Tuberculosis in Patients Referred for Liver Transplant: A Case Series and Review of Literature
Pre transplant evaluation of a patient provides unique opportunity to diagnose certain diseases. Tuberculosis is endemic in India and patients are often diagnosed to have tuberculosis during their pre transplant evaluation. As these patients have advanced liver disease diagnosis, treatment planning for anti-tuberculosis therapy and timing the transplant is based on individual choice. There are no established guidelines from either the west or from India. We here report 5 cases of tuberculosis diagnosed as a part of pre transplant evaluation and have summarized available knowledge on managing such patients in peritransplant period.
Introduction
Tuberculosis in general is quite prevalent in developing countries with a belief that around 40-50% of population of Asia and Africa is infected with Mycobacterium Tuberculosis (TB) [1]. As per the Global TB report 2017 the estimated incidence of TB in India was approximately 28,00,000 accounting for about a quarter of the world’s TB cases [2]. Its frequency is increased 14-fold in patients with chronic liver diseases (CLD) and liver cirrhosis, more so in those with decompensated disease, probably due to the cirrhosis- associated immune dysfunction syndrome, and case-fatality rates are high. Tuberculosis in patients being evaluated for liver transplant presents a unique challenge. These patients cannot be transplanted with active tuberculosis while tuberculosis cannot be treated adequately in view of severe liver disease. Patients usually cannot wait for the tuberculosis treatment to be completed considering overall poor prognosis of advanced liver disease. There is scanty literature published on treatment of tuberculosis in such select group of patients. Most literature is on patients with early or Child-Turcotte-Pugh (CTP) B cirrhosis. There is no literature on treating CTP C patients diagnosed and treated when they were being evaluated for liver transplant. We report here 5 cases of tuberculosis diagnosed during pre- transplant evaluation.
Case Report
Case 1
45 year old male patient presented to us with end stage liver disease caused by alcohol. He was referred to our center for evaluation of liver transplant. At presentation he had jaundice, refractory ascites, hyponatremia, muscle wasting, coagulopathy and hypoalbuminemia. He had previously undergone multiple time band ligations for esophageal varies over a period of 18 months. He was abstinent from alcohol for 18 months before presentation. He had bilirubin 8.3 mg/dl, ALT 28 IU/ml, AST 65 IU/ml, Serum Albumin 21 gram/dl, International ratio (INR) 2.89, Serum Creatinine 0.65 mg/dl, Serum Sodium 128 mg/dl. He did not have overt encephalopathy. He was evaluated for liver transplant. During his evaluation his chest x-ray showed bilateral mild pleural effusion. His diagnostic ascitic fluid tap showed protein 2 grams, SAAG > 1.1, 620 cells with lymphocytes 90 percent, ADA 2, MTB Genxpert® [3] negative and negative AFB culture. In view of high protein high SAAG ascites, he underwent a pleural tap which also showed negative AFB culture, negative MTB GenXpert®, negative ADA and protein of 2.6 grams. Our pulmonologist went ahead with bronchoscopy which was normal but broncheo-alveolar lavage was positive for AFB and MTB GenXpert was positive for Rifampicin sensitive mycobacterium tuberculosis. As per guidelines neither of Rifampicin and Isoniazid was given to the patient. He was started on ethambutol, moxifloxacin, clofazamine and cycloserine. His transplant was postponed. On starting anti tuberculosis treatment and naso gastric feeds, he started improving symptomatically. His pleural effusion on chest x-ray improved and even ascites decreased. Four weeks after starting treatment, he developed sudden onset breathlessness and was admitted with severe metabolic acidosis (pH - 6.8). He was resuscitated, intubated and started on renal replacement therapy. He was given carbapenem, azole and teicoplanin. He died 12 hours later. His blood culture reports came positive 3 days later showing extensive resistant Klebsiella Pneumonia showing sensitivity only to colistin/polymyxin B.
Case 2
A 37 year old male with alcohol related cirrhosis of liver diagnosed recently was transferred under our care from an outside hospital in view of worsening dyspnea for considering an urgent liver transplant. At presentation he had history of worsening jaundice for 4 weeks, abdominal distension and pedal edema for 2 weeks and breathlessness for 7 days. He had pallor, icterus, anasarca and absent air entry on left side with an intercostal drain (ICD) placed draining blood. He did not have encephalopathy and was passing good urine. He had undergone ICD insertion outside after requiring daily taps for pleural effusion outside 2 days before presentation. The initial pleural fluid reports were showing transudative picture. However, after he bled on ICD insertion it contained red blood cells > 50,000. His Hb was 6.9 gm/ dl, white cell count 12,000 per cumm, platelets 45,000 per cumm, Bilirubin 5.2 mg/dl, albumin 2.8 gram/dl, INR 2.24, Creatinine 1.45 mg/dl, Sodium 139 mEq/L and Fibrinogen 98 mg/dl. His chest x-ray showed massive left sided effusion with collapse. Local ultrasound revealed hemorrhagic content in the chest and septations. He was started on antibiotics, albumin, nasogastric feeds, multivitamins and coagulopathy correction based on thromboelastography. On third day the ICD got blocked and was removed. The pleural fluid sample was aspirated which showed AFB negative, ADA 18, MTB GenXpert® Negative, 580 cells with lymphocytes predominant, Protein 1.2 grams/L, Albumin 0.4 grams/L. His fluid was sent for AFP culture. His symptoms improved over a week and he was discharged on nasogastric feeds for high calorie high protein diet. He presented again after 8 days with a fistula arising from left side of chest, a site different from the ICD insertion site. The fistula on local ultrasound was communicating with pleural cavity. He denied consent for repeat ICD insertion or pleural tap and so a local fistula closure was done under general anesthesia and sample from fistula was sent for tuberculosis screening. This time it showed AFB negativity but MTB GenXpert® AFB positivity and so was started on Ethambutol and Moxifloxacin. Two months after starting his 2 drug ATT, his pleural effusion and fistula has completely resolved with only minimal pleural thickening remaining on chest x-ray. His ascites and pedal edema has disappeared and liver tests have normalized. His
liver has compensated (Bilirubin 1.2 mg/dl, albumin 3.9 g/ dl, sodium 140 mEq/L, INR 1.01, no ascites on ultrasound) and was started on Rifampicin initially and isoniazid later on. His pleural fluid AFB cultures have turned out to be negative. His transplant evaluation has been on hold and is not on transplant list.
Case 3
A 51 year old male diagnosed to have alcohol related liver disease for 3 years had started worsening over the last 3 months and was referred for evaluation for liver transplant. He had been symptom free and abstinent from the time of diagnosis. He had portal hypertension (HT) manifesting as varies and was started on beta blockers as primary prophylaxis. Over previous 3 months he had development of refractory ascites, edema and significant loss of muscle mass. He had developed loss of appetite but denied any fever, jaundice, decreased urine output or an episode suggestive of encephalopathy. At presentation his reports showed hemoglobin 11 g/dl, platelets 120 per cumm, bilirubin 2.4 mg/dl (conjugated 0.1 mg/dl), albumin 2.6 grams/dl, INR 1.91, creatinine 0.7 mg/dl and sodium 136mEq/L. His ascites was high SAAG and negative for tuberculosis workup. He had isolated minimal right sided effusion and had undergone a tap outside 15 days before presentation which corroborative of hepatic hydrothorax. He was started on liver transplant evaluation and pulmonologist advised a repeat tap of pleural effusion before clearance. He underwent a repeat tap of right sided pleural effusion which showed cell count of 879 with lymphocyte predominant, protein 4 grams, Albumin 2.3 grams, ADA 81, AFB negative and MTB GenXpert® negative. Considering this picture, he was started on anti-tuberculosis therapy (ATT) - Rifampicin, Ethambutol and Moxifloxacin. Within 4 weeks of starting treatment, his ascites improved and edema disappeared. His appetite improved and even liver tests normalized. Isoniazid was added 8 weeks after starting ATT and has completed 12 months of therapy. He is asymptomatic currently. He is not evaluated for transplant.
Case 4
A 48 year old male patient with diagnosis of alcohol related liver disease was referred to us for non-resolving right sided hepatic hydrothorax with refractory ascites. At presentation he was breathless. He had icterus, pallor, anasarca, tense ascites and absent air entry on right side with a respiratory rate of 30 per minute. His last tap was 48 hours before. His previous ascetic and pleural tap reports were negative. His chest x-ray showed hemithorax right sided opacity. With coagulopathy correction based on thromboelastography, he underwent an indwelling pleural catheter insertion and pleural fluid reports were repeated. An HRCT thorax was carried out which showed consolidation in left basal area. The pulmonologist advised a bronchoscopy which revealed MTB GenXpert positive broncheo-alveolar lavage. The patient was started on Ethambutol and Moxifloxacin. He was re admitted 7 days later with decreased urine output. He was diagnosed with urinary tract infection with sepsis. He developed progressive multi organ dysfunction over next 4 days and died. His culture showed Klebsiella Pneumonia sensitive only to polymyxin and colistin.
Case 5
A 61 year old male with ethanol related cirrhosis was referred to our center for requiring repeated ascitic taps. He had history of developing encephalopathy on multiple occasions but had no history of hematemesis. At admission he was sarcopenic with ascites out of proportion to edema and had severe muscle wasting. His reports showed bilirubin 3.1 mg/dl, INR 2.14, serum creatinine 1.28, serum albumin 3.2 and serum sodium 140mEq/L. On admission his ascetic tap was sent which was high SAAG high protein ascites with lymphocyte predominant cellularity. It was negative for MTB GenXpert, ADA and AFB staining. However, the ascetic fluid culture grew MTB at 20 days. The patient was started on Ethambutol and Levofloxacin. The Table 1 mentions the summary of all 5 patients.
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | |
|---|---|---|---|---|---|
| Age (in years) | 45 | 37 | 51 | 48 | 61 |
| Gender | Male | Male | Male | Male | Male |
| Etiology of Liver disease | Ethanol | Ethanol | Ethanol | Ethanol | Ethanol |
| Bilirubin (mg/dl) | 8.3 | 5.2 | 2.4 | 13 | 3.1 |
| INR | 2.89 | 2.24 | 1.91 | 3.25 | 2.14 |
| Creatinine (mg/dl) | 0.65 | 1.45 | 0.7 | 1.1 | 1.28 |
| Albumin (g/dl) | 21 | 28 | 26 | 19 | 32 |
| Sodium (mEq/L) | 128 | 139 | 136 | 130 | 140 |
| MELD Sodium | 30 | 25 | 18 | 32 | 22 |
| CTP class | C | C | C | C | C |
| Ascitic cell clount | 620 | 90 | 65 | 225 | 1287 |
| Ascitic Protein (in grams) | 2 | 0.4 | 0.7 | 0.2 | 3.8 |
| Ascitic ADA | 2 | <1 | 8 | <1 | 21 |
| Ascitic MTB GenXpert | Negative | Negative | Negative | Negative | Negative |
| Pleural Protein | 2.6 | 1.2 | 4 | 2.4 | - |
| Pleural cell count | 839 | 580 | 879 | 110 | - |
| Pleural ADA | 12 | 18 | 81 | 12 | - |
| Pleural Fluid MTB GenXpert | Negative | Negative | Negative | Negative | - |
| Fluid Culture | Negative | Negative | Negative | Negative | Positive |
| Diagnostic test | Bronchoscopy with lavage | Pleuro cutaneous fistula | Pleural Fluid | Bronchoscopy with lavage | Culture |
| Site of tuberculosis | Pulmonary | Pleural | Pleural | Pulmonary | Peritoneal |
| Treatment | E+ Q+ Clofazamine+ Cycloserine | E+ Q, R+H added later on | E+ Q, H added later on | E+ Q | E+ Q, H added later on |
| Outcome | Died due to sepsis | Alive | Alive | Died due to sepsis | Alive |
| Transplant | Not done | On Hold | On Hold | Not done | On Hold |
Table 1: The summary of all 5 patients with tuberculosis. INR: International Normalized Ratio, MELD: Model for End Stage Liver Di
Discussion
This case series stresses on the fact that tuberculosis in cirrhosis is not just a diagnostic dilemma but also a therapeutic dilemma. The patients who are sent for liver transplant are routinely evaluated by all specialties and hence provide a unique opportunity to diagnose tuberculosis.
Prevalence
Tuberculosis and cirrhosis both are widely prevalent in India and other south Asian countries. Though data of tuberculosis in transplant evaluated patients is scanty, there is data on tuberculosis in cirrhosis in general. In a Taiwanese nationwide longitudinal study including 41,076 cirrhotic patients and 204,244 non-cirrhotic controls from 1998 through 2007, a total of 957 (2.32%) cirrhotic patients developed TB, yielding a rate that was significantly higher than that of the 955 (0.46%) non-cirrhotic patients (P < 0.001) [4]. In a retrospective database published from Nepal [5], tuberculosis prevalence in cirrhosis was 9% while it was 7.38% in a study from western India [6]. In a Danish study cohort of 22675 patients with liver cirrhosis, they identified 151 cases of tuberculosis from 1977 to 1993 with an incidence of 168.6 per 100000 person-years and 30-day case-fatality rate was 27.3% [7].
Prognosis
In our case series 2 patients died with complications of cirrhosis leading to a case fatality rate of 40 percent. In a study which looked at mortality of patients with cirrhosis and tuberculosis, 0-day, 90-day, 1-year and 3-year mortalities were 10.1%, 24.2%, 43.1%, and 63% in the TB group and the hazard ratios (HR) in cirrhotic patients with TB for 30-day, 30 to 90-day, 90-day to 1-year, and 1 to 3-year mortalities were 1.33, 1.91, 1.46, and 1.10 compared to the non-TB group respectively [8]. This study however does not mention about the severity of underlying disease. In a Japanese study, 18/44 patients with cirrhosis and tuberculosis died with liver disease. The severity of cirrhosis was not mentioned even in this study [9].
Risk factors
In our case series all the patients suffered from ethanol related cirrhosis of liver. In previous study, alcoholism and hepatitis C infection were associated with significantly higher TB risk with adjust hazard ratios of 2.184. Alcoholism was also the most common etiology of liver disease (60%) in the study from western India [6]. In a study from Northern India, the etiologies of cirrhosis of liver were: alcohol in 49% cases; the others being post viral infection (23%), cryptogenic (16%) and NASH (12%) [10]. In a Chinese case control study, Hepatitis B was the underlying etiology in 44% patients while ethanol was responsible for 22% cases [11].
Site
In our series, 2/5 (40%) had pulmonary tuberculosis. Even in Nepalese study, extra pulmonary tuberculosis was more common (67%) than pulmonary (33%). In extra pulmonary tuberculosis, distribution was as pleural effusion, abdominal, intestinal, peritoneal, and spine [5]. In the study by Amarapurkar, et al. [6], 40% had pulmonary tuberculosis while other sites involved were pleural in 28%, peritoneal 18%, cervical node 6%, liver 4%, intestine 2% and spine was 2%. As per the Taiwanese database4, 80.0% had pulmonary TB, 0.9% had military TB, 16.6% had extrapulmonary TB and 2.5% had both pulmonary and extrapulmonary TB. In a study from Northern India [10], site of tuberculosis was pulmonary (37%), pleural effusion (16%), peritoneal (29%), lymph nodes (4%), liver (1.5%), intestines (4%), bone (4%), brain (1.5%) and disseminated (3%).primary carried out to look at outcomes of drug induced liver injury with ATT in cirrhosis included 67 patients, of which 16 were belonging to CTP C category.
Diagnosis
In all our patients, tuberculosis diagnosis was not straight forward. The tests were negative at the first instance and only on repeated analysis they turned out to be positive. This is very important as a single negative sample should not exclude tuberculosis in these patients. The clinical presentations of low grade fever, muscle loss, loss of appetite are routinely seen in patients with end stage liver disease and may be symptoms of cirrhosis or tuberculosis [10]. So the diagnosis is mainly based on investigations and high clinical suspicion. Tuberculosis peritonitis can simulate ascites from liver disease or spontaneous bacterial peritonitis. The diagnosis is difficult in these patients because the ascitic fluid may not be of the exudative type as a result of the low albumin level in serum, and lymphocytes do not predominate in all cases. The time required to achieve a correct diagnosis was significantly longer in cirrhotic than in non-cirrhotic patients [12]. In a study to differentiate spontaneous bacterial peritonitis (SBP) from tuberculosis peritonitis (TP), TP in cirrhotic patients was more frequently associated with extra-peritoneal tuberculosis (53.3%), an insidious onset (≥2 weeks in 60%) and advanced liver disease (CTP B in 80%) while, TP showed lower white blood cell count in ascites, higher protein concentration and higher adenosine deaminase activity in ascites [13]. The utility of ADA from peritoneal fluid in cirrhosis has been questioned although. In a US study, the overall sensitivity of the ADA determination in diagnosing tuberculosis peritonitis was only 58.8%, and the specificity was 95.4% and was only 30% sensitive in detecting TP in the setting of cirrhosis. In addition, malignancy-related ascites (13%) and bacterial peritonitis specimens (5.8%) yielded false-positive results [14]. In a Taiwanese study, a 27 U/L as the cut-off value of ADA on the contrary, showed sensitivity and specificity of 100% and 93.3%, respectively to differentiate TP in cirrhosis [15] which is similar to patients without cirrhosis [16, 17]. Limited data are available to support the use of GeneXpert MTB in the diagnosis of abdominal tuberculosis. In our series 3 of 5 patients had GenXpert MTB positive (one in tissue culture from cutaneous fistula and two from Bronchoalveolar Lavage). None of the patients had peritoneal or pleural fluid report positive. Data are also not favoring use of MTB GenXpert in these patients with a study from Pakistan having 0% specificity for the test [18]. The studies from India have found a sensitivity of 8 to 32% for intestinal tuberculosis [19, 20, 21]. A Cochrane review also found that sensitivity of the test varied as per tissue sample, the highest sensitivity in urine, bone and joint while for pleural fluid it was just 31% [22]. Mantoux or interferon gamma release assays (IGRA) were not carried out in our patients. The interpretation of Mantoux test in cirrhosis is difficult. Besides, almost all Indians are vaccinated with tuberculin. Published Indian literature also states that there is no role of Mantoux testing before liver transplant while the utility of IGRA is not established as compared to west [23, 24, 25]. The diagnosis in the study from western India6 was based on histopathology or fluid analysis in 60% cases. Remaining 40% were considered tuberculosis based on clinical and radiological parameters. In the study from Northern India, Mantoux was positive in only 43% patients with CTP C cirrhosis compared to more than 70% with CTP A and CTP B cirrhosis. 59/67 patients had TB confirmed histopathologically [10]. In our series as well, 80% diagnosis was made from tissue sample and only one patient was diagnosed on biochemical and radiological parameters.
Treatment
We treated all patients with Ethambutol and Quinolone. Aminoglycosides were not given considering the risk of acute kidney injury. One patient was given cycloserine. Isoniazid was added once the clinical parameters improved to CTP B state. Isoniazid was initially given at dose of 150 mg and then increased to 300 mg after 15 days. Weekly monitoring was carried out. Rifampicin was added later in one patient in step wise manner. Dhiman, et al. [26] recommends the following management guidelines for tuberculosis in patients of cirrhosis - ATT should include no more than 2 hepatotoxic drugs (Rifampicin (R) and Isoniazid
(H)) in patients with CLD or liver cirrhosis and stable liver function (CTP ≤7), only a single hepatotoxic drug (R or H) in those with advanced liver dysfunction (CTP 8-10) and no hepatotoxic drugs with very advanced liver dysfunction (CTP ≥11). The duration of therapy is for 18-24 months. However, as per study by Sharma et al. they have used R+H for first two months in 2 patients with CTP C cirrhosis along with Ethambutol (E) and Quinolones (Q). They used Rifampicin without isoniazid in 7 patients while used Isoniazid without rifampicin in 2 patients. Of 16 patients treated with CTP C cirrhosis, the mortality was 25% and both patients with R+H use developed liver injury. Drug induced toxicity was seen in 35% patients in patients started with RHEQ, HEQ and REQ. Saigal, et al, in their study comparing Pyrizinamide (Z) with R+H in patients of cirrhosis have shown that R+H is more hepatotoxic than a combination with Q+Z [27]. The previous Indian study published treated 14 patients with E+Q with or without aminoglycosides and clarithromycin6. However, the selective outcome of these patients in CTP C patients was not mentioned, although four patients died of liver related complications from an entire cohort of 50 patients. In a Chinese study [11], only 57% of total patients completed full course of treatment and 7/36 patients had CTP C cirrhosis. Six of patients with CTP C cirrhosis died due to progression of liver disease. None of them received R or H. In an interesting case series published of 3 patients, all 3 patients were given Isoniazid based therapy, one patient getting transplanted 1 month after starting treatment while one patient was started anti tuberculosis treatment (ATT) after transplant. One patient deteriorated 6 months after full dose of ATT [28].
Liver Transplant
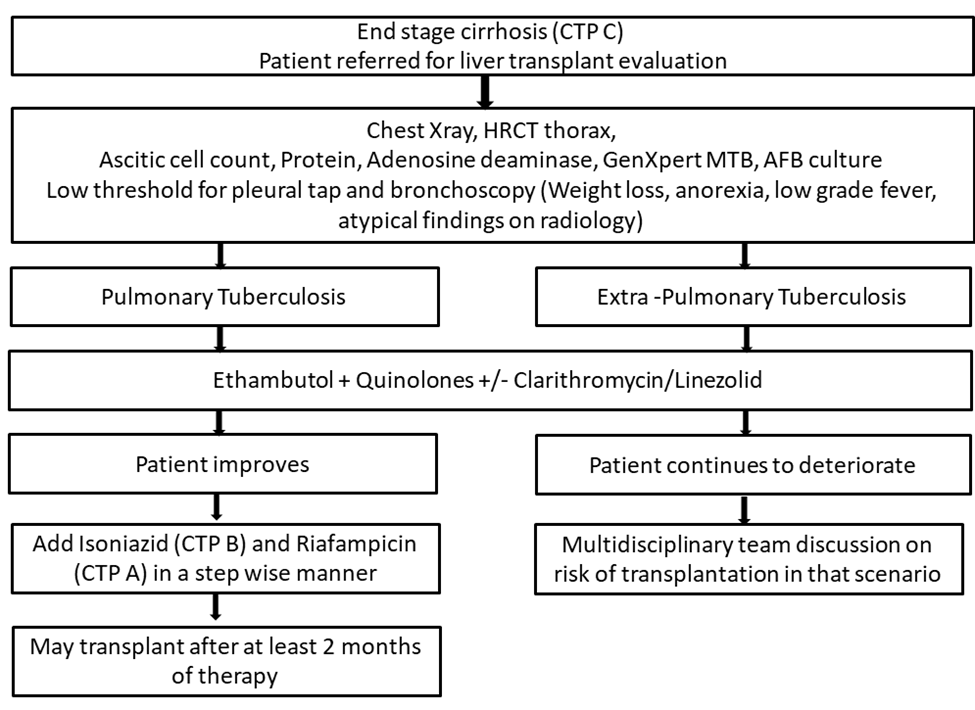
In our series, none of the patient was transplanted after the diagnosis. The two patients died within short period of starting therapy. The remaining patients improved with therapy so much as to take them off the transplant list. For patients treated with R +H, it is usually considered safe to transplant after the intensive therapy. However, when patient is just taking E+Q, the timing for transplant is not known. At the same time, delaying transplants in very sick cirrhotic patients can lead to poor outcome. Further research is needed in optimizing the timing of these patients. Although, in a published Chinese case series [11], the patient was transplanted and then ATT was started, from our series we can see that some patients may have dramatic improvement and may no longer require the transplant. The comparative evaluation of ATT by different groups is shown in Table 2. The management of Tuberculosis as proposed by our team is mentioned in Figure 1.
| Our Series | Baijal, et al. [6] | Sharma, et al. [5] | Sharma, et al. [10] | Cho, et al. [11] | Wang, et al. [28] | |
|---|---|---|---|---|---|---|
| Total patients | 5 | 50 | 18 | 67 | 36 | 3 |
| Number of patients with CTP C Cirrhosis | 5 | - | 8 | 16 | 7 | 2 |
| Mean Age (in years) | 48.4 | 46.8 | 53 | 52 | 63 | 42 |
| Male | 100% | 92% | 67% | 85% | 89% | 67% |
| Alcohol Related liver disease | 100% | 60% | 52% | 22% | 0% | |
| Mean Bilirubin (mg/dl) | 6.4 | - | - | 4.8 | - | |
| Mean INR | 2.4 | - | - | 1.8 | - | |
| Mean serum creatinine (mg/dl) | 1.03 | - | - | - | ||
| Mean serum albumin (g/dl) | 25.2 | - | - | - | ||
| Sodium (mEq/L) | 134 | - | - | - | ||
| Mean MELD Sodium | 25 | - | - | - | ||
| Pulmonary tuberculosis | 40% | 40% | 33% | 37% | 69% | 33% |
| Extra pulmonary tuberculosis | 60% | 60% | 67% | 63% | 31% | 67% |
| Diagnostic Modality | 80% tissue based | 88% tissue based | 95% tissue based | 100% tissue based | ||
| Treatment in CTP C cirrhosis (Number of patients) | EQ based | HRZES (35) | REQ(7) | - | HEQS (1) | |
| EQ (14) | RHE(2) | |||||
| HRZESQ+ Cl (1) | HEQ(2) | |||||
| EQ(5) | ||||||
| Patients on Isoniazid | 60% | - | - | 25% | - | 50% |
| Patients on Rifampicin | 20% | - | - | 56% | - | - |
| Duration | 12-18 months | 18-Jun | 9-18 months | 12 months | 12 months | |
| Survival | 60% | 92% | 25% in CTP C | 85% in CTP C | 100% | |
| Transplant | Nil | - | - | - | 1* |
Table 2: The management of Tuberculosis as proposed by our team is mentioned in Figure 1.
Conclusion
To conclude, tuberculosis is not uncommon in patients being evaluated for liver transplant. Tuberculosis in itself can lead to development of worsening liver function. The diagnosis of tuberculosis requires repeating the tests multiple times. No single test is adequate and often requires battery of investigations if index of suspicion is high. Extra pulmonary tuberculosis is more common and history of alcoholism is a risk factor for development of tuberculosis in these patients of advanced liver disease. The treatment of tuberculosis and timing of transplant are not defined and needs further studies to define the best treatment strategy and timing for transplant.
References
-
World Health Organization (2018) Global Tuberculosis Report 2018- Executive Summary, pp: 266.
-
Soediono B (2019) Global Tuberculosis Report 2012. World Health Organization.
-
Rasool G, Khan AM, Din RMU, Riaz M (2019) Detection of mycobacterium tuberculosis in afb smear-negative sputum specimens through MTB culture and GeneXpert® MTB/RIF assay. Int J Immunopathol Pharmacol 33: 2058738419827174.
-
Lin YT, Wu PH, Lin CY, Lin MY, Chuang HY, et al. (2014) Cirrhosis as a risk factor for tuberculosis infection - A nationwide longitudinal study in Taiwan. Am J Epidemiol 180(1): 103-110.
-
Sharma D, Kc S, Jaisi B (2018) Prevalence of Tuberculosis in Patients with Liver Cirrhosis. J Nepal Health Res Counc 15(3): 264-267.
-
Baijal R, Praveenkumar HR, Amarapurkar DN, Nagaraj K, Jain M (2010) Prevalence of tuberculosis in patients with cirrhosis of liver in western India. Trop Doct 40(3): 163-164.
-
Thulstrup AM, Molle I, Svendsen N, Sorensen HT (2000) Incidence and prognosis of tuberculosis in patients with cirrhosis of the liver: A Danish nationwide population based study. Epidemiol Infect 124(2): 221-225.
-
Hung TH, Lay CJ, Tseng CW, Tsai CC, Tsai CC (2014) The effect of tuberculosis on the mortality of cirrhotic patients: A population-based 3-year follow-up study. Medicine (Baltimore) 93(28): e295.
-
Saito A, Nagayama N, Yagi O, Ohshima N, Tamuraet A, et al. (2006) Tuberculosis complicated with liver cirrhosis. Kekkaku 81(7): 457-465.
-
Sharma P, Tyagi P, Singla V, Bansal N, Kumar A, et al. (2015) Clinical and biochemical profile of tuberculosis in patients with liver cirrhosis. J Clin Exp Hepatol 5(1): 8-13.
-
Cho YJ, Lee SM, Yoo CG, Kim YW, Han SK, et al. (2007) Clinical characteristics of tuberculosis in patients with liver cirrhosis. Respirology 12(3): 401-405.
-
Aguado JM, Pons F, Casafont F, Miguel GS, Valle R (1990) Tuberculous peritonitis: A study comparing cirrhotic and noncirrhotic patients. J Clin Gastroenterol 12(5): 550-554.
-
Kim NJ, Choo EJ, Kwak YG, Lee SO, Choi SH, et al. (2009) Tuberculous peritonitis in cirrhotic patients: Comparison of spontaneous bacterial peritonitis caused by Escherichia coli with tuberculosis peritonitis. Scand J Infect Dis. 41(11-12): 852-856.
-
Hillebrand DJ, Runyon BA, Yasmineh WG, Rynders GP (1996) Ascitic fluid adenosine deaminase insensitivity in detecting tuberculosis peritonitis in the United States. Hepatology 24(6): 1408-1412.
-
Liao YJ, Wu CY, Lee SW, Lee CL, Yanget SS, et al. (2012) Adenosine deaminase activity in tuberculosis peritonitis among patients with underlying liver cirrhosis. World J Gastroenterol 18(37): 5260-5265.
-
Bhargava DK, Gupta M, Nijhawan S, Dasarathy S, Kushwaha AKS (1990) Adenosine deaminase (ADA) in peritoneal tuberculosis: Diagnostic value in ascitic fluid and serum. Tubercle 71(2): 121-126.
-
Riquelme A, Calvo M, Salech F, Valderrama S, Pattillo A, et al. (2006) Value of adenosine deaminase (ADA) in ascitic fluid for the diagnosis of tuberculosis peritonitis: A meta-analysis. J Clin Gastroenterol 40(8): 705-710.
-
Ahmad R, Changeez M, Khan JS, Qureshi U, Tariq M, et al. (2018) Diagnostic Accuracy of Peritoneal Fluid GeneXpert in the Diagnosis of Intestinal Tuberculosis, Keeping Histopathology as the Gold Standard. Cureus 10(10).
-
Udgirkar S, Jain S, Pawar S, Chandnani S, Contractor Q, et al. (2019) Clinical profile, drug resistance pattern and treatment outcomes of abdominal tuberculosis patients in western India. Arq Gastroenterol 56(2): 178-183.
-
Kumar S, Bopanna S, Kedia S, Mouli P, Dhingra R, et al. (2017) Evaluation of Xpert MTB/RIF assay performance in the diagnosis of abdominal tuberculosis. Intest Res 15(2): 187-194.
-
Bellam BL, Mandavdhare HS, Sharma K, Shukla S, Soni H, et al. (2019) Utility of tissue Xpert-Mtb/Rif for the diagnosis of intestinal tuberculosis in patients with ileocolonic ulcers. Ther Adv Infect Dis 6: 204993611986393.
-
Kohli M, Schiller I, Dendukuri N, Dheda K, Denkinger CM, et al. (2018) Xpert® MTB/RIF assay for extrapulmonary tuberculosis and rifampicin resistance. Cochrane Database Syst Rev 8(8): CD012768.
-
Rajagopala S, Olithselvan A, Varghese J, Shanmugam N, Rela M (2011) Latent Mycobacterium tuberculosis Infection in liver transplant recipients-Controversies in current diagnosis and management. J Clin Exp Hepatol 1(1): 34-37.
-
Holty JEC, Gould MK, Meinke L, Keeffe EB, Ruoss SJ (2009) Tuberculosis in liver transplant recipients: A systematic review and meta-analysis of individual patient data. Liver Transplant 15(8): 894-906.
-
Sharma SK, Mohanan S, Sharma A (2012) Relevance of latent TB infection in areas of high TB prevalence. Chest 142(3): 761-773.
-
Dhiman RK, Saraswat VA, Rajekar H, Reddy C, Chawla YK (2012) A Guide to the Management of Tuberculosis in Patients with Chronic Liver Disease. J Clin Exp Hepatol 2(3): 260-270.
-
Saigal S, Agarwal SR, Nandeesh HP, Sarin SK (2001) Safety of an ofloxacin-based antitubercular regimen for the treatment of tuberculosis in patients with underlying chronic liver disease: A preliminary report. J Gastroenterol Hepatol 16(9): 1028-1032.
-
Wang B, Lu Y, Yu L, Liu C, Liu X, et al. (2009) Liver transplantation for patients with pulmonary tuberculosis. Transpl Infect Dis 11(2): 128-131.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient