COVID-19-Associated Liver Injury Is a Key Determinant of Patient's Survival in a Low Endemicity Area from Central Italy
1.1. Background: Liver injury (LI) occurring in patients with COVID-19 has been reported, yet its prognostic significance remains unexplored. 1.2. Aim: To investigate whether the onset, type and severity of virus-associated LI predicts the clinical outcomes of the disease 1.3. Methods: All consecutive patients with COVID-19 admitted to the Infectious Disease Unit of the University Hospital of Rome “Tor Vergata†from February to May 2020, were enrolled. LI was defined as the presence of an elevation of aminotransferases, gamma-glutamyl transferase or alkaline phosphatase greater than 1.5 times above the upper limit of normality (ULN), and/or a total bilirubin greater than 2.0 mg/dl. Death was considered as the primary endpoint. 1.4. Results: Among 151 hospitalized patients (mean age, 64 ± 18 years; 62.9% males) 41 (27.1%) died. LI was found in 57.6% of cases and in 23.8% was already present at admission. LI was associated with older age (p=0.006), longer hospital stay (p
Introduction
SARS-CoV-2 was recently identified as a novel highly contagious and pathogenic coronavirus causing severe pneumonia. Since December 2019, the viral infection rapidly spread over the world, with more than 12 million of infected cases and over 560,000 related deaths reported to date [1]. The coronavirus disease 2019 (COVID-19) primarily involves the lungs, causing typical respiratory symptoms and signs. However, gastrointestinal symptoms and liver injury (LI) also occur during the course of the disease. Diarrhea has been reported as the most common digestive symptom, more often occurring within the first week of illness [2], and many COVID-19 patients presented abnormal liver enzymes, a feature possibly related to the disease severity [1]. The mechanisms of gastrointestinal and liver involvement by SARS-CoV-2 likely imply a primary role of angiotensin- converting enzyme 2 (ACE2) cell entry receptors, which are used by the virus to infect different epithelial cells. ACE2 receptors are in fact widely expressed in human small intestinal enterocytes [4], as in bile duct epithelial cells, but not in liver cells [5, 6]. This suggests that ACE2 receptors are not directly involved in the development of SARS-CoV- 2-induced hepatic damage, which rather may conceivably be the result of a systemic cytokine-mediated inflammatory response.
Since March 2019, several hospital-based studies have reported the clinical characteristics of patients with COVID-19, showing different patterns of liver abnormalities, with predominant hepatocellular, cholestatic or mixed damage [7, 8, 9, 10, 11, 12]. Additionally, post-mortem pathological analyses performed in patients died from COVID-19 showed the presence of hepatocyte degeneration associated with lobular focal necrosis and neutrophil infiltration, as well as lymphocytes and monocytes infiltration in portal tracts and congestion of hepatic sinusoids, with evidence of micro- thrombosis [13, 14]. Yet, histological features of liver failure or bile duct injury have not been observed in deceased cases. In a recent study from China [15], 41% of patients with COVID-19 showed abnormal liver tests at hospital admission and 5% had liver injury, based on liver enzyme abnormalities. Patients with abnormal liver tests were older, had a higher body mass index (BMI) and were more often males and had a greater risk of developing severe COVID-19 compared to those with normal liver function. A recent Italian meta- analysis [16], including 11 observational studies with more than 2000 patients with COVID-19, reported a relatively low prevalence (3%) of chronic liver disease at baseline in patients. However, patients with severe forms of COVID-19 developed more frequently abnormalities of liver enzymes and changes in the coagulative and fibrinolytic profiles. While the clinical characteristics of LI occurring in patients with COVID-19 have been extensively reported, little attention has been given so far to the prognostic significance of COVID-19- associated LI, which therefore remains largely unexplored. It is also unclear whether LI presents with the same features in geographic areas with different rates of disease endemicity.
In this study of a cohort of SARS-CoV-2-infected patients consecutively admitted to a COVID hospital located in an area of central Italy with a cumulative incidence of 138,51 cases per 100.000 citizens [17], we aimed to investigate to what extent the onset, type and severity of virus-associated LI predicted the clinical outcomes of the disease.
Patients and Methods
This is a single-center, observational study evaluating the prevalence and the possible clinical impact of LI in patients with COVID-19 admitted to the Clinical Infectious Disease Unit of the Tor Vergata University Hospital in Rome, Italy. Patients’ clinical features and laboratory tests were prospectively collected in a dedicated dataset. In particular, serology for hepatitis B and C viruses were evaluated in all patients at entry. All therapeutic regimens were reported and analysed. Liver injury was defined as the presence of aspartate amino-transferase (AST), alanine amino- transferase (ALT), gamma-glutamyl transferase (GGT), or alkaline phosphatase greater than 1.5 times the upper limit of normal values (ULN) (34 U/l, 55 U/l, 50 U/l and 150 U/l, respectively), or by the presence of total bilirubin greater than 2.0 mg/dl. LI was assessed both at hospital admission as well as if developed during the hospital stay and was classified as cytolytic, cholestatic or mixed type depending on the predominantly observed liver abnormality. Severe LI was defined by the presence of any serum liver test greater than 3 times above ULN.
The aim of the study was to assess whether LI predicts the clinical outcomes, considering death as the primary endpoint.
The study was conducted in compliance with the 1975 Declaration of Helsinki and was approved by our local Ethics Committee. (se disponibile mettere il numero dell’approvazione)
Statistical analysis
Chi-square with Mantel-Haenszel correction or Fisher- exact test were performed to compare categorical variables. A Kolmogorov-Smirnov test for normality was preliminarily executed to define the distribution of each continuous variable; a t-Student test was then performed for normally distributed variables and a Mann-Whitney U non-parametric test for non-normally distributed variables. A backward stepwise multivariable regression model was used to assess the association between all recorded patients’ features and death. Survival was estimated using Kaplan-Meier curves and analysed by the log-rank test. A Cox regression analysis was performed to define the independent predictors of death recorded at time of hospitalization. Statistical significance was defined by a p value <0.05 in a “two-tailed” test, with a 95% confidence interval. Statistical analyses were performed using the IBM Statistical Program for Social Sciences (SPSS®) version 20.0 for Windows® (IBM Corp, Armonk, NY, USA).
Results
Prevalence and Severity of Liver Injury and Associated Factors
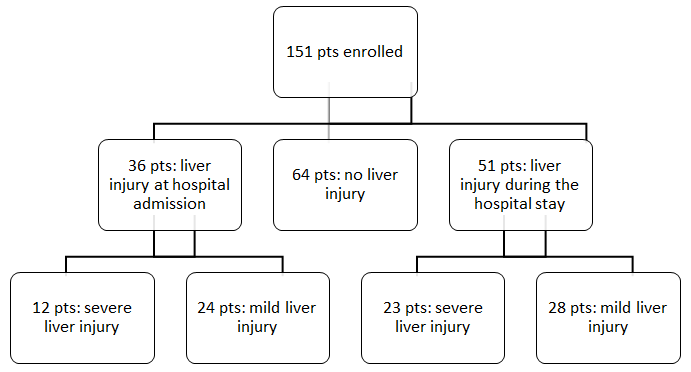
A total of 151 patients with COVID-19 were enrolled from February 27, 2020 to May 4, 2020 (Figure 1). As shown in Table 1, mean age was 64 ± 18 years with a prevalence of male gender (62.9%). The most frequent comorbidities were cardiovascular diseases (51.0%), pulmonary diseases (24.5%) and diabetes (23.2%). Six patients were HCV- antibody positive and 2 of these had evidence of viral replication. No replicating HBV infections were observed. A total of 41 patients died during the observation period.
| Total | Liver Injury | No Liver Injury | P value | O.R. | |
|---|---|---|---|---|---|
| (151 pts) | (87 pts) | (64 pts) | |||
| Age (years) | 64 ± 18 | 68 ± 16 | 60 ± 20 | 0.006 | n.a. |
| Male Sex (%) | 95 (62.9) | 59 (67.8) | 36 (56.3) | 0.146 | |
| Hospital stay (days) | 20 ± 16 | 24 ± 17 | 14 ± 13 | <0.0001 | n.a. |
| ICU stay (%) | 23 (15.2) | 20 (23.0) | 3 (4.7) | 0.002 | 6.07 |
| ICU stay (days) | 8 ± 6 | 8 ± 6 | 12 ± 5 | 0.279 | |
| Death (%) | 41 (27.2) | 32 (36.8) | 9 (14.1) | 0.002 | 3.556 |
| Obesity (%) | 27 (17.9) | 21 (24.1) | 6 (9.4) | 0.019 | 3.076 |
| Diabetes (%) | 35 (23.2) | 23 (26.4) | 12 (18.8) | 0.269 | |
| Cardiovascular disease (%) | 77 (51.0) | 51 (58.6) | 26 (40.6) | 0.029 | 2.071 |
| Liver disease (%) | 2 (1.3) | 1 (1.1) | 1 (1.6) | 0.826 | |
| Pulmonary disease (%) | 37 (24.5) | 25 (28.7) | 12 (18.8) | 0.159 | |
| Chronic Kidney disease (%) | 14 (9.3) | 8 (9.2) | 6 (9.4) | 0.97 | |
| Cytopathic LI (%) | 47 (31.1) | 47 (54.0) | - | ||
| Cholestatic LI (%) | 8 (5.3) | 8 (9.2) | - | ||
| Mixed LI (%) | 32 (21.2) | 32 (36.8) | - | ||
| Mild LI (%) | 43 (28.5) | 43 (49.4) | - | ||
| Severe LI (%) | 44 (29.1) | 44 (50.6) | - | ||
| LI at hospital admission (%) | 36 (23.8) | 36 (41.4) | - | ||
| Cytopathic LI (%) | 22 (14.6) | 22 (25.3) | - | ||
| Cholestatic LI (%) | 4 (2.6) | 4 (4.6) | - | ||
| Mixed LI (%) | 10 (6.6) | 10 (11.5) | - | ||
| Mild LI (%) | 24 (15.9) | 24 (27.6) | - | ||
| Severe LI (%) | 12 (7.9) | 12 (13.8) | - | ||
| HCV-ab positive (%) | 6 (4.0) | 4 (4.6) | 2 (3.1) | 0.672 | |
| HCV-RNA positive (%) | 2 (33.3) | 1 (1.1) | 1 (1.6) | 0.807 | |
| HBsAg (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | |
| HBcAb (%) | 25 (16.6) | 19 (21.8) | 6 (9.4) | 0.064 | |
| HBsAb (%) | 34 (22.5) | 21 (24.1) | 13 (20.3) | 0.71 | |
| Lopinavir/Ritonavir (%) | 112 (74.2) | 67 (77.0) | 45 (70.3) | 0.353 | |
| Hydroxychloroquine (%) | 126 (83.4) | 77 (88.5) | 49 (76.6) | 0.051 | |
| Corticosteroids (%) | 45 (29.8) | 31 (35.6) | 14 (21.9) | 0.068 | |
| Darunavir/Ritonavir (%) | 28 (18.5) | 18 (20.7) | 10 (15.6) | 0.429 | |
| Tocilizumab (%) | 27 (17.9) | 20 (23.0) | 7 (10.9) | 0.056 |
Table 1: Association between liver injury and patients’ features. All continuous variables are expressed as Mean ± Standard Devia
Table 1: Association between liver injury and patients’ features. All continuous variables are expressed as Mean ± Standard Deviation. Abbreviations: pts= patients; n.a. = not applicable; ICU= Intensive Care Unit; AST: aspartate amino-transferase; ALT: alanine amino-transferase; GGT: gamma-glutamyl transferase; ALP: alkaline phosphatase; LI: liver injury.
LI was found in 87 patients (57.6%) and in 36 (23.8 %) of these was already present at hospital admission. LI was cytolytic in 47 patients (31.1 %), cholestatic in 8 patients (5.3%) and mixed type in 32 patients (21.2%), respectively. Severe LI was observed in 44 patients (29.1 %), in 12 of whom (27.2%) was already present at hospital admission. The mean hospital stay was significantly longer in patients with than without LI (24 ± 17 vs 14 ± 13 days, respectively, p<0.0001). At univariate analysis, the following variables were found to be associated with LI: older age (68 ± 16 vs 60 ± 20 years; p=0.006); ICU stay (23.0% vs 4.7%; p=0.002); obesity (24.1% vs 9.4%; p=0.019) and cardiovascular diseases (58.6% vs 40.6; p=0.029).
A further sub-analysis was performed to define the characteristics of patients who developed severe LI. These patients presented more frequently with a mixed type of LI (p=0.034) and more often were treated with tocilizumab and corticosteroids (p=0.006 and p=0.023, respectively), compared to those who did not show LI, or had only mild LI.
Liver Injury as Predictor of Death
Table 2 reports the characteristics of patients who died at univariate analysis. These patients were older (78 ± 13 vs 59 ± 17 years; p<0.0001), more frequently admitted to ICU (39.0% vs 6.4%; p<0.0001) and almost all had comorbidities (40/41 patients; p<0.0001). LI was found in 32 patients who died (78.0%) compared to 55 (50.0%) who survived (p=0.002). Patients who died showed higher levels of AST (67 ± 75 vs 35 ± 17 U/l; p<0.0001), total bilirubin (0.91 ± 0.49 vs 0.69 ± 0.22 mg/dl; p=0.036), GGT (61 ± 71 vs 47 ± 59 U/l; p=0.041) and alkaline phosphatase (92 ± 47 vs 66 ± 27 U/l; p<0.0001) than patients who survived.
| Death (41 pts) | Healed (110 pts) | P value | O.R. | |
|---|---|---|---|---|
| Age | 78 ± 13 | 59 ± 17 | <0.0001 | n.a |
| Male Sex (%) | 25 (61.0) | 70 (63.6) | 0.763 | |
| Hospital stay (days) | 17 ± 16 | 21 ± 16 | 0.044 | n.a |
| ICU stay (%) | 16 (39.0) | 7 (6.4) | <0.0001 | 9.147 |
| ICU stay (days) | 7 ± 6 | 11 ± 5 | 0.076 | |
| Comorbidities (%) | 40 (97.6) | 63 (57.3) | <0.0001 | 29.841 |
| Obesity (%) | 9 (22.0) | 18 (16.4) | 0.426 | |
| Diabetes (%) | 18 (43.9) | 17 (15.5) | <0.0001 | 4.281 |
| Cardiovascular disease (%) | 33 (80.5) | 44 (40.0) | <0.0001 | 6.188 |
| Liver disease (%) | 0 (0.0) | 2 (1.8) | 0.945 | |
| Pulmonary disease (%) | 17 (41.5) | 20 (18.2) | 0.003 | 3.188 |
| Chronic Kidney disease (%) | 9 (22.0) | 5 (4.5) | 0.001 | 5.906 |
| Liver injury (%) | 32 (78.0) | 55 (50.0) | 0.002 | 3.556 |
| AST | 67 ± 75 | 35 ± 17 | <0.0001 | n.a |
| ALT | 40 ± 43 | 52 ± 49 | 0.052 | |
| Albumin | 2.83 ± 0.36 | 3.65 ± 0.49 | <0.0001 | n.a |
| Total Bilirubin | 0.91 ± 0.49 | 0.69 ± 0.22 | 0.036 | n.a |
| GGT | 61 ± 71 | 47 ± 59 | 0.041 | n.a |
| ALP | 92 ± 47 | 66 ± 27 | <0.0001 | n.a |
| Mild LI (%) | 13 (31.7) | 29 (26.4) | 0.516 | |
| Severe LI (%) | 14 (34.1) | 23 (20.9) | 0.096 | |
| LI at hospital admission (%) | 15 (36.6) | 21 (19.1) | 0.025 | 2.445 |
Table 2: Factors associated with death at univariate analysis. All continuous variables are expressed as Mean ± Standard Deviatio
Table 2: Factors associated with death at univariate analysis. All continuous variables are expressed as Mean ± Standard Deviation. Abbreviations: pts= patients; n.a. = not applicable; ICU= Intensive Care Unit; AST: aspartate amino-transferase; ALT: alanine amino-transferase; GGT: gamma-glutamyl transferase; ALP: alkaline phosphatase; LI: liver injury.
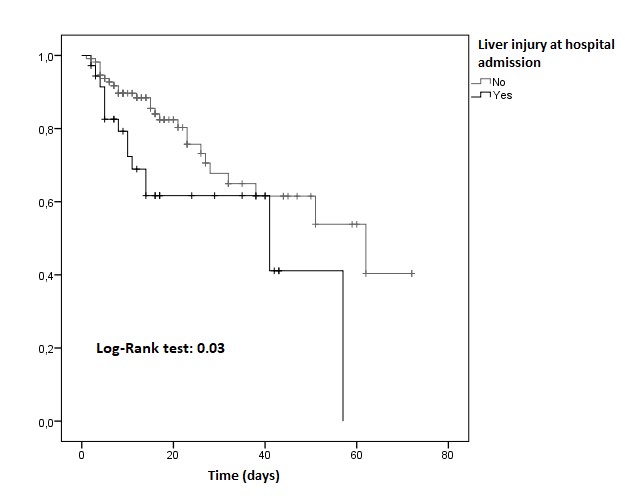
In contrast, ALT values were lower in patients who died than in survivors, but the difference did not achieve statistical significance (40 ± 43 vs 52 ± 49 U/l; p=0.052). Albumin levels were lower in patients who died than patients who survived (2.86 ± 0.36 vs 3.65 ± 0.49 g/dl; p<0.0001). Even LI at admission was tightly related to a poor outcome, as it was observed in 36.6% of those who died compared to
19.1% of those who survived (p=0.025). Accordingly, the overall survival in patients with LI at hospital admission was significantly lower than in patients with normal liver function at entry (35 vs 49 days; p=0.030; Figure 2). Additional factors associated with death at univariate analysis are shown in supplementary Table 1.
| Death (41 pts) | Healed (110 pts) | P value | |
|---|---|---|---|
| Corticosteroids (%) | 23 (56.1) | 22 (20.0) | <0.0001 |
| Haemoglobin | 11.4 ± 1.9 | 12.6 ± 1.8 | 0.001 |
| WBC | 11325 ± 4270 | 6630 ± 1880 | <0.0001 |
| NEU | 9915 ± 4170 | 4485 ± 1845 | <0.0001 |
| LYM | 825 ± 385 | 1440 ± 575 | <0.0001 |
| Platelets | 212 ± 85 | 254 ± 80 | 0.003 |
| INR | 1.42 ± 0.69 | 1.15 ± 0.14 | <0.0001 |
| D-Dimer | 6095 ± 8836 | 1616 ± 2456 | <0.0001 |
| Glycaemia | 150 ± 53 | 110 ± 41 | <0.0001 |
| Creatinine | 2.25 ± 1.79 | 1.03 ± 0.99 | <0.0001 |
| LDH | 499 ± 234 | 260 ± 71 | <0.0001 |
| CRP | 106.5 ± 51.5 | 39.9 ± 39.8 | <0.0001 |
Supplementary Table 1: Additional factors associated with death at univariate analysis. All continuous variables are expressed as Mean ± standard deviation. Abbreviations: pts: patients; WBC: white blood cell; NEU: neutrophils; LYM: lymphocytes; INR: international normalised ratio; LDH: lactate dehydrogenase; CRP: C-reactive protein.
All variables found to be significantly associated with death at univariate analysis were entered in a multivariable analysis model with COVID-19 death as dependent variable. The following variables, expressed as means during the whole hospital stay, were found to be independently associated with a greater risk of death: low albumin (p<0.0001), low ALT (p=0.0002), high AST (p=0.0250), high LDH (p=0.0014), low platelets count (p=0.0056) and high white blood cell count (p=0.0001).
We also performed a further analysis to identify which laboratory test measured at time of hospital admission was associated with a greater probability of death. These included, at univariate analysis, low haemoglobin (p=0.001), high white blood cells count (p<0.0001), high INR (p=0.006), high D-Dimer (p=0.005), high serum creatinine (p<0.0001), high AST (p=0.032), high total bilirubin (p=0.013), high GGT (p=0.041), high alkaline phosphatase (p<0.0001), low serum albumin (p<0.0001), high LDH (p<0.0001) and high CRP (p<0.0001). All these variables were then entered in a Cox regression model, together with age, gender and the presence of individual comorbidities found to be associated with death in the previous analysis. Older age (H.R. 1.065, C.I. 95% 1.022-1.110; p=0.003), diabetes (H.R. 3.389, C.I. 95% 1.188-9.668; p=0.023), low serum albumin (H.R. 0.118, C.I. 95% 0.035-0.399; p=0.001), high AST (H.R. 1.007, C.I. 95% 1.000-1.013; p=0.035), high total bilirubin (H.R. 9.199, C.I. 95% 2.396-35.314; p=0.001), high GGT (H.R. 1.032, C.I. 95% 1.016-1.048; p<0.0001) and low alkaline phosphatase (H.R. 0.968, C.I. 95% 0.952-0.985; p<0.0001) were identified as independent predictive factors of death in SARS-CoV-2 infected patients (Tables 3 & 4).
| Standardized Coefficient | P value | |
|---|---|---|
| Albumin | -0.2967 | <0.0001 |
| ALT | -0.2390 | 0.0002 |
| AST | 0.1907 | 0.0250 |
| LDH | 0.2757 | 0.0014 |
| Platelets | -0.1495 | 0.0056 |
| White Blood Cells Count | 0.2833 | 0.0001 |
Table 4: Factors associated with death at multivariable analysis. Abbreviations: ALT: Alanine amino-transferase; AST: Aspartate a
| Death (41 pts) | Healed (110 pts) | P value | |
|---|---|---|---|
| Corticosteroids (%) | 23 (56.1) | 22 (20.0) | <0.0001 |
| Haemoglobin | 11.4 ± 1.9 | 12.6 ± 1.8 | 0.001 |
| WBC | 11325 ± 4270 | 6630 ± 1880 | <0.0001 |
| NEU | 9915 ± 4170 | 4485 ± 1845 | <0.0001 |
| LYM | 825 ± 385 | 1440 ± 575 | <0.0001 |
| Platelets | 212 ± 85 | 254 ± 80 | 0.003 |
| INR | 1.42 ± 0.69 | 1.15 ± 0.14 | <0.0001 |
| D-Dimer | 6095 ± 8836 | 1616 ± 2456 | <0.0001 |
| Glycaemia | 150 ± 53 | 110 ± 41 | <0.0001 |
| Creatinine | 2.25 ± 1.79 | 1.03 ± 0.99 | <0.0001 |
| LDH | 499 ± 234 | 260 ± 71 | <0.0001 |
| CRP | 106.5 ± 51.5 | 39.9 ± 39.8 | <0.0001 |
Table 5: Independent predictive factors of death at hospital admission. All continuous variables are expressed as Mean ± Standard
Table 4: Independent predictive factors of death at hospital admission. All continuous variables are expressed as Mean ± Standard Deviation. Abbreviations: WBC: white blood cell; NEU: neutrophils; LYM: lymphocytes; INR: international normalised ratio; AST: aspartate amino-transferase; ALT: alanine amino-transferase; GGT: gamma-glutamyl transferase; ALP: alkaline phosphatase; LDH: lactate dehydrogenase; CRP: C-reactive protein.
Discussion
Development of LI has been already described in earlier reports on COVID-19 patients. Our study provides further evidences that LI is a very frequent event in this setting, as it was found in 57% of SARS-CoV-2-infected patients in our cohort. Comparison of the prevalence rates of LI with the current literature is, however, difficult due to the variable definitions of LI adopted in different studies [15, 18, 19]. In the present study we aimed to address for the first time whether emergence of LI is related to the outcome of COVID-19, specifically looking at the time of onset of LI, its predominant type and its severity. We found, at multivariable analysis, that LI was an independent predictor of poor outcome, as patients who developed LI had a significantly lower survival compared to those who maintained normal liver tests during the hospital stay. Interestingly, 23.8% of the whole cohort of patients already presented with LI at hospital admission and this subgroup of patients had the highest probability of death compared to all other patients. Thus, LI is an early event during the course of the disease and its prompt detection upon entering the hospital, may help identifying patients with a poorer prognosis.
The origin of LI in patients with COVID-19 is currently unknown, yet it is most likely to be multifactorial. LI might in fact be the results of direct viral infection of liver epithelial cells, or follow a strong systemic inflammatory response, or be due to pneumonia-associated hypoxia. In addition, LI may be induced by sepsis-related metabolic acidosis and/or antiviral drug toxicity. Many of these putative mechanisms may indeed coexist and together conceivably trigger an ischemic/hypoxic pathway leading to liver damage, as the likely predominant cause. This interpretation is supported by our finding that an increase of AST and of LDH, observed either at or during hospitalization, but not an increase of ALT, was significantly associated with a greater risk of death, as already observed by Lei Fang et al.20 The possibility of a predominant ischemic/hypoxic nature of LI in COVID-19 is also consistent with the known ability of the virus to cause diffuse micro-thrombosis, associated with high D-Dimer values, as also found in our study in patients with worse outcomes. On the other hand, the possibility of a direct virus- related cytopathic damage appears less likely, also considering that none of the patients with LI died of acute liver failure or presented a clinically significant liver disease. Accordingly, liver biopsies were not performed to further investigate the nature of LI, as there was no clinical justification to perform invasive examinations. However, in our study LI appeared to present in most cases with a cytolytic or mixed biochemical pattern, and only rarely with a predominantly cholestatic type. This finding differs from what reported in a cohort of Asian patients, where a predominantly cholestatic type of LI was described15, suggesting that SARS-CoV-2-related liver pathogenicity might reflect different host-virus interactions, or even patient-related genetic variability.
Our study has limitations. Our cohort is relatively small, yet has the advantage to origin from a single academic center and to include a series of consecutive patients, with a negligible number of missing data. Our facility is a university hospital located in central Italy, where the incidence of COVID-19 has been considerably lower compared to other Italian regions, such as Lombardy or other areas from other countries in which COVID-19 incidence was significantly higher.
Conclusion
LI is as an inherent finding in COVID-19, despite its development is unlikely to be clinically relevant, nor associated with liver failure. Yet, its early emergence represents an unfavorable prognostic marker of the disease and prompt detection is therefore advisable to better identify patients at greater risk of death.
Conflicts of Interest: All Authors have no conflict of interest Funding: No Authors received any financial support for the manuscript
References
-
European Centre for Disease Prevention and Control (ECDC) (2020) COVID-19 situation update worldwide.
-
Guan WJ, Zheng yi Ni, Yu Hu, Wen-hua L, Chun-quan O, et al. (2020) Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med 382(18): 1708-1720.
-
Zhang C, Lei S, Fu-Sheng W (2020) Liver injury in COVID-19: management and challenges. Lancet Gastroenterol Hepatol 5(5): 428-430.
-
Zhanga H, Hong-Bao Li, Jian-Rui L, Xiao-Ming L, Wei L, et al. (2020) Specific ACE2 expression in small intestinal enterocytes may cause gastrointestinal symptoms and injury after 2019-CoV Infection. International Journal of Infectious Diseases 96 (2020): 19-24.
-
Chai X, Longfei H, Yan Z, Weiyu H, Zhou L, et al. (2020) Specific ACE2 expression in cholangiocytes may cause liver damage after 2019-nCoV infection. bio-Rxiv.
-
Liu M, Ting W, Yun Z, Yutong Z, Yutong Z, et al. (2020) Potential Role of ACE2 in Coronavirus Disease 2019 (COVID-19) Prevention and Management. J Transl Int Med 8(1): 9-19.
-
Chen N, Min Z, Min Z, Xuan D, Jieming Q, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395: 507-513.
-
Huang C, Yeming W, Xingwang Li, Lili R, Jianping Z (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
Tian S, Nan H, ing L, Kun C, Xuqin K, et al. (2020) Characteristics of COVID-19 infection in Beijing. J Infect 80: 401-406.
-
Yang W, Qiqi C, Le Q, Xiaoyang W, Zenghui C, et al. (2020) Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): a multi- center study in Wenzhou city, Zhejiang, China. J Infect 80: 388-393.
-
Zhang JJ, Xiang D, Yi-Yuan C, Ya-Dong Y, Yi-Bin Y, et al. (2020) Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 75(7): 1730- 1741.
-
Wang D, Bo H, Chang H, Fangfang Z, Xing L, et al. (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 323: 1061-1069.
-
Xu Z, Lei S, Yijin W, Jiyuan Z, Lei H, et al. (2020) Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med 8(4): S2213-2600.
-
Liu Q (2020) General anatomy report of novel coronavirus pneumonia patients. Journal of Forensic Medicine 36: 21-23.
-
Cai Q, Deliang H, Hong Y, Jun C, Lei L, et al. (2020) COVID-19: Abnormal liver function tests. J Hepatol 8278(20).
-
Mantovani A, Giorgia B, Andrea D (2020) Coronavirus disease 2019 and prevalence of chronic liver disease: A meta-analysis. Liver Int 40(6): 1316-1320.
-
Jothimani D, Radhika V, Mohammed FA, Ilankumaran K, Mohamed R, et al. (2020) Covid-19 and liver. J Hepatol S0168-8278(20): 30377-30379.
-
Fan Z, Liping C, Jun L, Xin C, Jingmao Y, et al. (2020) Clinical Features of COVID-19-Related Liver Functional Abnormality. Clin Gastroenterol Hepatol 18(7): 1561- 1566.
-
Fang L, Ye-Mao L, Feng Z, Juan-Juan Q, Peng Z, et al. (2020) Longitudinal association between markers of liver injury and mortality in COVID-19 in China. Hepatology 72(2): 389-398.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient