide-Chances and limitations. World J Gastroenterol 22(11): 3158- 3164.
-
McFarlane M, O’Flynn L, Ventre R, Disney BR (2017) Emerging role of thalidomide in the treatment of gastrointestinal bleeding. Frontline Gastroenterol 9(2): 98-104.
-
Boybeyi Ö, Karnak I, Tanyel FC, Şenocak ME (2009) Management of unusually extensive esophagogastric corrosive injuries: emergency measures and gastric reconstruction. J Pediatr Surg 44(5):1022-1026.
-
CJ H (1952) Construction of food pouch from segment of jejunum as substitute for stomach in total gastrectomy. AMA Arch Surg 64(5): 601-608.
-
Menon P, Sunil I, Chowdhury SK RAO KL (2003) Hunt- Lawrence pouch after total gastrectomy: 4 years follow up. Indian Pediatr 40(3): 249-251.
-
Durham MM, Ricketts RR (1999) Neonatal gastric perforation and necrosis with Hunt-Lawrence Pouch reconstruction. J Pediatr Surg 34(4): 649-651.
-
Schwarz ABH (1998) Gastric substitute after total gastrectomy--clinical relevance for reconstruction techniques. Langenbecks Arch Surg 383(6): 485-491.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient