Cytokeratin 20 Positive with HepPar-1 Negative in Hepatocellular Carcinoma - A Potential Diagnostic Pitfall in the Pathological Interpretation of Needle Core Liver Biopsy
Needle core biopsy of liver lesions in adults with a clinical query of metastases is commonly encountered in general surgical pathology practice. The presence of poorly differentiated malignant cells forming ill-formed glands favors a working pathological diagnosis of metastatic carcinoma. If metastatic, determination of the primary site of origin is the next diagnostic challenge that faces the pathologist. An algorithmic IHC approach using cytokeratins and lineage markers often narrows the diagnostic possibilities with definition of tumor type and assigns site of origin. However, aberrant staining patterns are major potential diagnostic pitfalls. We present the case of a needle core liver biopsy with a poorly differentiated pseudoglandular HCC component that showed diffuse Cytokeratin (CK) 20 positivity with absent CK7 and Hepatocyte Paraffin-1 (HepPar-1) staining that was initially misinterpreted as metastatic adenocarcinoma from the lower gastrointestinal tract. However, with systematic integration of complete clinical, endoscopic and radiological data with reevaluation of the surrounding ‘non-neoplastic’ liver, the pathological diagnosis confirmed the presence of hepatocellular carcinoma arising in a background of chronic hepatitis C related cirrhosis, with a poorly differentiated pseudo glandular component associated with loss of HepPar-1 staining and aberrant strong diffuse positivity with CK20 posing as a diagnostic pitfall in the interpretation of limited material on needle core biopsies of mass lesions in an adult liver. Needle core biopsy of liver lesions in adults with a clinical query of metastases is commonly encountered in general surgical pathology practice. The presence of poorly differentiated malignant cells forming ill-formed glands favors a working pathological diagnosis of metastatic carcinoma. If metastatic, determination of the primary site of origin is the next diagnostic challenge that faces the pathologist. An algorithmic IHC approach using cytokeratins and lineage markers often narrows the diagnostic possibilities with definition of tumor type and assigns site of origin. However, aberrant staining patterns are major potential diagnostic pitfalls. We present the case of a needle core liver biopsy with a poorly differentiated pseudoglandular HCC component that showed diffuse Cytokeratin (CK) 20 positivity with absent CK7 and Hepatocyte Paraffin-1 (HepPar-1) staining that was initially misinterpreted as metastatic adenocarcinoma from the lower gastrointestinal tract. However, with systematic integration of complete clinical, endoscopic and radiological data with reevaluation of the surrounding ‘non-neoplastic’ liver, the pathological diagnosis confirmed the presence of hepatocellular carcinoma arising in a background of chronic hepatitis C related cirrhosis, with a poorly differentiated pseudo glandular component associated with loss of HepPar-1 staining and aberrant strong diffuse positivity with CK20 posing as a diagnostic pitfall in the interpretation of limited material on needle core biopsies of mass lesions in an adult liver. We conclude with key learning points in the diagnostic interpretation of needle core liver biopsies from mass lesions in an adult liver with an underlying caveat to “never diagnose liver biopsies in ‘pathological isolationâ€.
Introduction
Needle core biopsy of liver mass lesions in adults with a clinical query of metastases is commonly encountered in a general surgical pathology practice, as the commonest cause of multiple solid lesions in the adult liver is metastatic disease. The distinction between multifocal primary hepatocellular carcinoma [HCC] and metastatic adenocarcinoma can be extremely difficult when these tumors are poorly differentiated, and in particular, if the biopsy size is limited to a needle core biopsy [1, 2]. However, as the management and prognosis of these tumors are very different, additional staining with an optimal panel of immunohistochemical [IHC] antibodies including hepatocyte markers are used which are usually helpful in this distinction. Additionally, if metastatic, determination of the primary site of origin is the next diagnostic challenge that faces the pathologist. In this context, an algorithmic IHC approach using cytokeratins and lineage markers are often used to narrow the diagnostic possibilities with definition of tumor type and assigns site of origin [3].
We present a case herewith of a liver biopsy with a poorly differentiated pseudoglandular HCC component that showed diffuse CK 20 positivity with absent CK7 and Hep Par-1 staining that was initially misdiagnosed as metastatic adenocarcinoma from the lower gastrointestinal tract. However, with systematic integration of complete clinical, endoscopic, radiological data and with reevaluation of the surrounding ‘non-neoplastic’ liver, the pathological diagnosis was revised to the presence of HCC arising in a background of chronic hepatitis C related cirrhosis, with a poorly differentiated pseudoglandular component associated with loss of staining to Hep Par-1 and aberrant strong diffuse positivity with CK20 posing as a diagnostic pitfall in the interpretation of limited material on needle core biopsies of multiple liver lesions in an adult.
Case Report
A 62 year old man with emphysema who was undergoing investigation for a spiculated lesion of concern in the lateral segment of right middle lobe of the lung, presented with lower abdominal pain with diarrhea. Upon clinical examination, he was found to have an enlarged liver. A previous PET scan had reported a possible malignant lesion in the proximal sigmoid. CT scan abdomen /pelvis showed the presence of multiple hypo-attenuating lesions in segments 3, 5 and 6 in the right lobe of the liver, measuring 1cm, 3.7 and 3.6 cm respectively, which were radiologically in keeping with metastatic disease as seen in Figure 1. In order to establish a definitive diagnosis, an ultrasound guided needle core liver
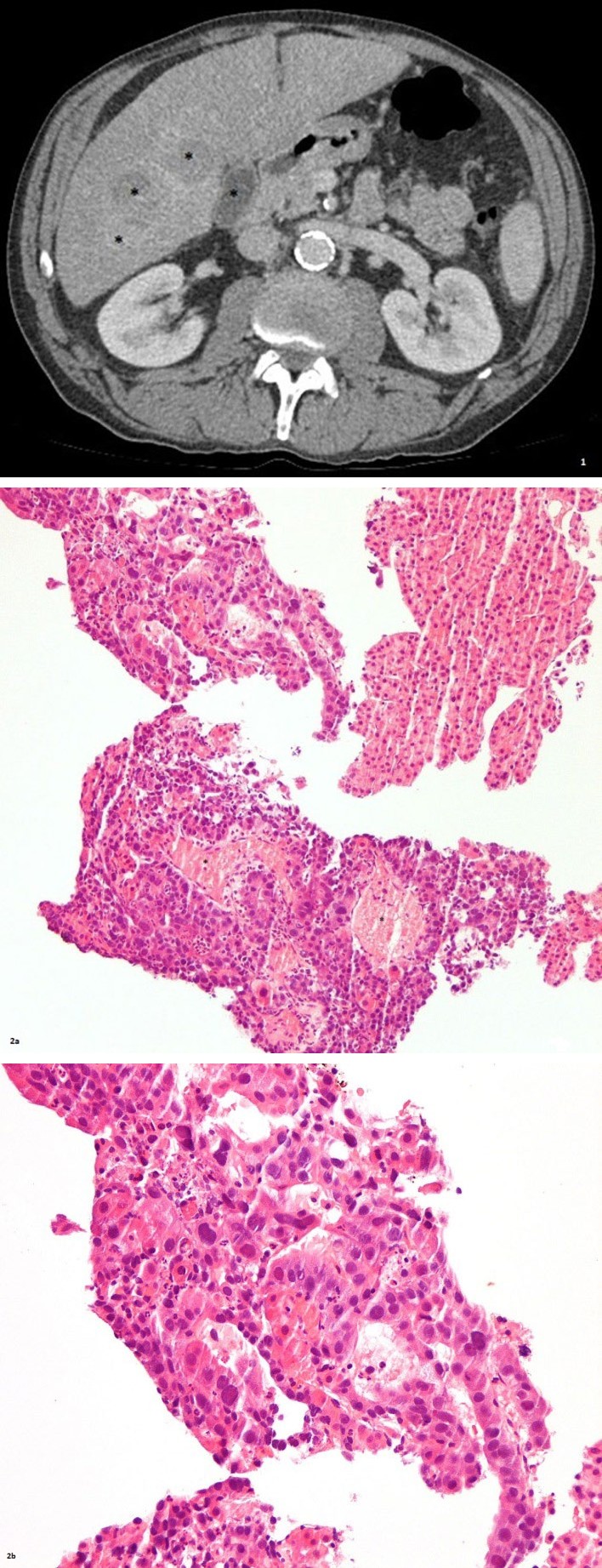
2(a) 2(b) biopsy was performed.
The needle core biopsies were formalin-fixed, paraffin- embedded and routinely processed. Routine three levels of hematoxylin-eosin stained slides were evaluated. The core biopsy showed fragments of unremarkable liver associated with partial sampling of a poorly differentiated malignant neoplasm composed of neoplastic cells, forming ill-defined glands, associated with central necrosis as seen in Figures 2a, 2b which was morphologically consistent with the clinical impression of a metastatic colonic adenocarcinoma. Immunohistochemical stains were performed using antibodies against CK7, CK20, CDX-2, TTF-1 and HepPar-1 with positive and negative controls. The neoplastic cells showed diffuse strong positive staining for CK20 (Figure 2c) and were negative for CK7, CDX2, TTF1 and HepPar-1 (Figure 2d). In this context, the initial pathological diagnosis favored metastatic adenocarcinoma consistent with a lower gastrointestinal (presumed colonic) site of origin.
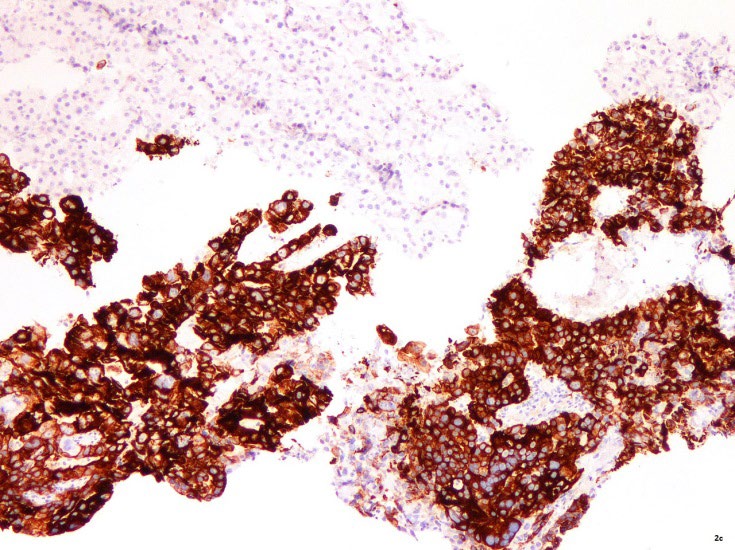
2(c) 2(d) Figure 2: Hematoxylin and eosin stained slides at medium (a) and high magnification (b) show the presence of a fragment of unremarkable liver (top left hand corner) admixed with fragments of a poorly differentiated malignant neoplasm composed of neoplastic cells forming ill-defined glands associated with central necrosis*. Immunohistochemically stained slides with antibodies to CK20 and HepPar-1 shows diffuse strong positive homogenous staining with CK20 (c) and no expression of HepPar-1 in the neoplastic cells at the bottom of the picture panel (d) Reverse pattern of staining is seen in the adjacent fragment of uninvolved liver at the top of the picture panel.
An extensive gastrointestinal workup, including repeat dedicated imaging with upper and lower endoscopies were undertaken. No definitive primary gastrointestinal lesion was found.
![Figure 3: MRI Follow-up 2months. MRI liver with contrast shows several [4-5] heterogeneous solid hepatic masses* within the right hepatic lobe associated with thrombus of the right portal vein^ and smaller early enhancing foci in the left hepatic lobe with signal and enhancement characteristics concerning for multifocal hepatocellular carcinoma.](/fulltextimages/5849/fig_3.jpeg)
Additional medical history of pre-existing liver disease of chronic hepatitis C was now available. Continued serum monitoring over the next few months showed rising alpha- fetoprotein levels. Follow up MRI liver with contrast now showed several, four to five, heterogeneous solid hepatic masses within the right hepatic lobe, associated with thrombus of the right portal vein, and smaller early enhancing foci in the left hepatic lobe with signal and enhancement characteristics concerning for multifocal hepatocellular carcinoma (Figure 3).
The liver biopsies were reviewed together with evaluation of the surrounding ‘non-neoplastic’ liver parenchyma in additional needle cores. Histological examination of the surrounding liver biopsies showed the presence of a densely fibrotic nodular liver with atypical hepatocytes arranged in 3-4 cell thick plates (Figure 4a) that focally formed pseudo glands with loss of normal reticulin staining (Figure 4b) in keeping with moderately well differentiated hepatocellular carcinoma arising in the background of a densely fibrotic liver (Figure 4c). Staining with CD34 highlighted the sinusoidal capillarization of the neoplastic cells (Figure 4d) as typically observed in HCC. These neoplastic cells strongly expressed HepPar-1 (Figure 4e) and showed no expression of CK7 or CK20 (Figure 4e). Mild increased portal inflammation and steatosis (Figure 4f) associated with hepatic siderosis was also observed in the surrounding liver cores (Figure 4h) in keeping with the clinical history of chronic hepatitis C.
In keeping with the detailed clinical history now available, associated with the updated endoscopic and radiological imaging and re-evaluation of the liver biopsies, including study of the surrounding ‘non-neoplastic’ liver, the pathological diagnosis was revised to the presence of HCC arising in a background of chronic hepatitis C with cirrhosis, with a poorly differentiated pseudo glandular component associated with loss of staining to HepPar-1, and aberrant

strong diffuse positivity with CK20, posing as a diagnostic pitfall in the interpretation of limited material on needle core biopsies of mass lesions in an adult liver.
4a 4b 4c
4d 4e 4f
4g 4h Figure 4: Hematoxylin and eosin stained slides at medium magnification showing atypical hepatocytes arranged in 3-4 cell thickened plates that focally forms pseudo glands (a) with loss of normal staining pattern with reticulin (b) in keeping with moderately well differentiated hepatocellular carcinoma arising in the background of a densely fibrotic liver as highlighted by intense blue staining of the collagen with Masons trichrome stain, inset with higher magnification (c). Immunohistochemically stained slides with antibodies to CD 34 demonstrates the typical sinusoidal capillarization of the neoplastic liver cells (d). Staining with HepPar-1 antibody is expressed in the neoplastic cells € while staining with CK20 antibodies is negative (f). Hematoxylin and eosin stained slides of the non-neoplastic liver parenchyma at low magnification (g) shows mild increased portal inflammation*with mild steatosis^, while Perl’s stained slides show mild increased iron deposition as blue granules (h).
Discussion
The clinical working diagnosis of multiple solid liver nodules in an adult is metastatic disease with the possibility of multifocal HCC being one of much lower probability. In this context, though the International Working Party has established clear criteria for the histological diagnosis of HCC, the differential diagnosis of HCC, especially the poorly differentiated pseudoglandular phenotype, from metastatic colon cancer is not easy, especially, when diagnostic material is limited to needle core biopsies. Fanni D, et al. [1], International Working Party [4], Mourra N, et al. [5] In this context, additional immunohistochemical studies play an important role in the diagnostic workup and it has been suggested that the best panel for discriminating HCC from metastatic adenocarcinoma should include HepPar-1, MOC- 31, pCEA, CD10 and CD34 [6].
The IHC approach to a ‘garden variety’ adenocarcinoma in the liver includes CK7, CK20, CDX2, TTF-1 and GATA-3 if female, as this panel is targeted to identify breast, lung, tubal gut and pancreaticobiliary origin of tumors. Coordinate expression of CK7/CK20 are the most commonly used epithelial lineage markers to assign site of origin in metastatic carcinomas of occult origin. A homogenous diffuse staining pattern of CK7-ve /CK20+ve, combined with a morphological impression of garden variety adenocarcinoma, supports a lower gastrointestinal site of origin, as at least 80% of colon cancers demonstrate the classic CK7-/CK20+ve immunophenotype [3, 7, 8]. Semiquantitative assessments of staining patterns are useful, as isolated focal staining patterns are not diagnostically relevant. Usually, colonic tumors also have strong homogenous co-expression of CDX2. Though in our case there was no co-expression of CDX2, it is important to note that upto 5% of HCCs can express CDX2 with some reports documenting co-expression of CDX2 and CK20 in poorly differentiated HCC with central necrosis, thus, truly mimicking metastatic colonic adenocarcinoma [9, 10].
Hepatocellular differentiation markers include HepPar-1, glypican-3 and arginase-1. HepPar-1 recognizes the urea cycle enzyme carbomyl phosphate synthetase I (CPS I) in hepatocytes and is very sensitive with strong expression in well (>95%), moderately (>90%) and less so in poorly differentiated (50-80%) hepatocellular carcinomas.3 HepPar-1 is expressed in most of the HCCs and is considered the most reliable marker for HCC differentiation. Yet, it is to be remembered that patchy staining is seen in about 20% of HCCs and therefore liver needle core biopsies representing limited sampling can be negative.2 Additionally, as the sensitivity for HepPar-1 in poorly differentiated HCC can drop to 30%, recently, arginase has been recommended as the most sensitive marker in all differentiations of HCC and in combination with Glypican-3 enables identification of all cases of poorly differentiated HCC [6, 11].
Cytokeratin 20 [CK20], a 46-kDA polypeptide related cytokeratin expression in normal human tissues is restricted to gastric and intestinal epithelium [5, 12], Merkel cells of the skin [13] and transitional epithelium [14] and is absent in the liver [1]; thus, by extension, CK20 is therefore expressed in tumors that are derived from the gastrointestinal tract, urothelium and Merkel cells and is not expressed in HCC. In Porcell’s study none of the 13 cases of HCC expressed CK20 and they concluded that if CK20 is strongly expressed it excludes HCC [15]. In Wang’s study of 400 epithelial tumors only 2 of the 30 HCCs [6.66%] showed CK20 expression7 while Mourra and Karabork’s study reported up to 14.7% of HCCs were positive for CK20 [5, 6]. Aberrant expression of CK20 in the liver, if present, is usually restricted to a small subpopulation of tumor cells. The reason underlying this atypical, aberrant expression is largely unknown. However, it has been shown that there is strong proliferation of CK20+ve cells following experimentally induced cholestasis, thus proposing that keratin expression do not entirely reflect histogenesis, but this phenomenon may be influenced by epigenetic factors. Fanni D, et al. [1], Faa G, et al. [16] case reports of diffuse strong positivity of HCC tumor cells with CK20 are also increasingly being reported. Fanni D, et al. [1], Mourra N, et al. [5] in both these reports, the tumor cells retained their staining with HepPar-1, while in our case report, the tumor cells being poorly differentiated, additionally, had lost their staining to HepPar-1 (Figure 2d) thus contributing to the diagnostic interpretive error. Therefore, diffuse immunoreactivity for CK20 alone as seen in Fig 2c does not rule out the diagnosis of HCC especially if the HCC is poorly differentiated5 as seen in Figs 2a and 2b. Moreover, as the staining pattern of HepPar-1 is patchy, heterogeneous and variable, it is possible that, the false negative result in our case (Figure 2d) was compounded by limited sampling of only the poorly differentiated tumor component in the given needle core biopsy examined.
The key element that helped in the accurate histopathological recognition of this being a primary hepatocellular carcinoma was the status of the surrounding liver on examination of the additional liver core biopsies. As seen in Figure 4c these cores showed the presence of a densely fibrotic/cirrhotic background of the liver parenchyma, with trichrome stain highlighting the moderate to severe fibrosis, associated with atypical neoplastic hepatocytes in 3-4 cell layer thickness forming pseudo glands (Figure 4a) with reticulin loss (Figure 4b) and the typical sinusoidal capillarization highlighted by CD34 staining (Figure 4d) representing a moderately well differentiated hepatocellular carcinoma. These neoplastic cells retained their HepPar-1 staining (Figure 4e) with no aberrant expression of CK7 or CK20 (Figure 4f). Hence, in this context, the poorly differentiated component with aberrant IHC staining patterns represents tumor heterogeneity of the same tumor. This was also supported with the integration of complete clinical (long standing history of chronic hepatitis C) associated with endoscopic and radiological data of a completely negative gastrointestinal investigative workup.
Though the commonest cause for multiple solid liver lesions in an adult is metastatic disease, it is important to remember multifocal HCC as a differential diagnosis especially if the surrounding liver is cirrhotic. Though for the past 70 years or so, it has been observed that, metastases commonly does not occur in a cirrhotic liver, this has been confirmed in 2014 in a meta-analysis study of 10,349 colorectal cancer patients in whom, patients with chronically diseased livers have a significantly lower incidence of colorectal liver metastases than those with normal livers [17]. The exact cause for this phenomenon is not clearly understood though the presence of the dense fibrosis resulting due to matrix metalloproteinases [MMPs] and their tissue inhibitors (TIMPs) with matrix degradation and remodeling is said to be a key factor. In this study, cirrhotic livers due to hepatitis virus infection also showed reduced to nil liver metastases which is postulated to be related to virus replication that promotes immune cells to secrete tumor necrosis factor that kill metastatic cancer cells. Correspondingly, the virus replication is said to be involved in DNA methyltransferases with overexpression and dysregulation of polycomb- repressive- complex (PRC2) that results in epigenetic silencing of tumor suppressor genes thus promoting intrinsic liver carcinogenesis-i.e. hepatocellular carcinoma.
Conclusion with Learning Points
In summary, this case report highlights the following learning points in the diagnostic interpretation of needle core biopsy of multiple solid liver lesions in adults. 1) Diffuse CK20 positivity with HepPar-1 negativity in a poorly differentiated neoplasm in the liver does not rule out HCC and does not rule in colorectal metastases. 2) Evaluation of the surrounding ‘non-neoplastic’ liver parenchyma is important to determine whether it is a ‘virgin’ non diseased liver or ‘non-virgin’ diseased liver. 3) In the presence of ‘non-virgin’ diseased liver and / or cirrhosis, the working diagnostic rule is that the occurrence of colorectal metastases is one of low probability. 4) It is therefore recommended, that in addition to needle core biopsy of the mass lesion, the surrounding liver should also be sampled to a) evaluate native liver disease status and b) for increased tumor sampling to accommodate tumor heterogeneity with adequate representations of both poorly and moderately well- differentiated components.
5) Limited diagnostic material in a liver biopsy compounded by aberrant IHC staining patterns can be a diagnostic pitfall for accurate histopathological identification of the underlying lesion. 6) Last, but not the least, clinicopathological correlation with complete systematic integration of clinical, biochemical, endoscopic and radiological data are essential for accurate pathological interpretation of needle core biopsies of solid liver mass lesions in adults by enforcing the underlying caveat of “never diagnose liver biopsies in ‘pathological isolation’.
References
-
Fanni D, Nemolato S, Ganga R, Senes G, Gerosa C, et al. (2009) Cytokeratin 20-positive hepatocellular carcino- ma. European Journal of Histochemistry 53(4): 269-274.
-
Barakauskienė A, Šumkauskaitė M (2008) Immunohis- tochemical approach to hepatocellularcarcinoma (HCC). Acta Medica Lituanica 15(2): 88-94.
-
Bellizzi MA (2020) An Algorithmic Immunohistochemical Approach to Define Tumor Type and Assign Site of Origin. Adv Anat Pathol 27(3): 114-163.
-
International Working Party (1995) Terminology of Hepatocellular Lesions. Hepatolog 22(3): 983-993.
-
Mourra N, Azizi L (2013) CK20 Positivity in Hepatocellular Carcinoma: A Potential Diagnostic Pitfall in Liver Biopsy. Applied Immunohistochemistry & Molecular Morphology 21(1): 94-95.
-
Karabork A, Kaygusuz G, Ekinci C (2010) The best immunohistochemical panel for differentiating hepatocellular carcinoma from metastatic adenocarcinoma. Pathology Research and Practice 206(8): 572-577.
-
Wang NP, Zee S, Zarbo R, Carlos B, Allen G, et al. (1995) Coordinate Expression of Cytokeratin 7 and 20 Defines Unique Subsets of Carcinomas. Applied Immunohistochemistry 3(2): 99-107.
-
Rullier A, Le Bail B, Fawaz R, Blanc JF, Saric J, et al. (2000) Cytokeratin7 and 20 expression in Cholangiocarcinoma Varies Along Biliary Tract But Still Differs From That In Colorectal Metastasis. American Journal of Surgical Pathology 24(6): 870-876.
-
El Jabbour T, Durie N, Lee H (2018) Coexpression of CDX2 and CK20 in hepatocellular carcinoma, an exceedingly rare co-incidence with potential diagnostic pitfall, Human Pathology 81: 298-302.
-
Shah SS, Wu TT, Torbenson MS, Chandan VS (2017) Aberrant CDX2 Expression in Hepatocellular Carcinomas: An Important Diagnostic Pitfall. Human Pathology 64: 13-18.
-
Nguyen T, Phillips D, Jain D, Torbenson M, Wu TT, et al. (2015) Comparison of 5 Immunohistochemical Markers of Hepatocellular Differentiation for the Diagnosis of Hepatocellular Carcinoma. Arch Pathol Lab Med 139: 1028-1034.
-
Botta MC, Ambu R, Liguori C, Van Eyken P, Pisanu A, et al. (2000) CK20 Expression in the Gastrointestinal Tract of the Embryo and Fetus. Pathologica 93(6): 640-644.
-
Miettnen M (1995) Keratin 20: Immunohistochemical Marker for Gastrointestinal, Urothelial and Merkel Cell carcinomas. Modern Pathology 8(4): 384-388.
-
Southgate J, Harnden P, Trejdosiewicz LK (1999) Cytokeratin expression patterns in normal and malignant urothelium: a review of the biological and diagnostic implications. Histol Histopathology 14: 657-664.
-
Porcell AI, De Young BR, Proca DM, Frankel WL (2000) Immunohistochemical Analysis of Hepatocellular and Adenocarcinoma in the Liver: MOC31 Compares Favorably with Other Putative Markers. Modern Pathology 13(7): 773-778.
-
Faa G, Van Eyken P, Roskams T, Miyazakiet H, Serreli S, et al. (1998) Expression of cytokeratin 20 in developing rat liver and experimental models of ductular and oval cell proliferation. Journal of Hepatology 29: 628-633.
-
Cai B, Liao K, Song XQ, Wei WY, Zhuang Y, et al. (2014) Patients with Chronically Diseased Livers Have Lower Incidence of Colorectal Liver Metastases: A Meta- Analysis. PLoS One 29: 9(9).
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient