Xanthogranulomatous Cholecystitis Surgical Dilemma and Difficulty
Xanthogranulomatous Cholecystitis (XGC) is difficult to diagnose by surgeons preoperatively. XGC is often mistaken for, and may predispose to, gallbladder carcinoma (GBC). Most of the patients present with features of chronic cholecystitis and pain. Radiological features can be helpful for assuming XGC but cannot rule out any other pathology. Cholecystectomy is encouraged to be performed as soon as the diagnosis of XGC is established to prevent the occurrence of complications. However laparoscopic cholecystectomy may not be feasible in all patients and conversion to open or subtotal cholecystectomy is done. XGC can only be confirmed by histological findings, thus always causing a surgical dilemma and difficulty for the surgeon.
Ankush Sarwal
Introduction
Xanthogranulomatous cholecystitis (XGC) is an uncommon, focal or diffuse destructive inflammatory disease of the gallbladder characterized by macrophage and foamy cell infiltration and diffuse fibrosis in the gallbladder (GB) wall. Inflammatory reaction and fibrosis cause asymmetric wall thickening in the GB wall and multiple yellowish brown- coloured intramural nodules [1]. Although it is considered as benign disease but in literature there have been reports of its close association with gallbladder cancer (GBC) [2]. The nomenclature was done by McCoy et al in 1976 though it was first described in 1970 by Christensen, et al. [3]. It is clinically seen as acute or chronic cholecystitis. It is difficult to diagnose by surgeons and radiologists in pre-operative and intra-operative setting as clinical signs and symptoms are similar to acute and chronic cholecystitis. Cholelithiasis and choledocholithiasis are frequently associated with XGC [4]. The gold standard treatment for cholelithiasis and cholecystitis is laparoscopic cholecystectomy. In XGC, surgery is often difficult due to intense fibrosis and adhesions to neighbouring organs [5].
Clinical Features
Male preponderance has been reported with a male to female ratio of 2:1 [5]. Incidence of XGC has been reported to be higher in the sixth and seventh decades of life. However, it can occur at any age and its occurrence in a two-month-old infant has also been described in literature [6]. Most of the patients present with features of chronic cholecystitis and pain. Around two fifth of the patient have features of acute cholecystitis or obstructive jaundice. Palpable lump is seen in 5% and cholangitis in 2% of cases of XGC [5]. On abdominal examination, positive Murphy’s sign can be localised in most of the cases. Even with these features it is a challenge for the clinician to diagnose as these clinical features are not specific for XGC and often no clinical difference between patients with XGC and GBC can be found [7]. Raised white blood cell counts and deranged liver function functions are a common biochemical investigation however these are not specific for diagnosis of XGC. Yu, et al. evaluated tumor biomarkers which included serum CA 19-9, carcinoembryonic antigen (CEA), and CA 12-5 in patients with XGC. Elevation of tumour markers is frequent in XGC which further creates confusion in differentiating the disease with GBC [8]. Therefore, tumour markers are often misleading in such cases.
Radiological Assessment
Radiology is an important aspect of pre-operative assessment of patients of XGC. In study done by Guzmaan- Valdivia, et al. [5] on XGC patients there was radiologic suspicion of GBC in 12% of the cases, but this was corroborated in only 2% of patient’s.
Ultrasonography
The sonographic findings in XGC include the presence of gallstones or sludge and moderate to marked focal or diffuse thickening of the gallbladder wall. Parra et al in study done on 26 patients observed that the GB wall was hyperechoic in comparison with the liver in all patients. Presence of hypoechoic nodules or bands in the thickened wall can occasionally be seen, the presence of which is considered a characteristic finding [9].
Computed Tomography (CT)
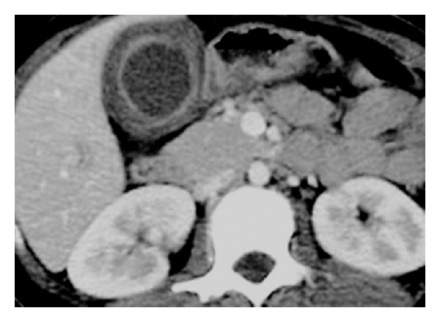
There are generally no definitive differences on CT between acute or chronic symptoms. Common features of XGC are increased gallbladder wall thickness (gallbladder wall thickening: >3 mm), extent of gallbladder wall thickness can be diffuse that’s is more than 50% involved gall bladder wall or focal that is less than 50% involved gall bladder wall. Gallbladder wall thickening can range from 4.0 mm to 18.5 mm and is usually diffuse in nature the presence of intramural hypo-attenuated nodules. The continuity of mucosal lines, the presence of luminal surface enhancement diffuse or focal wall thickening, intramural hypoattenuating nodules in thickened walls, luminal surface enhancement (LSE) with continuous mucosal lines or mucosal lines with focal breach (Figure 1).
Cholelithiasis and choledocholithiasis are often seen associated with XGC [10]. Occurrence of lymphadenopathy (> 10 mm in short axis diameter) has been seen from an incidence of 10.2 to 90 % in various studies [10, 11].
Magnetic Resonance Imaging (MRI)
On MRI, there can be variable nature of the intramural nodule. Intramural nodules consist of lymphocytes, foamy histiocytes, plasma cells, micro abscess, polymorphonuclear leucocytes, fibrosis and necrosis within them. Presence of these diverse contents leads to variability on MRI. CT has shown more sensitivity for intramural nodules than MRI [11]. The study done by Kang et al showed the benefit of diffusion-weighted magnetic resonance imaging (DWI) in differentiating XGC from the wall-thickening type of gallbladder cancer. Diffusion restriction was more frequently seen in gallbladder cancer (68%) than in XGC (7%). Kang et al showed addition of DWI to conventional MRI lead to better discrimination between XGC and the wall-thickening type of gallbladder cancer [12].
Surgical Features
Surgical treatment is recommended as the first line treatment of XGC. In the meta-analysis, which included 29 studies by Hale et al., the incidence of XGC was 1.3%- 1.9 with the exception of India where it was 8.8%. XGC if suspected preoperatively is most of the times a benign disease. Owing to the invasiveness and destruction of XGC, the cholecystectomy is encouraged to be performed as soon as the diagnosis of XGC is established to prevent the occurrence of complications, such as fistulas. XGC can have an aggressive presentation and extend into the adjacent structures, including liver, colon, and duodenum As we all know, laparoscopic surgery has already been widely applied because of its minimal invasiveness and rapid recovery from the procedure. In addition, laparoscopic cholecystectomy is a well-developed laparoscopic technique and has already been regarded as the golden standard in cholecystectomy. Thus, laparoscopic Cholecystectomy should be the first option for the surgical removal in these patients [13].
There is debate whether an extended Cholecystectomy should be tried first or simple cholecystectomy. Extended cholecystectomy avoids any chance of peritoneal spillage and maintains an oncological principle if the final Histopathological report comes out to be malignancy. However, doing laparoscopic cholecystectomy requires more expertise surgical skills and there are more chances of conversion to open cholecystectomy. In addition, the complications rate is more in extended as compared to open, causing more morbidity to the patient. This is still a matter of debate and no consensus is there. At operation, XGC may give the appearance of GBC due to the marked gallbladder thickening and local destructive spread of the inflammation. Hence, an intra-operative frozen-section biopsy is often recommended. On the other hand, the severe inflammation may mask the presence of a carcinoma [14, 15]. In reviewing the literature it is seen that around 8.8% receive an unnecessary extended operation for incorrectly suspected GBC and 1.3% who are treated with simple cholecystectomy only were post-operatively diagnosed with GBC [13, 16]. In Indian scenario, study done by Srinivas, et al. [17] had an laparoscopic attempt rate of 83%, but almost 50 % of these required conversion to open , while another study done by Srikanth, et al. [18] which had 60 patients of XGC , laparoscopic approach was attempted in 77% of patient with a conversion rate of 13 %.
One should be careful while doing XGC; violent dissection must be avoided to prevent possible injury of common bile duct. In the cases when the cystic gall duct is too thick to be sealed by LT 300, a bigger clip that is LT 400 should be applied. In case the callots anatomy is not defined well and there are high chances of common bile duct injury, a partial cholecystectomy should be carried out. If required the procedure can be carried out by harmonic scalpel or vessel sealer, which causes less bleeding and smoke. After the resection of the gall bladder, a careful inspection on any possible bleeding or leakage should be taking into account. Drainage is a significant prevention in bile leakage, which will cause no regrets. In many cases, XGC may coexist with choledocholithiasis. In such cases if ERCP is possible should be attempted first, otherwise for non-availability or failed ERCP, CBD exploration can be done. The postoperative complication rate of patients of XGC treated with partial cholecystectomy is around 10 % and around 3% in total cholecystectomy. The overall bile leak rate is around 5%. In addition, the length of stay in the hospital is generally longer in these patients as compared to cholecystectomy for other benign aetiologies. The average hospital stay has been reported to be 5 days for laparoscopic surgeries and around 10 days for open cholecystectomy [5, 9, 18].
Pathological Features
XGC was first described as a distinct pathological condition in 1981 by Goodman & Ishak [19]. XGC can only be confirmed by histological findings. Its pathogenesis is related to bile flow obstruction with infection and subsequent inflammation. Additionally, leading to leakage of bile to tissues, which enters into the stroma of the gallbladder wall through ruptured Rokitansky-Aschoff sinuses or mucosal ulcerations secondary to the presence of gallstones and/or acute inflammation? Subsequently, histiocytes accumulate and phagocytose the bile pigment, hemosiderin and cholesterol. Resulting in the formation of xanthoma cells [20]. Micro-abscesses form in the gallbladder wall eventually resulting in xanthogranulomatosis. Finally, a fibrous reaction and scarring result from healing of the inflammatory reaction.
Conclusion
XGC is a rare condition of acute or chronic inflammation of the gallbladder, associated with a high incidence of conversion to open cholecystectomy. Any radiological suspicion of XGC should make surgeron more careful during operative time. As there is no confirmatory test in preoperative evaluation to confirm XGC, there is always a surgical dilemma for the clinician.
References
-
Yang T, Zhang B, Zhang J, Zhang Y, Jiang X, et al. (2007) surgical treatment of xanthogranulomatous cholecystitis: Experience in 33 cases. Hepatobiliary Pancreat Dis Int 6(5): 504-508.
-
Ghosh M, Sakhuja P, Agarwal AK (2011) Xanthogranulomatous cholecystitis: a premalignant condition? Hepatobiliary Pancreat Dis Int 10(2): 79-184.
-
Christensen AH, Ishak KG (1970) Benign tumors and pseudotumors of the gallbladder: report of 180 cases. Arch Pathol 90(5): 423-432.
-
Qasaimeh GR, Matalqah I, Bakkar S, Al Omari A, Qasaimeh M (2015) Xanthogranulomatous cholecystitis in the laparoscopic era is still a challenging disease. J Gastrointest Surg 19(6): 1036-1042.
-
Guzmaan-Valdivia G (2004) Xanthogranulomatous cholecystitis:15 years’ experience. World J Surg 28(3): 254-257.
-
Kim SH, Kim HY, Jung SE, Park KW, Choi YH, et al. ((2013) Xanthogranulomatous cholecystits in 2-month-old infant. J Korean Surg Soc 85: 191-194.
-
Roberts KM, Parsons MA (1987) Xanthogranulomatous cholecystitis: clinicopathological study of 13 cases. J Clin Pathol 40: 412-417.
-
Yu H, Yu TN, Cai XJ (2013) Tumor biomarkers: help or mislead in the diagnosis of xanthogranulomatous cholecystitis?-analysis of serum CA 19-9, carcinoembryonic antigen, and CA 12-5. Chin Med J (Engl) 126(6): 3044-3047.
-
Parra JA, Acinas O, Bueno J, Güezmes A, Fernández MA, et al. (2001) Xanthogranulomatous cholecystitis: clinical, sonographic, and CT findings in 26 patients. AJR Am J Roentgenol 174: 979-983.
-
Zhao F, Lu PX, Yan SX, Wang GF, Yuan J, et al. (2013) CT and MR features of xanthogranulomatous cholecystitis: an analysis of consecutive 49 cases. Eur J Radiol 82(9): 1391-1397.
-
Goshima S, Chang S, Wang JH, Kanematsu M, Bae KT, et al. (2010) Xanthogranulomatous cholecystitis: diagnostic performance of CT to differentiate from gallbladder cancer. Eur J Radiol 74: e79-e83.
-
Kang TW, Kim SH, Park HJ, Lim S, Jang KM, et al. (2013) Differentiating xanthogranulomatous cholecystitis from wall-thickening type of gallbladder cancer: added value of diffusion-weighted MRI. Clin Radiol 68(10): 992-1001.
-
Hale MD, Roberts KJ, Hodson J, Scott N, Sheridan M, et al. (2014) Xanthogranulomatous cholecystitis: A European and global perspective. HPB (Oxford) 16: 448-458.
-
Houston JP, Collins MC, Cameron I, Reed MW, Parsons MA, et al. (1994) Xanthogranulomatous cholecystitis. Br J Surg 81: 1030-1032.
-
Benbow EW, Taylor PM (1988) Simultaneous xanthogranulomatous cholecystitis and primary adenocarcinoma of gallbladder. Histopathology 12: 672- 675.
-
Kwon AH, Sakaida N (2007) Simultaneous presence of Xanthogranulomatous cholecystitis and gallbladder cancer. J Gastroenterol 42: 703-704.
-
Srikanth G, Kumar A, Khare R, Lakshmaiah S, Archana G, et al. (2004) Should laparoscopic cholecystectomy be performed in patients with thick-walled gallbladder?. J Hepatobiliary Pancreat Surg 11(1): 40-44.
-
Srinivas GN, Sinha S, Ryley N, Houghton PW (2007) Perfidious gallbladders - a diagnostic dilemma with xanthogranulomatous cholecystitis. Ann R Coll Surg Engl 89(2): 168-172.
-
Goodman ZD, Ishak KG (1981) Xanthogranulomatous cholecystitis. Am J Surg Pathol 5: 653-659.
-
Mulchandani M, Nagori LF (2000) Xanthogranulomatous cholecystitis. Bombay Hospital Journal. 42(4): 31-32.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient