Gastric Polyps in North India: Prevalence, Pattern and Beyond
Background The prevalence and histopathological type of gastric polyp vary between populations. In the recent past aggressive treatment of Helicobacter pylori (H. pylori) and the excessive use of proton pump inhibitors (PPIs) have altered the prevalence of specific types of gastric polyp. This study was designed to evaluate the prevalence and histopathology of gastric polyps. Methods the medical record of patients who underwent esophagogastroduodenoscopy in 3 centers in Northern India from 2011-2019 were reviewed. Results the prevalence of gastric polyps was 5%, of which 900 (50%) were fundic gland polyps (FGP), 757 (42.05%) hyperplastic polyps (Hpp), and 143 (7.90%) others. 46.49% of the polyp group (cases) and 45.15% of controls had H. pylori gastritis (HPG); 30.59% of the cases and 23.27% of controls had chronic inactive gastropathy (CIG); 1.34% of the cases and 25.63% of controls had reactive gastritis (RG); and 9.05% of the cases and 1.39% of controls had intestinal metaplasia (IM). Portal hypertensive gastropathy (PHTG) was seen in 0.50% of the cases and 4.54% of the controls. Conclusions As a result of anti - H. pylori treatment and the excessive use of PPIs, FGP are now more common, even in Northern India, than Hpp (a new trend). HPG, CIG and IM were more frequent in the cases whereas RG and PHTG were more frequent in the controls. The difference was
Introduction
A gastrointestinal polyp is a discrete mass of tissue protruding into the lumen of the stomach. Benign gastric polyps are reported to be found in 3-5% of patients who undergo esophagogastroduodenoscopy (EGD) [1, 2]. The most common types of gastric polyp are the hyperplastic polyps (Hpp) and fundic gland polyps (FGP) with relative prevalences of 60% and 30% respectively, followed by adenomas with a prevalence of 10-15%. Other less common epithelial stomach proliferations represent the remainder of polyps. These figures are derived from previous studies conducted over long periods of time in relatively small numbers of patients (Table 1) [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15].
| Country | Pub. year | Years | No. of polyps | Hpp | FGP | Adenoma | Carcinoma | Inflammatory | |
|---|---|---|---|---|---|---|---|---|---|
| Morais, et al. [8] | Brazil | 2007 | 5 | 153 | 71.30% | 16.30% | 12.40% | 2% | NR |
| Gencosmanoglu, et al. [6] | Turkey | 2003 | 5 | 150 | 64% | 14% | 3% | NR | 2% |
| Ljublcic [7] | Croatia | 2002 | 1 | 42 | 50% | 7% | 17% | NR | NR |
| Sivelli [14] | Italy | 2002 | 6 | 164 | 44.50% | NR | 16.40% | 0.60% | 4.9% |
| Attard [5] | USA | 2002 | 18 | 41 | 42% | 40% | 5% | NR | NR |
| Papa [10] | Italy | 1998 | 7 | 121 | 55.4% | 3.3% | 9.90% | 0.8% | 28.9% |
| Archimandritis, et al. [4] | Greece | 1996 | 4 | 258 | 75.6% | NR | 6.60% | NR | 17.8% |
| Stolte, et al. [13] | Germany | 1994 | 20 | 5515 | 28.3% | 47% | 9% | 7.20% | 3.1% |
| Rattan, et al. [11] | Israel | 1993 | 8 | 188 | 45.2% | NR | 3.2% | 5.3% | 29.3% |
| Roseau, et al. [12] | France | 1990 | 4 | 191 | 25.1% | 9.9% | 3.1% | NR | 61.8% |
| Deppisch, et al. [15] | USA | 1989 | 10 | 121 | 75% | 17% | 8.60% | NR | NR |
| Niv, et al. [9] | Israel | 1985 | 8 | 99 | 23.2% | 17.2% | 10.1% | NR | 25.3% |
| Laxen, et al. [3] | Finland | 1982 | 10 | 357 | 55% | NR | 8% | NR | 36% |
Table 1: Data from previous studies regarding prevalence of different types of gastric polyps around the world. Hpp: Hyperplastic
Hpp are usually sessile or pedunculated, are less than 2 cm in diameter [16], and typically occur in the antrum, although they can arise anywhere. Histologically, there is a proliferation of surface foveolar cells lining elongated, tortuous pits, imparting a corkscrew appearance that extends deep into the lamina propria. Gastric Hpp may contain pyloric glands, chief cells, and parietal cells, and their histologic appearance can overlap with hamartomas and inflammatory conditions [16]. The surface epithelium may also contain erosions or ulcerations leading to gastrointestinal bleeding [17].
Sporadic FGP are sessile polyps located in the body and fundus [16]. In general, their surface color is indistinguishable from that of normal gastric mucosa, and these lesions lack a stalk [18]. On microscopy, they contain dilated glands lined by gastric body mucosa, distorted glands and microcysts lined by parietal and chief cells; there is no or minimal inflammation [19]. Most endoscopists can diagnose these polyps on appearance alone with 89% accuracy [19]; the lesions appear as hyperemic, translucent, broad-based polyps with a smooth surface. The lesions vary in size from 1-8 mm and are most commonly found in middle-aged women [17], although much larger polyps are also seen in adult men and women of all age groups. An adenoma refers to dysplastic intestinal or gastric-type epithelium with variable architecture [1].
In addition to histopathology of gastric polyps, histopathology of gastric mucosa in patients with gastric polyps has also been reported in the literature. Apart from Helicobacter pylori gastritis (HPG), chronic inactive gastropathy (CIG), reactive gastritis (RG) and intestinal metaplasia (IM) were also seen in patients with gastric polyps [20]. HPG, CIG, IM are well defined in the literature. RG is the second most common pathologic diagnosis after HPG [21, 22]. RG refers to the chemical injury to the gastric mucosa leading to constellation of endoscopic and histologic findings [23]. The term “chemical gastropathy” was recommended by the updated Sydney System [21]. The common underlying causes of RG include chronic bile reflux and long-term intake of nonsteroidal anti-inflammatory drugs. Bile reflux usually occurs in patients who have undergone a Billroth II partial gastrectomy; it is also recognized to occur in intact stomachs in individuals with alcohol abuse, cigarette smoking, chronic respiratory disease, or duodenal ulcer, and even in healthy subjects [24, 25]. The mucosal changes seen in RG are usually most prominent in the antrum and pre-pyloric region but the more proximal oxyntic mucosa may also be affected. The endoscopic findings of RG are mostly nonspecific. The mucosa may be normal or may exhibit erythema, congestion, edema or erosions [24]. RG is characterized by prominent foveolar hyperplasia with elongation and tortuosity of the gastric pits that gives these structures a corkscrew appearance. The surface may appear villiform. The foveolar cells show regenerative changes with mucin depletion, nuclear hyperchromasia, and increased mitoses. Special stains for Helicobacter pylori (H. pylori) are negative. The microscopic features of RG were well characterized by Dixon et al in their original description of reflux gastritis as a distinct histopathologic entity [26]. Foveolar hyperplasia, smooth muscle fibers, vasodilatation and congestion are key histologic parameters for the diagnosis of RG [27].
In the west and in the United States in particular, data on gastric polyps have not been reevaluated on a large scale for 2 decades while several circumstances such as the treatment of H. pylori and the use of proton pump inhibitors (PPIs) have altered their relative and absolute frequency. In 2009, it was shown that relative prevalence of FGP was much higher than reported earlier, and was as high as 77% in contrast to previous studies showing 30% [20]. Whether this changing trend holds true in Asia and India has not been studied in large population in recent years.
We have not come across any study while reviewing literature were the gastric histopathology of polyp group (cases) has been compared with that of non-polyp group (controls).
This study was designed to investigate current trends in the prevalence of gastric specific polyps in the Asian population especially in Northern India. In addition the relationship with chronic gastritis was also evaluated in the cases and compared with types of gastritis in the controls. Apart from HPG, CIG, RG and IM; portal hypertensive gastropathy (PHTG) was also investigated.
Material and Methods
This was an observational retrospective study. Medical records of patients who underwent EGD in 3 gastroenterology departments of Northern India between 2011 and 2019 were reviewed. Biopsy specimens of patients with gastric polyps were also reviewed. It is a usual practice in these 3 centers to take gastric biopsies as per updated Sydney protocol while removing or biopsing a gastric polyp. In addition, gastric biopsies from controls were also reviewed. The policy for the evaluation of gastric biopsies in these centers is to specifically mention the presence or absence of H. pylori in the diagnostic report. When the H. pylori organism was not identified on hematoxylin and eosin stain, detection was aided by modified Giemsa stain. When staining results were negative but infection is nevertheless suspected on the basis of a histological finding of chronic active gastritis and lymphoid aggregates, a peroxidase conjugated monoclonal anti H. pylori immunostaining was carried out. Patients whose gastric biopsies were not assessed and properly graded as per the updated Sydney protocol were excluded from the study.
Data analysis: Statistical analysis was conducted using SPSS ver. 16.0 for Windows (SPSS, Chicago, IL). Categorical variables were compared using the chi-square or Fisher’s exact test where appropriate. Continuous data were compared using the t-test or the Mann-Whitney test, the Kruskal-Wallis test was used for multiple comparisons, when appropriate. Quantitative variables with a normal distribution were expressed as mean values ± standard deviation and those with a non-normal distribution as median values (range). Significance level was two-sided and set to less than 0.05.
Study was done after proper approval from institutional review board.
Results
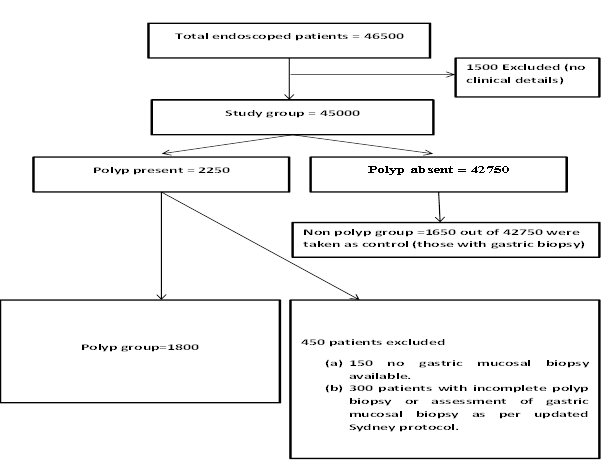
A total of 46500 patients who underwent EGD were screened. Of these, 1500 were excluded because the clinical details of the indications were inadequate; in the remaining 45000 patients 2250 polyps were seen on EGD. A further 450 patients were excluded for the following reasons: a. non-availability of concomitant gastric biopsies in 150 patients; and b. incomplete polyp pathology and assessment of chronic gastritis as per updated Sydney protocol in 300 patients (Figure 1).
There were 2250 patients without polyps who underwent biopsy for different upper gastrointestinal symptoms like dyspepsia, abdominal pain, anemia, melena, and gastroesophageal reflux disease. However, only 1650 patients had gastric biopsy assessed as per the updated Sydney protocol and these were taken as a control group (Figure 1).
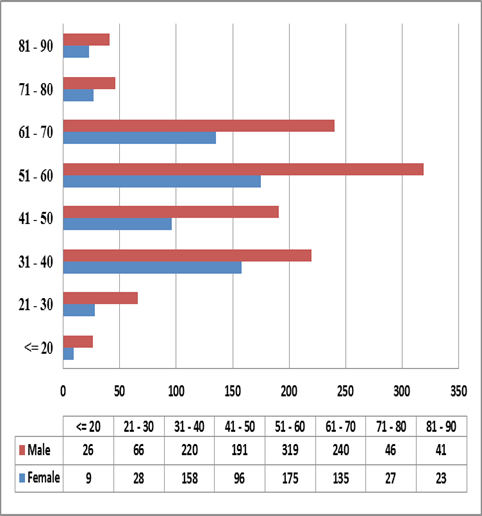
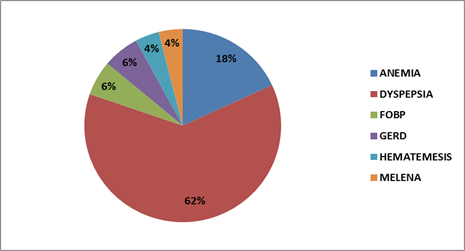
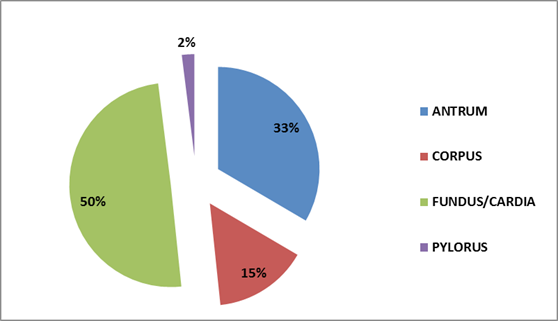
Of the 1800 patients in the polyp group, 1149 (63.80%) were male and 651 (36.20%) female (Figure 2). Overall, gastric polyps were found in 2250 of 45000 patients, i.e., 5% of the study population. The most frequent presenting complaint of patients with gastric polyps was dyspepsia followed by anemia and others as given in Figure 3. The distribution of polyps in the stomach is in Figure 4. Polyps were most common in the fundus. There were 900 FGP (50%), 750 (42.05%) Hpp, and 143 (7.94%) others; others include adenomatous polyps, leiomyomas, pancreatic rest, lipoma, lymphoma, neuroendocrine tumors, xanthomas, adenocarcinoma and gastrointestinal stromal tumor as shown in Table 2. Synchronous polyps were also recorded in 19 patients.
| Histology of polyp | Antrum | Corpus | Fundus/Cardia | Pylorus | Total | |
|---|---|---|---|---|---|---|
| AC | 2 | 6 | 4 | 5 | 17 | |
| AP | 7 | 26 | 16 | 5 | 54 | |
| FGP | 174 | 94 | 626 | 6 | 900 | |
| GIST | 0 | 1 | 1 | 0 | 2 | |
| Hpp | 390 | 130 | 227 | 10 | 757 | |
| Leiomyoma | 0 | 1 | 1 | 0 | 2 | |
| Lipoma | 2 | 0 | 1 | 1 | 4 | |
| Lymphoma | 1 | 1 | 1 | 3 | 6 | |
| NET | 15 | 9 | 9 | 3 | 36 | |
| Pancreatic rest | 4 | 0 | 0 | 2 | 6 | |
| Xanthoma | 6 | 1 | 8 | 1 | 16 | |
| Total | 601 | 269 | 894 | 36 | 1800 |
Table 2: Location of polyps in stomach in our study (n=1800). AC: Adenocarcinoma; AP: Adenomatous Polyp; FGP: Fundic Gland Polyps
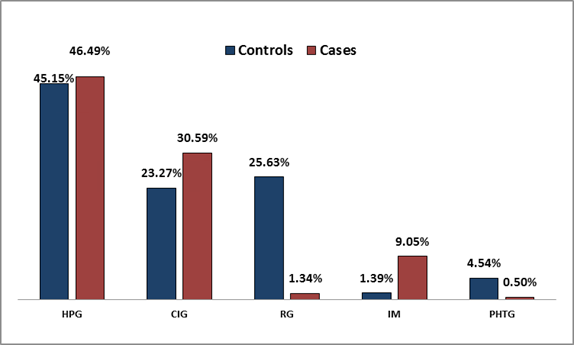
Background gastric histopathology in the cases is presented in Tables 3. 7.55% of the FGP patients and 45.70% of the Hpp patients had HPG. The histopathology of gastric mucosa in the cases compared to the controls is presented in Table 4. 46.49% of the cases and 45.15% of controls had HPG; 30.59% of the cases and 23.27% of controls had CIG;
1.34% of the cases and 25.63% of controls had RG; and 9.05% of the cases and 1.39% of controls had IM. PHTG was seen in 0.50% of the cases and 4.54% of the controls. These results show that the proportions of different types of gastritis found in the cases were significantly different from those in the controls (P<0.001).
| Histology of polyp | NGM | CIG | HPG | IM | PHTG | RG | Total | |
|---|---|---|---|---|---|---|---|---|
| AC | 4 | 3 | 4 | 3 | 0 | 3 | 17 | |
| AP | 11 | 8 | 21 | 7 | 0 | 7 | 54 | |
| FGP | 543 | 171 | 68 | 37 | 3 | 78 | 900 | |
| GIST | 2 | 0 | 0 | 0 | 0 | 0 | 2 | |
| Hpp | 224 | 108 | 346 | 37 | 2 | 40 | 757 | |
| Leiomyoma | 1 | 1 | 0 | 0 | 0 | 0 | 2 | |
| Lipoma | 3 | 0 | 1 | 0 | 0 | 0 | 4 | |
| Lymphoma | 2 | 1 | 1 | 1 | 0 | 1 | 6 | |
| NET | 20 | 4 | 7 | 3 | 0 | 2 | 36 | |
| Pancreatic Rest | 2 | 2 | 1 | 1 | 0 | 0 | 6 | |
| Xanthoma | 5 | 2 | 8 | 0 | 0 | 1 | 16 | |
| Total | 817 | 300 | 457 | 89 | 5 | 132 | 1800 |
Table 3: Type of background gastric histopathology in polyp group (n=1800). AC: Adenocarcinoma; AP: Adenomatous Polyp; FGP: Fundi
Table 3: Type of background gastric histopathology in polyp group (n=1800). AC: Adenocarcinoma; AP: Adenomatous Polyp; FGP: Fundic Gland Polyps; Hpp: Hyperplastic Polyps; GIST: Gastrointestinal Stromal Tumor; NET: Neuroendocrine Tumor; NGM: Normal Gastric Mucosa; CIG: Chronic Inactive Gastropathy; HPG: Helicobacter Pylori Gastritis; IM: Intestinal Metaplasia; PHTG: Portal Hypertensive Gastropathy; RG: Reactive Gastritis.
| Histopathology of gastric mucosa | Non-polyp (n) | Percentage | Polyp (n) | Percentage | P-value |
|---|---|---|---|---|---|
| HPG | 745 | 45.15% | 457 | 46.49% | <0.001 |
| CIG | 384 | 23.27% | 300 | 30.59% | |
| RG | 423 | 25.63% | 132 | 1.34% | |
| IM | 23 | 1.39% | 89 | 9.05% | |
| PHTG | 75 | 4.54% | 5 | 0.50% | |
| Total | 1650 | 983 |
Table 4: Comparison of background histopathology in non-polyp (n=1650) with polyp patients (n=983).
HPG: Helicobacter Pylori Gastritis; CIG: Chronic Inactive Gastropathy; RG: Reactive Gastritis; IM: Intestinal Metaplasia; PHTG: Portal Hypertensive Gastropathy. Table 4: Comparison of background histopathology in non-polyp (n=1650) with polyp patients (n=983).
Discussion
There is a changing trend in the relative prevalence of types of gastric polyps throughout the world. The relative prevalence of FGP even in a Northern Indian population was much higher than that reported in the earlier literature. This may be due to the widespread use of PPIs and aggressive treatment of H. pylori. In a large retrospective evaluation of gastric polyps from 5515 patients over a 20- year period, reviewed by Stolte, et al. [13], the incidence of Hpp was 28.30%, compared with 47% for FGP and 10% for adenomatous polyps. In contrast, in 1996, Archimandritis from Greece [4] reported that the majority of polyps (75%) were Hpp. In a study from Brazil by Morais DJ, et al. [8], 70% of gastric polyps were Hpp and 16% were FGP. Ljubicic, et al. [7] investigated the frequency, location, age and sex distribution of various histological types of benign gastric epithelial polyps in 31 patients and found 42 benign gastric epithelial polyps in 31 patients, with 21 Hpp, 7 adenomatous, and 3 FGP polyps. All patients with Hpp had chronic active superficial gastritis. Among 21 patients with Hpp 76% were positive for H. pylori infection, in contrast to only 2 (29%) of those with adenomatous polyps and 33% of those with FGP. Rattin, et al. [11] reported 188 polyps with similar results. Deppisch, et al. [15] in 1998 reported an Hpp prevalence of 75% from the USA. In 2009, Carmack, et al. [20] reported a change in the trend for gastric polyp prevalence in a large series from the United States. In that series the prevalence of gastric polyps was 6.35% and they found a relative prevalence of 77% for FGP in their population; this was much higher than had been reported earlier and was probably due to the widespread use of PPIs. In western countries the most commonly encountered polyps are FGP because of aggressive anti H. pylori treatment and because PPIs use is common [28, 29, 30]. The frequency of the most common type of polyp varies widely depending upon the population studied as Hpp and adenomatous polyps are relatively more frequent than FGP in regions with H. pylori infection [21, 30, 31, 32, 33].
Our population frequently uses PPIs and with the aggressive awareness regarding H. pylori treatment in the last 15 years we also expected a change in the prevalence of different types of polyp. In our study gastric polyps were seen in 2250 patients overall, i.e., 5%; the most common types of polyp were FGP 50% followed by Hpp 42.05%, while around 894 polyps (49.70%) were located in the fundus region. Our data differ significantly from those reported earlier from the United States and other countries as shown in Table 1, the most remarkable discrepancy being in the relative prevalence of FGP. In 1989 they represented 17% of all gastric polyps in United States [15], and 10% in France [12], whereas during the years 2001-2006 they accounted for 16.3% of all polyps reported in a large Brazilian series [8]. The highest relative prevalence in the literature is 47% reported in a 20-year German study [13]. In our series FGP made up 50% as mentioned above. These polyps were considered to be hamartomata in the past; they tend to arise in patients with H. pylori free stomachs who receive chronic PPIs treatment [34, 35, 36]. Given the widespread use of PPIs in Northern India especially in Jammu Kashmir because of the typical spicy dietary habits and the on counter use and free availability of PPIs even in remote areas of the state combined with better gastroenterological care to get these polyps biopsied, we also expected an increased prevalence of FGP.
In our study we selected patients with polyps who had a concomitant gastric biopsy in accordance with the updated Sydney protocol to identify the associated type of chronic gastritis. HPG was seen in only 7.55% of FGP cases. Hpp are believed to be associated with H. pylori infection and atrophic gastritis [37, 38]. In our study these lesions were seen in 42.05 % of patients in contrast to more than 2/3 in Brazil, Turkey, Greece and the USA [4, 6, 8, 15], and approximately 1/2 in Finland, Croatia, Italy and Israel [3, 7, 10, 11]. The continuing decline in H. pylori infection as well as the simultaneous increase in FGP may have contributed to the low relative prevalence of Hpp. In our study 45.70% of Hpp were associated with HPG, in contrast to only 7.55% for FGP. In the cases, 46.49% had HPG compared with 45.15% of the controls, probably because of the high background prevalence of H. pylori infection. In addition, most of the polyps were FGP which was to be expected in patients who make extensive use of PPIs and probably undergo more H. pylori eradication. In the cases, 30.59% of patients had CIG compared with 23.27% of the controls; similarly 1.34% of the cases had RG compared with only 25.63% of the controls. These results show that the prevalences of different types of gastritis were significantly different in the cases compared to the controls as reported earlier [39] and the difference was significant (Figure 5) (P<0.001). It could be suggested that some forms of gastritis may increase the risk of gastric polyp; however, this needs further studies for validation. The explanation for FGP being common polyps may be the changing trend in PPIs use and aggressive H. pylori treatment [28, 29, 40, 41]; there has been a change in the spectrum of gastric polyps with the frequency of FGPs increasing from 19% (15/80) to 77% (638/828) while Hpp decreased from 65% (52/80) to 15% (123/828) [40]. However, our study may be biased by the inclusion of more patients with dyspepsia and excessive PPIs use in the cases as clinical details regarding the use of PPIs or anti-H.pylori treatment were not available. HPG was still found in more than 40% of the controls which may represent the true prevalence of H. pylori in the population. Our study also highlights that only 0.50% of gastric polyps in the cases has background PHTG, whereas PHTG was seen in 4.54% of the controls. It seems that there is a low prevalence of gastric polyps in PHTG but this needs further studies for confirmation.
In conclusion, our study is the first to describe the changing relative prevalence of different gastric polyps in a Northern Indian population, with overall prevalence of 5%. There is rising trend of FGP possibly signifying increasing PPI use and H. pylori eradication therapy. Our study also highlights the specific types of chronic gastritis in cases compared with controls, is showing significant differences (p<0.001). HPG, CIG and IM were more frequent in the cases whereas RG and PHTG were more frequent in the controls. These results are interesting and provide new perspective to look into pathogenesis of gastric polyps.
Summary Box
What is already known? Most studies around the world report a prevalence of gastric polyps of around 3-5% There is a changing trend in the histopathology of gastric polyps in world, as reported in the western literature What the new findings are:
- Our study found the prevalence of gastric polyps in our region was 5%.
- Our study is first to highlight the increasing trend of FGP constituting 50% (most common type) of gastric polyps from North India.
- There is high background prevalence of HPG (45.72%) in cases with Hpp.
- IM was present in 9.05% of cases and only in 1.39% of controls. RG was present in 1.34% of cases whereas in 25.63% of controls (p<0.001).
References
-
Turner JR, Odze RD (2004) Polyps of the stomach. In: Odze RD, Goldblum JR, Crawford JM (Eds.), Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas, (1st Edn.), Saunders-Elsevier: Philadelphia, pp: 267-294.
-
Bhatttacharya B (2005) Non-neoplastic disorders of the stomach. In: Iacobuzio-Donahue CA, Montgomery EA (Eds.), Gastrointestinal and Liver Pathology, (1st Edn.), Churchil-Livingstone-Elsevier: Philadelphia, pp: 66-126.
-
Laxén F, Sipponen P, Ihamäki T, Hakkiluoto A, Dortscheva Z (1982) Gastric polyps; their morphological and endoscopical characteristics and relation to gastric carcinoma. Acta Pathol Microbiol Immunol Scand A 90(3): 221-228.
-
Archimandritis A, Spiliadis C, Tzivras M, Vamvakousis B, Davaris P, et al. (1996) Gastric epithelial polyps: a retrospective endoscopic study of 12,974 symptomatic patients. Ital J Gastroenterol 28(7): 387-390.
-
Attard TM, Yardley JH, Cuffari C (2002) Gastric polyps in pediatrics: an 18-year hospital-based analysis. Am J Gastroenterol 97(2): 298-301.
-
Gencosmanoglu R, Sen OE, Kurtkaya YO, Avsar E, Sav A, et al. (2003) Gastric polypoid lesions: analysis of 150 endoscopic polypectomy specimens from 91 patients. World J Gastroenterol 9(10): 2236-2239.
-
Ljubicić N, Kujundzić M, Roić G, Banić M, Cupić H, et al. (2002) Benign epithelial gastric polyps; frequency, location, and age and sex distribution. Coll Antropol 26: 55-60.
-
Morais DJ, Yamanaka A, Zeitune JM, Andreollo NA, Ademar Y (2007) Gastric polyps: a retrospective analysis of 26,000 digestive endoscopies. Arq Gastroenterol 44(1): 14-17.
-
Niv Y, Bat L (1985) Gastric polyps, a clinical study. Isr J Med Sci 21(10): 841-844.
-
Papa A, Cammarota G, Tursi A, Montalto M, Cuoco L, et al. (1998) Histologic types and surveillance of gastric polyps: a seven year clinico-pathological study. Hepatogastroenterology 45(20): 579-582.
-
Rattan J, Arber N, Tiomny E, Moshkowitz M, Chapsky Y, et al. (1993) Gastric polypoid lesions-an eight-year study. Hepatogastroenterology 40(2): 107-109.
-
Roseau G, Ducreux M, Molas G, Ponsot P, Amouyal P, et al. (1990) Epithelial gastric polyps in a series of 13000 gastroscopies. Presse Med 19(4): 650-654.
-
Stolte M, Sticht T, Eidt S, Ebert D, Finkenzeller G (1994) Frequency, location, and age and sex distribution of various types of gastric polyp. Endoscopy 26(8): 659- 665.
-
Sivelli R, Del Rio P, Bonati L, Sianesi M (2002) Gastric polyps: a clinical contribution. Chir Ital 54(1): 37-40.
-
Deppisch LM, Rona VT (1989) Gastric epithelial polyps. A 10-year study. J Clin Gastroenterol 11(1): 110-115.
-
Goddard AF, Badreldin R, Pritchard DM, Walker MM, Warren B (2010) British Society of Gastroenterology. The management of gastric polyps. Gut 59(9): 1270- 1276.
-
Chandrasekhara V, Ginsberg GG (2011) Endoscopic management of gastrointestinal stromal tumors. Curr Gastroenterol Rep 13(6): 532-539.
-
Burt RW (2003) Gastric fundic gland polyps. Gastroenterology 125: 1462-1469.
-
Weston BR, Helper DJ, Rex DK (2003) Positive predictive value of endoscopic features deemed typical of gastric fundic gland polyps. J Clin Gastroenterol 36(5): 399-402.
-
Carmack SW, Genta RM, Schuler CM, Saboorian MH (2009) The current spectrum of gastric polyps: a 1-year national study of over 120,000 patients. Am J Gastroenterol 104(6): 1524-1532.
-
Owen DA (2003) Gastritis and carditis. Mod Pathol 16(4): 325-341.
-
Carrasco G, Corvalan AH (2013) Helicobacter pylori- induced chronic gastritis and assessing risks for gastric cancer. Gastroenterol Res Pract 2013: 393015.
-
Dixon F, Genta RM, Yardley JH, Correa P (1996) participants in the International Workshop on the Histopathology of Gastritis. Classification and grading of gastritis. The updated Sydney system. Houston 1994. Am J Surg Pathol 20(10): 1161-1181.
-
El-Zimaity HM, Genta RM, Graham DY (1996) Histological features do not define NSAID-induced gastritis. Hum Pathol 27(12): 1348-1354.
-
Maguilnik I, Neumann WL, Sonnenberg A, Genta RM (2012) Reactive gastropathy is associated with inflammatory conditions throughout the gastrointestinal tract. Aliment Pharmacol Ther 36(8): 736-743.
-
Dixon MF, O Connor HJ, Axon AT, King RF, Johnston D (1986) Reflux gastritis: distinct histopathological entity? J Clin Pathol 39: 524-530.
-
Wolf EM, Plieschnegger W, Schmack B, Bordel H, Höfler B, et al. (2014) Evolving patterns in the diagnosis of reactive gastropathy: data from a prospective Central European multicenter study with proposal of a new histologic scoring system. Pathol Res Pract 210(2): 847- 854.
-
Cao H, Wang B, Zhang Z, Zhang H, Qu R (2012) Distribution trends of gastric polyps: an endoscopy database analysis of 24 121 northern Chinese patients. J Gastroenterol Hepatol 27(7): 1175-1180.
-
Peretz A, Fuchs T, Livovsky DM, Turvall E, Pappo O, et al. (2012) The changing histological pattern of gastric polyps in an ethnically heterogeneous population. Scand J Gastroenterol 47(8-9): 907-913.
-
Velázquez Dohorn ME, López Durand CF, Gamboa Domínguez A (2018) Changing trends in gastric polyps. Rev Inves Clin 70: 40-45.
-
Ohkusa T, Miwa H, Hojo M, Kumagai J, Tanizawa T, et al. (2003) Endoscopic, histological and serologic findings of gastric hyperplastic polyps after eradication of Helicobacter pylori: comparison between responder and non-responder cases. Digestion 68: 57-62.
-
Zelter A, Fernández JL, Bilder C, Rodríguez P, Wonaga A, et al. (2011) Fundic gland polyps and association with proton pump inhibitor intake: a prospective study in 1,780 endoscopies. Dig Dis Sci 56(6): 1743-1748.
-
Elhanafi S, Saadi M, Lou W, Indika M, Alok D, et al. (2015) Gastric polyps: Association with Helicobacter pylori status and the pathology of the surrounding mucosa, a cross sectional study. World J Gastrointest Endosc 7(10): 995-1002.
-
Freeman HJ (2008) Proton pump inhibitors and an emerging epidemic of gastric fundic gland polyposis. World J Gastroenterol 14: 1318-1320.
-
El-Zimaity HM, Jackson FW, Graham DY (1997) Fundic gland polyps developing during omeprazole therapy. Am J Gastroenterol 92: 1858-1860.
-
Raghunath AS, O Morain C, McLoughlin RC (2005) Review article: the long-term use of proton-pump inhibitors. Aliment Pharmacol Ther 22(1): 55-63.
-
Dirschmid K, Platz-Baudin C, Stolte M (2006) Why is the hyperplastic polyp a marker for the precancerous condition of the gastric mucosa? Virchows Arch 448: 80- 84.
-
Laxén F, Kekki M, Sipponen P, Siurala M (1983) The gastric mucosa in stomachs with polyps: morphologic and dynamic evaluation. Scand J Gastroenterol 18(4): 503-511.
-
Montenegro-Molina W, Zamorano-Orozco Y, Martinez- Garcia CL (2011) Prevalence of gastric polyps and histological correlation at the “Dr. Carlos Mac Gregor Sanchez Navarro” Hospital. Endoscopia 23(1): 23-28.
-
Fan NN, Yang J, Sun G, Lu ZS, Ling Hu EQ, et al. (2015) Changes in the spectrum of gastric polyps in the Chinese population. World J Gastroenterol 21(33): 9758-9764.
-
Tran Duy A, Spaetgens B, Hoes AW, de Wit NJ, Stehouwer CDA (2016) Use of proton pump inhibitors and risk of fundic gland polyps and gastric cancer: Systematic review and meta-analysis. Clin Gastroenterol Hepatol 14(12): 1706-1719.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient